Surgical Management of Extremity Soft Tissue Sarcomas: Principles of Wide Resection and Limb Salvage
Key Takeaway
The surgical management of extremity soft tissue sarcomas demands a multidisciplinary approach, integrating neoadjuvant radiotherapy with precise wide local excision. Limb-salvage surgery relies on achieving negative microscopic margins while preserving neurovascular structures. This guide details the critical steps of preoperative imaging, biopsy tract management, and en bloc resection, ensuring optimal oncologic and functional outcomes for orthopedic oncology patients.
Introduction to Extremity Soft Tissue Sarcomas
The evolution of orthopedic oncology has witnessed a paradigm shift from radical amputations to sophisticated limb-salvage procedures for the treatment of extremity soft tissue sarcomas (STS). This transformation is underpinned by advancements in advanced cross-sectional imaging, the strategic application of neoadjuvant radiotherapy, and a refined understanding of compartmental anatomy.
Soft tissue sarcomas are a heterogeneous group of mesenchymal malignancies. While histologies vary widely—ranging from pleomorphic undifferentiated sarcoma and liposarcoma to rarer entities such as extraskeletal myxoid chondrosarcoma and epithelioid sarcoma—the fundamental surgical principles remain uniform. The primary objective is the complete eradication of the tumor with negative microscopic margins (R0 resection) while maximizing the functional preservation of the affected limb.
This comprehensive guide delineates the evidence-based protocols for the evaluation, neoadjuvant management, and surgical resection of extremity soft tissue sarcomas, utilizing a documented case of extraskeletal myxoid chondrosarcoma to illustrate critical operative tenets.
Preoperative Evaluation and Imaging
Accurate staging and anatomic mapping are the cornerstones of successful limb-salvage surgery. Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the local extent of a soft tissue sarcoma.
The Role of Magnetic Resonance Imaging (MRI)
MRI provides unparalleled soft-tissue contrast, allowing the surgeon to delineate the tumor's relationship to major neurovascular bundles, fascial planes, and adjacent osseous structures. Standard protocols must include T1-weighted, T2-weighted, and gadolinium-enhanced sequences in axial, coronal, and sagittal planes.
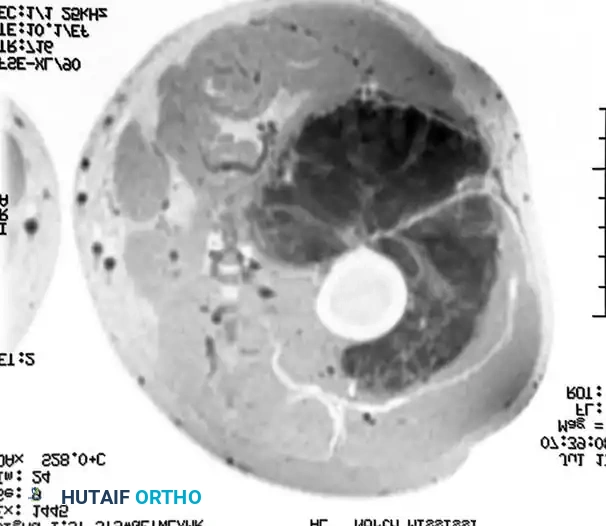
Figure 1: Axial MRI demonstrating a large, lobulated soft-tissue mass within the musculature of the thigh. The heterogeneous signal intensity and lobulated architecture are characteristic of an extraskeletal myxoid chondrosarcoma prior to therapeutic intervention.
Clinical Pearl: Always evaluate the entire length of the involved compartment on MRI to rule out "skip" metastases or proximal/distal fascial extension that could compromise the planned surgical margins.
Systemic Staging
Following local imaging, systemic staging is mandatory to rule out distant metastasis, which most commonly occurs in the lungs. High-resolution Computed Tomography (CT) of the chest is the standard of care. In specific histologies with a propensity for lymphatic spread (e.g., epithelioid sarcoma, synovial sarcoma, clear cell sarcoma, rhabdomyosarcoma, and angiosarcoma), regional lymph node evaluation via ultrasound or PET-CT is indicated.
Neoadjuvant Therapy: Biomechanical and Surgical Implications
The integration of neoadjuvant (preoperative) radiation therapy has revolutionized the surgical approach to high-grade soft tissue sarcomas. Administering radiation prior to surgery offers several distinct advantages over postoperative radiation:
- Tumor Downstaging: Radiation induces tumor necrosis, often leading to a reduction in tumor volume.
- Pseudocapsule Maturation: Radiation thickens the reactive zone (pseudocapsule) surrounding the tumor. This fibrotic transformation provides a more robust physical barrier during surgical dissection, reducing the risk of intraoperative tumor spillage.
- Lower Radiation Doses: Preoperative fields are smaller, and the required dose (typically 50 Gy) is lower than postoperative doses (60-66 Gy), which reduces long-term tissue fibrosis and joint stiffness.
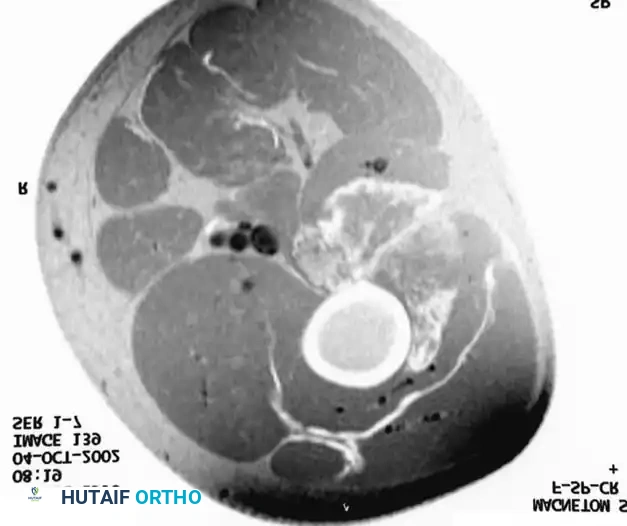
Figure 2: Axial MRI of the same patient following a full course of preoperative radiation therapy. Note the dramatic decrease in the size of the mass and the increased definition of the surrounding tissue planes. This radiologic response makes the subsequent wide resection technically much easier and oncologically safer.
Surgical Warning: While neoadjuvant radiation facilitates easier resection, it significantly increases the risk of postoperative wound complications (up to 30-35%). Meticulous soft-tissue handling, the avoidance of extensive undermining, and the liberal use of vascularized tissue transfers (e.g., rotational or free flaps) are critical to mitigating wound dehiscence.
Principles of Biopsy in Orthopedic Oncology
The biopsy is the most critical initial step in the management of a suspected sarcoma. A poorly planned biopsy can preclude limb salvage and necessitate amputation.
Core Needle vs. Open Biopsy
Image-guided core needle biopsy (multiple passes with a 14-gauge needle) is preferred due to its high diagnostic yield and minimal contamination of surrounding tissues. If an open incisional biopsy is required, strict adherence to the following rules is mandatory:
- Longitudinal Incisions Only: Transverse incisions contaminate multiple lymphatic and fascial planes and are nearly impossible to excise en bloc during definitive surgery.
- Direct Approach: Traverse the minimum amount of normal tissue. Do not cross un-involved compartments.
- Meticulous Hemostasis: Post-biopsy hematomas disseminate tumor cells far beyond the primary site, expanding the required volume of definitive resection.
- Tourniquet Use: If a tourniquet is used during an open biopsy, the limb must be elevated for exsanguination; never use an Esmarch bandage, as the compressive forces can milk tumor cells into the systemic circulation.
Step-by-Step Surgical Approach: Wide Local Excision
The goal of a wide local excision is to remove the tumor entirely within an envelope of normal, healthy tissue. The dissection plane must never breach the tumor's pseudocapsule.
1. Patient Positioning and Preparation
- Positioning: The patient is positioned to allow circumferential access to the extremity. For thigh lesions, the patient is typically supine with a bump under the ipsilateral hip.
- Tourniquet: A sterile tourniquet is applied proximally. As with the biopsy, exsanguination is achieved via elevation, not compression. The tourniquet is often left uninflated unless catastrophic hemorrhage occurs, as visualizing bleeding vessels aids in identifying the reactive zone and ensuring viable margins.
2. Incision and Biopsy Tract Isolation
- An elliptical incision is designed to incorporate the previous biopsy tract, the biopsy skin entry point, and any associated tattooing.
- A minimum margin of 1 to 2 cm of normal skin surrounding the biopsy tract is excised.
- The skin flaps are raised at the level of the deep fascia. Flap thickness must be maintained to ensure adequate vascularity, especially in irradiated fields.
3. Compartmental Dissection and Margin Acquisition
- Fascial Incision: The deep fascia is incised longitudinally, well away from the palpable extent of the tumor.
- Muscle Resection: The dissection proceeds through normal muscle tissue. The surgeon must maintain a continuous cuff of normal muscle (typically 1-2 cm) around the tumor.
- Anatomic Barriers: Natural anatomic barriers, such as major fascial septa, the periosteum, and the epineurium of major nerves, can serve as adequate margins even if the physical distance is less than 1 cm. If the tumor abuts the bone without invasion, subperiosteal dissection is acceptable. If the periosteum is invaded, en bloc cortical resection or segmental bone resection is required.
4. Neurovascular Dissection
- Major neurovascular bundles (e.g., the superficial femoral artery or sciatic nerve) are identified proximal and distal to the tumor mass in normal, unscarred tissue.
- Dissection proceeds toward the tumor. If the tumor is adherent to the adventitia of the vessel or the epineurium of the nerve, an adventitial or epineurial dissection (epiperineurial margin) may be attempted to salvage the limb.
- If the nerve or vessel is directly invaded, it must be resected en bloc with the tumor. Vascular reconstruction with reversed saphenous vein grafts or synthetic conduits is performed immediately.
5. En Bloc Delivery of the Specimen
- The tumor is mobilized circumferentially. The deep margin is often the most challenging to visualize and requires meticulous retraction.
- The specimen is delivered en bloc, ensuring the biopsy tract remains attached to the main tumor mass without disruption.
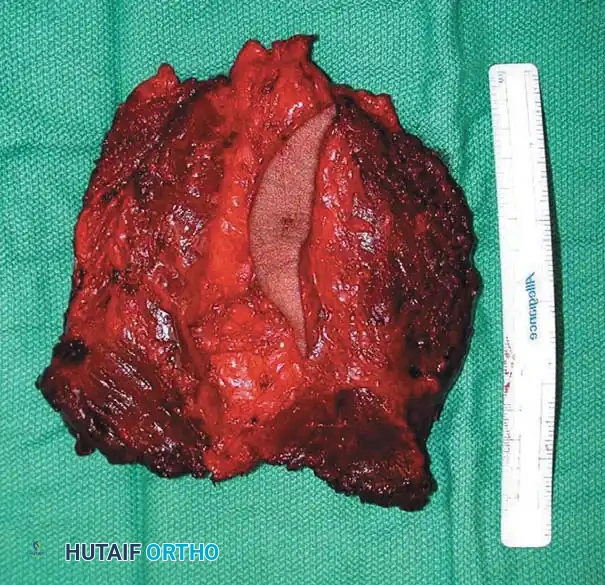
Figure 3: Photograph of the gross specimen following wide resection. The elliptical skin island containing the biopsy tract has been resected en bloc with the underlying tumor. The plane of dissection is entirely through normal, healthy muscle tissue, ensuring negative oncologic margins.
6. Specimen Orientation and Closure
- The excised specimen is oriented with sutures or surgical clips (e.g., short stitch superior, long stitch lateral) to guide the pathologist in evaluating the margins.
- The tumor bed is copiously irrigated with sterile saline.
- Hemostasis is achieved. Closed suction drains are placed in the dependent portion of the wound, exiting through separate stab incisions in line with the primary incision.
- Closure is performed in layers. If the dead space is significant or the skin cannot be closed without tension, a plastic surgery consultation for local rotational flaps or free tissue transfer is indicated.
Postoperative Protocols and Rehabilitation
Immediate Postoperative Care
- Wound Management: The surgical site is monitored closely for signs of necrosis or dehiscence, particularly in patients who received neoadjuvant radiation. Drains are maintained until output is less than 30 cc over a 24-hour period.
- Deep Vein Thrombosis (DVT) Prophylaxis: Due to the high risk of venous thromboembolism in orthopedic oncology patients, chemical prophylaxis (e.g., Low Molecular Weight Heparin) is initiated postoperatively and continued for 2 to 4 weeks.
Rehabilitation
- Early mobilization is encouraged to prevent joint contractures.
- Weight-bearing status depends on the extent of muscle resection and whether any osseous structures were compromised.
- Physical therapy focuses on restoring range of motion and strengthening compensatory muscle groups.
Adjuvant Therapies and Surveillance
- If final pathology reveals positive microscopic margins (R1 resection), re-excision is the preferred treatment. If re-excision is anatomically impossible without amputation, postoperative radiation (if not given preoperatively) or brachytherapy is administered.
- The role of adjuvant chemotherapy remains controversial in adult soft tissue sarcomas but is often considered for high-grade, deep tumors larger than 5 cm, particularly in specific histologies like synovial sarcoma or in pediatric populations.
- Surveillance: Patients undergo rigorous follow-up, including clinical examinations and local MRI every 3-4 months for the first 2 years, every 6 months up to year 5, and annually thereafter. Chest CT is performed concurrently to monitor for pulmonary metastasis.
Synthesis of the Literature: Evidence-Based Practice
The surgical management of soft tissue sarcomas is heavily guided by decades of robust clinical research. A review of the foundational literature highlights several critical tenets:
The Importance of Surgical Margins
The status of the surgical margin is the single most important predictor of local recurrence. Bell et al. (J Bone Joint Surg, 1989) and Gronchi et al. (J Clin Oncol, 2005) have extensively documented that positive surgical margins exponentially increase the risk of local failure. The modern consensus dictates that a planned wide resection, achieving a continuous envelope of normal tissue, is mandatory. Unplanned excisions (often termed "whoops" surgeries performed without prior imaging) require aggressive re-excision to clear residual microscopic disease, as noted by Davis et al. (J Surg Oncol, 1997).
Efficacy of Neoadjuvant Therapies
The shift toward limb-sparing surgery was largely facilitated by the integration of neoadjuvant therapies. Eilber et al. (Cancer, 1984; J Clin Oncol, 2001) demonstrated that treatment-induced pathologic necrosis following neoadjuvant therapy is a strong predictor of both local control and overall survival. Furthermore, Choong et al. (Clin Orthop Relat Res, 2001) highlighted the importance of radiotherapy even in selected low-grade sarcomas to prevent local recurrence when wide margins are anatomically constrained.
Histology-Specific Considerations
While the mechanical principles of resection are universal, specific histologies dictate nuanced approaches:
* Extraskeletal Myxoid Chondrosarcoma: As demonstrated in the clinical case above, these tumors often present as large, lobulated masses. They exhibit a prolonged clinical course but have a high propensity for late local recurrence and metastasis, necessitating long-term surveillance (Kawaguchi et al., Cancer, 2003).
* Dermatofibrosarcoma Protuberans (DFSP): Known for extensive microscopic tentacular spread, DFSP requires exceptionally wide margins (often 2-3 cm) or Mohs micrographic surgery to prevent the historically high recurrence rates (Dubay et al., Cancer, 2004).
* Desmoid Tumors (Aggressive Fibromatosis): While histologically benign, desmoids are locally aggressive. Modern management has shifted from radical surgery to a more conservative, multidisciplinary approach involving observation, anti-estrogen therapy (tamoxifen), or targeted agents like Imatinib, reserving surgery for symptomatic or rapidly progressive lesions (Heinrich et al., J Clin Oncol, 2006).
* Synovial Sarcoma: Frequently occurring near joints in young adults, these tumors have a higher rate of lymph node metastasis compared to other sarcomas, necessitating careful regional nodal evaluation (Buck et al., Clin Orthop Relat Res, 1981).
Conclusion
The operative management of extremity soft tissue sarcomas represents one of the most complex challenges in orthopedic surgery. Success relies not merely on technical surgical prowess, but on a profound understanding of tumor biology, meticulous preoperative planning, and seamless collaboration within a multidisciplinary oncology team. By adhering to the principles of wide en bloc resection and appropriate utilization of neoadjuvant therapies, surgeons can achieve the dual goals of oncologic cure and functional limb preservation.
📚 Medical References
- soft tissue sarcomas, Clin Orthop Relat Res 256:22, 1990.
- Lange RH: Limb reconstruction versus amputation decision making in massive lower extremity trauma, Clin Orthop Relat Res 243:92, 1989.
- Lange RH, Bach AW, Hansen ST, et al: Open tibial fractures with associated vascular injuries: prognosis for limb salvage, J Trauma 25:203, 1985.
- Lantsberg L, Goldman M: Laser Doppler fl owmetry, transcutaneous oxygen tension measurements and Doppler pressure compared in patients undergoing amputation, Eur J Vasc Surg 5:195, 1991.
- Latimer HA, Dahners LE, Bynum DK: Lengthening of belowthe-knee amputation stumps using the Ilizarov technique, J Orthop Trauma 4:411, 1990.
- Leow M, Pho R, Pereira B: Esthetic prostheses in minor and major upper limb amputations, Hand Clin 17:489, 2001.
- Levy SW: Sling problems of the amputee. In Bowker JH, Michael JW, eds: Atlas of limb prosthetics: surgical, prosthetic, and rehabilitation principles, 2nd ed, St Louis, 1992, Mosby. Lind J, Kramhoft M, Bodtker S: The infl uence of smoking on complications after primary amputations of the lower extremity, Clin Orthop Relat Res 267:211, 1991.
- Livingston DH, Keenan D, Kim D, et al: Extent of disability following traumatic extremity amputation, J Trauma 37:495, 1994.
- MacKenzie EJ, Bosse MJ, Castillo RC, et al: Functional outcomes following trauma-related lower-extremity amputation, J Bone Joint Surg 86A:1636, 2004.
- Malawer MM, Buch R, Khurana JS, et al: Postoperative infusional continuous regional analgesia, Clin Orthop Relat Res 266:227, 1991.
- Malawer MM, Buch RG, Thompson WE, et al: Major amputations done with palliative intent in the treatment of local bony complications associated with advanced cancer, J Surg Oncol 47:121, 1991.
- Marquardt E, Correll J: Amputations and prostheses for the lower limb, Int Orthop 8:139, 1984.
- Mars M, McKune A, Robbs JV: A comparison of laser Doppler fl uxmetry and transcutaneous oxygen pressure measurement in the dysvascular patient requiring amputation, Eur J Endovasc Surg 16:53, 1998.
- Martini A, Fromm B: A new operation for the prevention and treatment of amputation neuromas, J Bone Joint Surg 71B:379, 1989.
- Matsen S, Malchow D, Matsen F: Correlations with patients’ perspectives of the result of lower-extremity amputation, J Bone Joint Surg 82A:1089, 2000.
- McClure SK, Shaughnessy WJ: Farm-related limb amputations in children, J Pediatr Orthop 25:133, 2005.
- McCollum PT, Walker MA: The choice between limb salvage and amputation: major limb amputation for end-stage peripheral vascular disease: level selection and alternative options. In Bowker JH, Michael JW, eds: Atlas of limb prosthetics: surgical, prosthetic, and rehabilitation principles , 2nd ed, St Louis, 1992, Mosby. Mnaymneh W: The choice between limb salvage and amputation: tumor. In Bowker JH, Michael JW, eds: Atlas of limb prosthetics: surgical, prosthetic, and rehabilitation principles, 2nd ed, St Louis, 1992, Mosby. Mohler DG, Kessler JI, Earp BE: Augmented amputations of the lower extremity, Clin Orthop Relat Res 371:183, 2000.
- Mooney V, Wagner W, Waddell J, et al: The below-knee amputation for vascular disease, J Bone Joint Surg 58A:365, 1976.
- Moore TJ: Planning for optimal function in amputation surgery. In Bowker JH, Michael JW, eds: Atlas of limb prosthetics: surgical, prosthetic, and rehabilitation principles, 2nd ed, St Louis, 1992, Mosby. Morey T, Giannoni J, Duncan E, et al: Nerve sheath catheter analgesia after amputation, Clin Orthop Relat Res 397:281, 2002.
- Moss ALH, Waterhouse N, Townsend PLG, et al: Lengthening of a short traumatic femoral stump, Injury 16:350, 1985.
- Nikolajsen L, Ilkjaer S, Christensen JH, et al: Randomized trial of epidural bupivacaine and morphine in prevention of stump and phantom pain in lower-limb amputation, Lancet 350:1353, 1997.
- Omer GE: Nerve, neuroma, and pain problems related to upper limb amputations, Orthop Clin North Am 12:751, 1981.
- O’Neal ML, Bahner R, Ganey TM, et al: Osseous overgrowth after amputation in adolescents and children, J Pediatr Orthop 16:78, 1996.
- Otis JC, Lane JM, Kroll MA: Energy cost during gait in osteosarcoma patients after resection and knee replacement and after above-the-knee amputation, J Bone Joint Surg 67A:606, 1985.
- Pandian G, Kowalske K: Daily functioning of patients with an amputated lower extremity, Clin Orthop Relat Res 361:91, 1999.
- Pant R, Younge D: Turn-up bone fl ap for lengthening the below-knee amputation stump, J Bone Joint Surg 85B:171, 2003.
- Patterson BM, Smith AA, Holdren AM, et al: Case reports: osteocutaneous pedicle fl ap of the foot for salvage of belowknee amputation level after lower extremity injury, J Trauma 48:767, 2000.
- Pederson NW, Pederson D: Nutrition as a prognostic indicator in amputations, Acta Orthop Scand 63:675, 1992.
- Pedowitz WJ: Soft tissue disorders of the foot. In Coughlin MJ, Mann RA, eds: Surgery of the foot and ankle, 7th ed, vol 1, St Louis, 1999, Mosby. Pellegrini VD, Reid S, Evarts CM: Complications. In Rockwood CA, Green DP, Bucholz RW, et al, eds: Rockwood and Green’s fractures in adults, 4th ed, Philadelphia, 1996, Lippincott-Raven. Persson BM, Broome A: Lengthening a short femoral amputation stump: a case of tissue expander and endoprosthesis, Acta Orthop Scand 65:99, 1994.
- Pinzur MS: Amputations and prosthetics. In Beaty JH, ed: Orthopaedic knowledge update 6, Rosemont, Ill, 1999, American Academy of Orthopaedic Surgeons. Pinzur MS, Angelats J, Bittar T: Salvage of failed amputation about the hip in peripheral vascular disease by open wound care and nutritional support, Am J Orthop 27:561, 1998.
- Pinzur MS, Bowker JH:
You Might Also Like