Proximal Humerus Fracture: Your Essential Management Guide
Key Takeaway
Looking for accurate information on Proximal Humerus Fracture: Your Essential Management Guide? A proximal humerus fracture is a break in the upper part of the arm bone near the shoulder joint, comprising 4-5% of all fractures. It commonly results from falls in older individuals, often linked to osteoporosis. The humeral head receives its major blood supply from the anterior and posterior humeral circumflex arteries. Fracture displacement can be influenced by deforming muscular forces.
Management of Proximal Humerus Fracture
Questions
1. What is the injury shown in Figure 12.9?
2. What factors affect the prognosis of these fractures?
- What is the blood supply of the humeral head?
- How would you manage this patient with a varus displaced, surgical neck of humerus fracture? Discuss the pros and cons of different treatment options.
Varus Proximal Humerus Fracture


This is an AP radiograph of the right shoulder demonstrating a two-part, varus displaced, surgical neck of humerus fracture.
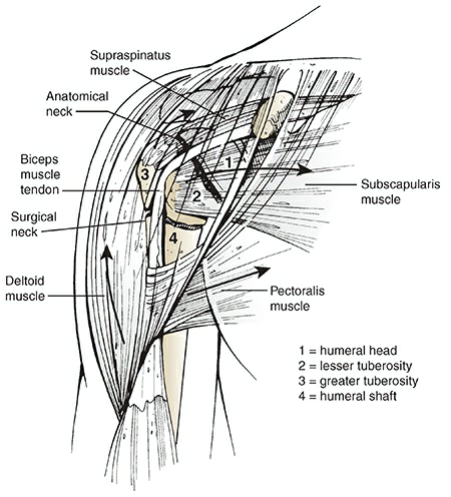
## Proximal Humerus Fractures ## EPIDEMIOLOGY | | | | | | :---------------- | :---------------------------------------------------------------------------------- | :------------------------------------------------------------------------------------------ | :-------------------------------------- | | Constitutes | 4% to 5% of all fractures | Incidence is 300,000 per year (more common than hip fracture) | Most (85%) are nondisplaced | | Older individuals | Higher incidence secondary to osteoporosis | A proximal humerus fracture in an older individual after a simple fall is considered a fragility fracture | The 2:1 female-to-male ratio is also related to osteoporosis | ## ANATOMY - The shoulder has the greatest range of motion of any joint in the body, secondary to the shallow glenoid fossa that is only 25% the size of the humeral head. The major contributor to stability is not bone but the soft tissue envelope composed of muscle, capsule, and ligaments. - The proximal humerus is retroverted 35 to 40 degrees relative to the epicondylar axis. - The shoulder has four osseous segments (Neer): humeral head, lesser tuberosity, greater tuberosity, and humeral shaft. * **Deforming muscular forces on the proximal humerus:** - The supraspinatus and external rotators, which displace the greater tuberosity superior and posterior - The subscapularis, which displaces the lesser tuberosity medially - The pectoralis major, which displaces the humeral shaft medially - The deltoid, which abducts the proximal fragment  Displacement of the fracture fragments depends on the pull of the muscles of the rotator cuff and the pectoralis major. * **Neurovascular supply** - The major blood supply is from the anterior and posterior humeral circumflex arteries. - The axillary nerve courses just anteroinferior to the glenohumeral joint, traversing the quadrangular space. It is at particular risk for traction injury owing to its relative rigid fixation at the posterior cord and deltoid as well as its proximity to the inferior capsule where it is susceptible to injury during anterior dislocation and anterior fracture-dislocation. ## MECHANISM OF INJURY The most common mechanism is a fall onto an outstretched upper extremity from a standing height, typically in an older woman (**fragility fracture**). Younger patients typically sustain a proximal humeral fracture following high-energy trauma, such as a motor vehicle accident. These usually represent more severe fractures and dislocations, with significant associated soft tissue disruption and multiple injuries. Less common mechanisms include excessive shoulder abduction in an individual with osteoporosis, in which the greater tuberosity prevents further rotation; direct trauma, usually associated with greater tuberosity fractures; electrical shock or seizure (associated with dislocation); and pathologic processes, such as malignant or benign processes in the proximal humerus. ## CLINICAL EVALUATION - Patients typically present with the arm held closely to the chest by the contralateral hand, with shoulder pain, swelling, tenderness, painful range of motion, and variable crepitus. - A careful neurovascular examination is essential, with particular attention to axillary nerve function. ## RADIOGRAPHIC EVALUATION A shoulder series, consisting of an anteroposterior and lateral (“Y”) views in the scapular plane as well as an axillary, is standard. Computed tomography is helpful in evaluating articular involvement, degree of fracture displacement, impression fractures, and glenoid rim fractures. Magnetic resonance imaging is generally not indicated for fracture management, but it may be used to assess rotator cuff integrity. ## CLASSIFICATION * **Neer** Defines four parts: These are the greater and lesser tuberosities, humeral shaft, and humeral head. A part is defined as displaced if >1 cm of fracture displacement or >45 degrees of angulation. Fracture types: | Fracture Type | Description | | :--------------- | :--------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- | | One-part fractures | No displaced fragments regardless of number of fracture lines | | Two-part fractures | - Anatomic neck - Surgical neck - Greater tuberosity - Lesser tuberosity | | Three-part fractures | - Surgical neck with greater tuberosity - Surgical neck with lesser tuberosity | | Four-part fractures | - Fracture-dislocation - Articular surface fracture |  The Neer classification of proximal humerus fractures. GT, greater tuberosity; LT, lesser tuberosity; SN, surgical neck. * **Orthopaedic Trauma Association** See Fracture and Dislocation Compendium at:
## Proximal Humerus Fractures ## SUMMARY Proximal humerus fractures are common fractures often seen in older patients with osteoporotic bone following a ground-level fall on an outstretched arm. Diagnosis is made with orthogonal radiographs of the shoulder. Treatment with sling immobilization is indicated for minimally displaced fractures with surgical fixation versus arthroplasty indicated in more complex and displaced fractures. ## EPIDEMIOLOGY - **Incidence:** common; 4-6% of all fractures - **Demographics:** - 2:1 female to male ratio - Increasing age associated with more complex fracture types - **Anatomic location:** may occur at the surgical neck, anatomic neck, greater tuberosity, and lesser tuberosity; two-part surgical neck fractures are most common - **Risk factors:** - Osteoporosis - Diabetes - Epilepsy - Female gender ## ANATOMY * **Osteology** - Anatomic neck represents the old epiphyseal plate; surgical neck represents the weakened area below head; more often involved in fractures than anatomic neck; average neck-shaft angle is 135 degrees * **Muscles** - Pectoralis major displaces shaft anteriorly and medially - Supraspinatus, infraspinatus, and teres minor externally rotate greater tuberosity - Subscapularis internally rotates articular segment or lesser tuberosity * **Ligaments** - Coracohumeral ligament attaches to coracoid and greater tuberosity and strengthens the rotator interval - SGHL restraint to inferior translation at 0° degrees of abduction (neutral rotation) - MGHL resists AP translation in the midrange (~45°) of abduction - IGHL restraint to AP translation at 90° degrees of abduction * **Blood Supply** - Anterior humeral circumflex artery with large number of anastomosis with other vessels in the proximal humerus - Branches: - Anterolateral ascending branch; arcuate artery is the terminal branch and main supply to greater tuberosity - Posterior humeral circumflex artery; recent studies suggest it is the main blood supply to humeral head ## CLASSIFICATION * **AO/OTA** Organizes fractures into 3 main groups and additional subgroups based on fracture location, status of the surgical neck, and presence/absence of dislocation. * **Neer classification** Based on anatomic relationship of 4 segments: greater tuberosity, lesser tuberosity, articular surface, and shaft. Considered a separate part if displacement of > 1 cm or 45° angulation. Minimally displaced, two-part, three-part, four-part, anatomical neck, surgical neck, greater tuberosity, lesser tuberosity, fracture-dislocation, and head split. ## PRESENTATION * **Symptoms** - Pain and swelling - Decreased motion * **Physical exam** - Inspection: extensive ecchymosis of chest, arm, and forearm - Neurovascular exam: axillary nerve injury most common; determine function of deltoid muscle and lateral shoulder sensation; arterial injury may be masked by extensive collateral circulation preserving distal pulses - Examine for concomitant chest wall injuries ## IMAGING * **Radiographs** Recommended views: complete trauma series, true AP (Grashey), scapular Y, and axillary. Additional views include apical oblique, Velpeau, and West Point axillary. Findings may include combined cortical thickness (medial + lateral thickness >4 mm) and pseudosubluxation (inferior humeral head subluxation caused by blood in the capsule and muscular atony). * **CT scan** - Indications: preoperative planning; humeral head or greater tuberosity position uncertain; intra-articular comminution; concern for head-split fracture * **MRI** - Indications: rarely indicated; useful to identify associated rotator cuff injury ## TREATMENT * **Nonoperative** Sling immobilization followed by progressive rehabilitation. - Indications: most proximal humerus fractures can be treated nonoperatively, including minimally displaced surgical and anatomic neck fractures and greater tuberosity fracture displaced < 5mm; fractures in patients who are not surgical candidates; additional variables to consider include age, fracture type, fracture displacement, bone quality, dominance, general medical condition, and concurrent injuries - Outcomes: immediate physical therapy results in faster recovery * **Operative** - CRPP (closed reduction percutaneous pinning) - Indications: two-part surgical neck fractures; 3-part and valgus
