Orthopedic Board Review MCQs (2026 Edition) - Part 3
30 مارس 2026 95 min read 45 Views
Score:
0
%
Orthopedic Board Review MCQs (2026 Edition) - Part 3
QUESTION 1
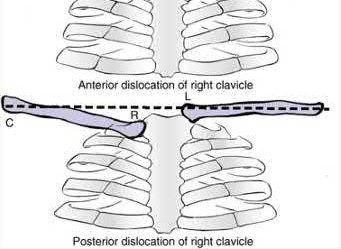
What structure is considered the single most important soft-tissue restraint to anterior-posterior stability of the sternoclavicular joint?
1
Posterior capsular ligament
2
Anterior capsular ligament
3
Interclavicular ligament
4
Intra-articular disk
5
Subclavius tendon
In a cadaver ligament sectioning study, the posterior capsular ligament was considered the most important structure for anterior-posterior stability of the sternoclavicular joint. The anterior capsular ligament also helps prevent anterior displacement but not to the same degree as the posterior ligament. The interclavicular ligament provides little support for anteroposterior translation.
REFERENCES: Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Rockwood CA Jr, Matsen FA III, Jobe CM: Gross Anatomy of the Shoulder. Philadelphia, PA, WB Saunders, 1998.
QUESTION 2
Conservative management of recurrent unidirectional posterior shoulder
2. instability emphasizes strengthening of the
3. 1- deltoid.
4. 2- trapezius.
5. 3- infraspinatus.
6. 4- pectoralis major.
7. 5- latissimus dorsi.
1
instability emphasizes strengthening of the
2
1- deltoid.
3
2- trapezius.
4
3- infraspinatus.
5
4- pectoralis major.
1.
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Fronek J, Warren RF, Bowen M: Posterior subluxation of the glenohumeral joint. J Bone Joint Surg 1989;71A:205-216.
#
QUESTION 3
Slide 1
A 42-year-old man with diabetes presents for treatment of a swollen foot (Slide). He does not recall the onset of swelling, and he states that his foot is not painful. On examination, the foot is hot to touch and swollen. Upon radiographic examination, no deformities are evident. Which of the following treatment options should be used next:
1
Short leg cast
2
Magnetic resonance image scan
3
Biopsy of the midfoot
4
Technetium and indium scan
5
Initiation of organism-specific intravenous antibiotic therapy
This patient presents with an acute neuroarthropathy. The acute painless swelling, associated with warmth and absence of radiographic findings, is typical of the acute phase of a C harcot process. A short leg cast or a boot to immobilize the foot is ideal, and no weight bearing should be permitted until the acute phase of this neuroarthropathy has subsided.
QUESTION 4
of 100
What is the most serious outcome associated with this injury?
1
Osteonecrosis
2
Subtalar arthritis
3
Wound necrosis
4
Complex regional pain syndrome
- Subtalar arthritis_
QUESTION 5
of 100
!img
A
!img
B
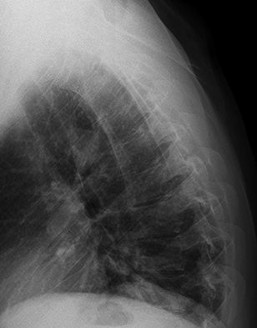
Figures 52a and 52b are the radiographs of a patient who was involved in a motor vehicle collision. He was wearing his seat belt and is now complaining of midthoracic back pain. Radiographs in the emergency department do not reveal a fracture. What is the most appropriate next step?
1
Nonsteroidal medication and follow up as needed
2
Repeat radiographs in 1 week
3
MR imaging of the thoracic spine
4
Flexion-extension radiographs
Ankylosing spinal disorders, including ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis, are conditions that make the spine rigid and at risk for 3-column unstable fractures. Spinal fractures in these patients pose high risk for complications and death and patients should be counseled and observed closely. Mortality strongly correlates with older age and increased number of comorbidities.
These spine fractures often are not seen at the time of initial evaluation, and a delay in diagnosis can occur in up to 19% of cases. This is particularly common in the setting of non- or minimally displaced fractures following minor injuries. A delayed diagnosis can lead to displacement of a previously nondisplaced fracture that can incur a high neurologic injury risk. Advanced imaging with a CT scan or MRI should be obtained for patients with ankylosing spinal disorders even when minor injuries occur. Although bracing and observation can be used, posterior multilevel spinal instrumentation is typically required to obtain adequate spinal stabilization.
The radiographs show an osteopenic ankylosed thoracic spine; the anteroposterior radiograph clearly shows fusion of the sacroiliac joints. Recognition of these radiographic findings is important when evaluating patients after an injury.
# RECOMMENDED READINGS
[Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010 May 15;35(11):E458-64. doi: 10.1097/BRS.0b013e3181cc764f. PubMed PMID: 20421858. ](http://www.ncbi.nlm.nih.gov/pubmed/20421858)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20421858)
[Hendrix RW, Melany M, Miller F, Rogers LF. Fracture of the spine in patients with ankylosis due to diffuse skeletal hyperostosis: clinical and imaging findings. AJR Am J Roentgenol. 1994 Apr;162(4):899-904. PubMed PMID: 8141015. ](http://www.ncbi.nlm.nih.gov/pubmed/8141015)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8141015)
QUESTION 6
Arthroscopic resection/debridement posterior to the midline of the radio-capitellar joint can result in damage to ligament, resulting in instability.
1
Lateral collateral; valgus
2
Ulnar collateral; valgus
3
Ulnar collateral; posterolateral rotatory
4
Annular; posterolateral rotatory
5
Lateral collateral; posterolateral rotatory
Resection posterior to the midpoint of the radiocapitellar joint can result in damage to the lateral collateral ligament and subsequent development of posterolateral rotator instability.
QUESTION 7
Which clinical or radiographic finding is not commonly associated with moderate or severe hallux valgus deformity in adults:
1
Positive family history
2
Presence of bilateral bunion deformity
3
Oval or curved metatarsophalangeal joint on radiographs
4
Longer 1st metatarsal than 2nd metatarsal
5
Achilles tendon contracture
A clinical series of 122 bunions was evaluated for demographic, etiologic, and radiographic findings associated with moderate to severe hallux valgus deformity. The following findings were reported:
83% of patients had a positive family history of bunions
84% of patients had bilateral bunion deformities
71% of patients had curved or oval-shaped metatarsophalangeal joints
71% of patients had a longer 1st metatarsal compared to the 2nd metatarsal by an average of 2.4 mm
11% of bunions were associated with an Achilles tendon contracture
QUESTION 8
of 100
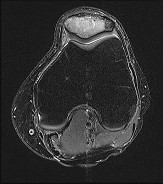
Figures 96a and 96b are the MRI sections of the symptomatic left knee of a 28-year-old man with left anterior knee pain 18 months after undergoing an allogenic bone marrow transplant for acute myelogenous leukemia. His intraoperative fluoroscopy images are shown in Figures 96c and 96d. What is most critical when obtaining a diagnosis for this patient?
!img
!img
!img
!img
1
Sampling from the periphery of the lesion
2
Immediate formalin fixation
3
Sending unfixed fresh tissue
4
Fixation with ribonucleic acid (RNA) stabilization solution
Flow cytometry and cytogenetic analysis are frequently crucial to make an accurate diagnosis of leukemia and lymphoma. These techniques are best performed on fresh, unfixed tissue. Optimal technique includes moistening the tissue to prevent desiccation and immediately sending the specimen for pathologic analysis. Communication with the pathologist regarding the possibility of
a leukemia or lymphoma is prudent to facilitate prompt processing. It is advisable to have a hematology technician in the operating room to handle tissue. Sampling the periphery of tumors with cystic components is often necessary to obtain cellular tissue, but this necessity is not specific to leukemia and lymphoma cases. Formalin is the standard tissue preservation solution for most biopsies. RNA stabilization solution is usually used for research rather than clinical purposes.
RECOMMENDED READINGS
101. [Traina F, Errani C, Toscano A, Pungetti C, Fabbri D, Mazzotti A, Donati D, Faldini C. Current concepts in the biopsy of musculoskeletal tumors: AAOS exhibit selection. J Bone Joint Surg Am. 2015 Jan 21;97(2):e7. doi: 10.2106/JBJS.N.00661. Review. PubMed PMID: 25609446. ](http://www.ncbi.nlm.nih.gov/pubmed/25609446)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/25609446)[ ](http://www.ncbi.nlm.nih.gov/pubmed/25609446)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25609446)
102. Virgo PF, Gibbs GJ. Flow cytometry in clinical pathology. Ann Clin Biochem. 2012 Jan;49(Pt 1):17-
[28/. doi: 10.1258/acb.2011.011128. Epub 2011 Oct 25. Review. PubMed PMID: 22028426. ](http://www.ncbi.nlm.nih.gov/pubmed/22028426)[View](http://www.ncbi.nlm.nih.gov/pubmed/22028426)[ ](http://www.ncbi.nlm.nih.gov/pubmed/22028426)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22028426)
103. Huang Q, Reddi D, Chu P, Snyder DS, Weisenburger DD. Clinical and pathologic analysis of extramedullary tumors after hematopoietic stem cell transplantation. Hum Pathol. 2014 Dec;45(12):2404-10. doi: 10.1016/j.humpath.2014.07.022. Epub 2014 Aug 23. PubMed PMID:
[25294373/. ](http://www.ncbi.nlm.nih.gov/pubmed/25294373)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25294373)
QUESTION 9
of 100
A 70-year-old man has a 1-year history of progressive right shoulder pain, motion loss, and weakness associated with rotator cuff arthropathy. He has failed nonsurgical treatment. During the informed consent process, the patient is counseled regarding his treatment options, and the surgeon recommends that he undergo a right reverse total shoulder arthroplasty (rTSA). The patient must be informed about the complications associated with this type of procedure, the most common of which is
1
infection.
2
prosthetic joint instability.
3
neurologic injury.
4
scapular notching.
rTSA originally was used to address rotator cuff arthropathy. Current indications have expanded to include massive rotator cuff tears without arthritis, failed shoulder arthroplasty, 3- and 4-part proximal humerus fractures, and glenohumeral arthrosis associated with severe/uncorrectable glenoid retroversion. rTSA volume has increased, leading to identification of problems specific to the procedure. Some of the common complications include neurologic injury, periprosthetic fracture, hematoma, infection, scapular notching, prosthetic joint instability, baseplate failure, and acromial fracture. A meta-analysis performed by Bohsali and associates involving rTSA
demonstrated these complications in decreasing order of frequency: scapular notching, hematoma formation, glenoid dissociation such as baseplate failure or aseptic loosening, glenohumeral dislocation, acromial and/or scapular spine fracture, infection, loosening or dissociation of the humeral component, and nerve injury.
RECOMMENDED READINGS
6. [Cheung E, Willis M, Walker M, Clark R, Frankle MA. Complications in reverse total shoulder arthroplasty. J Am Acad Orthop Surg. 2011 Jul;19(7):439-49. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/21724923)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21724923)
7. [Bohsali KI, Wirth MA, Rockwood CA Jr. Complications of total shoulder arthroplasty. J Bone Joint Surg Am. 2006 Oct;88(10):2279-92. Review. PubMed PMID: 17015609. ](http://www.ncbi.nlm.nih.gov/pubmed/17015609)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17015609)
QUESTION 10
A 32-year-old volleyball player has dull posterior shoulder pain. An examination reveals moderate external rotation weakness with his arm at his side but normal strength on supraspinatus isolation. Deltoid and supraspinatus bulk appear normal, although there appears to be mild infraspinatus atrophy. Sensation is normal throughout the shoulder and shoulder girdle. What is the most likely diagnosis?
1
Calcified transverse scapular ligament
2
Parsonage-Turner syndrome
3
Spinoglenoid notch cyst
4
Quadrilateral space syndrome
This clinical scenario describes a patient with an isolated injury affecting the infraspinatus muscle. The anatomic location of such a lesion would be at the spinoglenoid notch, at which the suprascapular nerve may be compressed distal to its innervation of the supraspinatus but proximal to the infraspinatus innervation. A calcified transverse scapular ligament would also affect the suprascapular nerve but is proximal to the innervation of both muscles. Quadrilateral space syndrome would affect innervation of the deltoid (and teres minor). Parsonage-Turner syndrome is a more diffuse, and often severely painful, brachial plexus neuropathy.
QUESTION 11
of 100
What is the most appropriate systemic therapy for this patient in the short term?
1
Bisphosphonate therapy
2
Monoclonal antibody against receptor activator of nuclear factor kappa beta ligand
3
Doxorubicin
4
Dexamethasone
- Dexamethasone
QUESTION 12
of 100
Which treatment of the current fracture will provide the best long-term outcome?
1
Casting it in its current position, which is acceptable alignment
2
Closed reduction and casting
3
Functional brace because this is a stable fracture
4
Open reduction with revision of the current implants
Many patients with mild dominant OI (the most common type) appear “normal,” and a diagnosis cannot be made without a careful personal history, family history, and observance of blue sclera. More than 3 fractures during childhood places someone outside of the mean and should merit further investigation. There is no sign of rickets on this radiograph (physeal widening/cupping). Similarly, the history and examination finding of blue sclera in the patient and his mother should raise concern for OI. Many parents of children with OI have inappropriately been accused of abuse despite obvious examination, radiograph, and family history findings that suggest OI. Low-energy mechanisms that create displaced fractures are a hallmark of OI and do not in isolation raise suspicion for nonaccidental trauma.
Based on the history and examination, mild-form OI caused by a defect in the type I collagen gene is most likely. Defects in type II collagen genes affect articular cartilage and cause epiphyseal dysplasia. Defects in the LEPRE cause severe-form OI involving clinically bowed limbs, marked short stature, and white sclera. There is no sign on radiographs of rickets, so severe vitamin D deficiency is not present. The history, examination, and radiographs all point toward OI/osteoporosis rather than nonaccidental trauma.
Peri-implant fractures occur because of a difference in elasticity between the bone with implants and the bone adjacent to it without implants. This is particularly important in the setting of osteoporotic bone in which the difference in elasticity and rigidity will be much more pronounced than in normal bone. Load-sharing implants are preferred when possible. The original fracture occurred proximal to the current fracture in the middle of the plated bone and looks healed with no sign of infection.
This fracture is in unacceptable alignment with subluxation of the radiocapitellar joint. The plates are bent, so closed reduction will not solve the alignment problem. In early childhood, load-sharing implants (flexible rods or wires) should be used to solve the elasticity mismatch that contributed to the current fracture.
|
|
|
Figure 51a
|
Figure 51b
|
Figure 51c
## CLINICAL SITUATION FOR QUESTIONS 51 THROUGH 54
Figures 51a through 51c are the radiographs of an 8-year-old boy with a shoulder deformity and limited cervical range of motion. He has no significant medical problems and plays baseball, pitching with his right arm. His active shoulder abduction is 180 degrees on the left and 150 degrees on the right.
QUESTION 13
Superficial peroneal nerve injury following ankle fracture:
1
Does not occur with nonoperative treatment
2
C an best be avoided during open reduction internal fixation with a posterolateral approach to the fibula
3
Did not ultimately affect the final AOFAS ankle-hindfoot score
4
Occurs in fewer than 5% of operatively fixed fibula fractures
5
C an best be avoided during open reduction internal fixation with an anterolateral approach to the fibula
One hundred twenty patients with ankle fractures were evaluated. Symptomatic superficial peroneal nerve injury was identified in
21% of patients who underwent open reduction internal fixation and 9% of nonoperatively treated patients. AOFAS scores were decreased in patients with symptomatic superficial peroneal nerve injury. No injuries to the superficial peroneal nerve occurred in patients who underwent surgery involving a posterolateral approach to the fibula.
QUESTION 14
A 30-year-old female involved in a severe motor-vehicle collision that requires prolonged extrication. She arrives at a referral trauma center almost 10 hours after her initial injury. She receives tetanus and intravenous antibiotics upon arrival. The patient has an open tibial fracture with significant periosteal stripping and a closed head injury that requires intracranial pressure monitoring. She is cleared for operative intervention by the neurosurgery and trauma surgery services the following morning. She undergoes a thorough debridement, placement of an antibiotic bead pouch, and external fixator placement approximately 18 hours after her injury. She is definitively treated 4 days after her injury with a repeat debridement, gracilis flap and intramedullary nail. Which of the following factors places the patient at increased risk of infection?
1
Free tissue transfer instead of rotational flap
2
Flap coverage at four days after injury
3
Use of an intramedullary nail instead of minimally invasive plating
4
Delay in administration of IV antibiotics
5
Debridement at 15 hours after injury
Intravenous antibiotics are critical to prevent infection in open fractures. Delay in administration of intravenous antibiotics has been linked with increased risk of infection.
Open tibia fractures are associated with high rates of infection. Historically,
early debridement (within 6-8 hours) and early flap coverage (typically defined as less than 72 hours) were thought to minimize the risk of infection. Recent evidence has challenged these findings, with multiple studies demonstrating no significant link between the timing of debridement and rates of infection.
Multiple studies from the Lower Extremity Assessment Project (LEAP) found no significant difference in infection or complication with flap coverage more than 72 hours after injury.
Bhattacharyya et al retrospectively evaluated patients with type IIIB tibial fractures treated with extended use of negative pressure wound therapy. The authors found increased rates of infection beyond 7 days despite the use of negative pressure wound therapy.
Lack et al evaluated the timing of antibiotic administration on infection rates for type III tibial fractures. The authors found increased rates of infection with administration of antibiotics beyond 66 minutes. The authors discuss the possibility of pre-hospital intervention as many severely injured patients have delayed arrival at treatment centers.
Pollak et al prospectively analyzed rates of complication with flap coverage as part of the LEAP study. The authors found no increase in complications with flap coverage beyond 72 hours. The only significant risk for complication was the use of rotational flaps in comminuted or segmental (AO/OTA type C) tibial fractures.
Incorrect answers:
Answer 1: Lower rates of complication, including infection, were seen with free flaps in AO/OTA type C fractures in the study by Pollak et al.
Answer 2: Timing of flap coverage is controversial. Early studies demonstrated increased infection with delay beyond 72 hours, however recent studies using more rigorous statistical analysis do not support these findings.
Answer 3: No study has demonstrated lower infection rates with the use of plating versus nailing in open tibial fractures.
Answer 5: The timing of debridement with open fractures has been shown not to effect the rate of infection in multiple recent studies.
QUESTION 15
Orthopedic MCQS online Shoulder and Elbow 017
SHOULDER AND ELBOW SELF-
SCORED SELF-ASSESSMENT EXAMINATION
# _AAOS 2017_
!img
!img
!img
!img
!img
!img
!img
### CLINICAL SITUATION FOR QUESTIONS 1 THROUGH 4
A 55-year-old man falls on his outstretched arm and sustains the injury shown in the 3-dimensional CT scans in Figures 1a and 1b.
!img
!img
**Question 1 of 100**
Which ligamentous structure attaches to the fracture fragment?
1
Lateral ulnar collateral ligament
2
Radial collateral ligament
3
Posterior medial collateral ligament (MCL)
4
Anterior MCL
_
Varus posteromedial rotatory instability is a complex injury pattern that starts with varus stress resulting in a fracture of the anteromedial coronoid. The anterior MCL attaches to the sublime tubercle, which is part of the anteromedial coronoid facet. The posterior MCL attaches to the posterior medial aspect of the ulna. The radial collateral and lateral ulnar collateral attach to the ulna at the crista supinatoris. The bony landmark is the sublime tubercle; as noted above, the crista supinatoris is lateral on the ulna. The radial notch is also lateral and is the articulation between the proximal ulna and proximal radius. The anteromedial coronoid facet is part of the coronoid, which extends more lateral and anterior than the anteromedial facet. The anteromedial facet represents the critical weight-bearing portion of the ulnohumeral joint. Damage to this structure causes posteromedial subluxation that often results in severe progressive arthritis. The coronoid is the larger structure of which the anteromedial coronoid facet is a portion. The posteromedial coronoid facet does not appear to be critical in weight bearing. The radial notch is not associated with increased stress with weight bearing. The treatment of displaced fractures of this structure is open reduction and internal fixation utilizing buttress plating. Closed treatment is acceptable only for nondisplaced fractures with appropriate radiographic follow-up. Suture fixation is not advocated because of inadequate strength.
RECOMMENDED READINGS
1. Pollock JW, Brownhill J, Ferreira L, McDonald CP, Johnson J, King G. The effect of anteromedial facet fractures of the coronoid and lateral collateral ligament injury on elbow stability and kinematics. J Bone Joint Surg Am. 2009 Jun;91(6):1448-58. doi: 10.2106/JBJS.H.00222.
2. Sanchez-Sotelo J, O'Driscoll SW, Morrey BF. Anteromedial fracture of the coronoid process of the ulna. J Shoulder Elbow Surg. 2006 Sep-Oct;15(5):e5-8. Epub 2006 Jul 26. Erratum in: J Shoulder Elbow Surg. 2007 Jan-Feb;16(1):127. PubMed PMID: 16979044.
QUESTION 16
!img
#### A 19-year-old linebacker for a
#### collegiate football team
#### has had two episodes of
#### bilateral arm tingling and
#### weakness after tackling; the
#### symptoms resolved after
#### 30 minutes of rest. Three
#### follow-up neurologic
#### examinations have been
#### normal. Cervical spine
#### CT and MRI scans
#### Figure 13a
#### are
#### Figure 13b
#### shown in
#### Figure 13c
#### Figures 13a through
#### 13c. What is the next best step in management?
1
#### The addition of a neck roll to the helmet and continuation of play
2
#### Electrodiagnostic studies
3
#### A series of epidural steroid injections, followed by a return to play
4
#### Methylprednisolone dose pack, followed by a return to play in 1 week
5
#### No further participation in football
####
#### DISCUSSION: Cervical spinal stenosis is a contraindication to participation in collision and contact sports. Previously, the risks of permanent quadriparesis from cervical spinal stenosis were thought to be unclear and athletes with cervical spinal stenosis were often allowed to play contact sports. In 1996, Torg and associates reported that developmental narrowing of the cervical canal in a stable patient does not appear to predispose an individual to permanent catastrophic neurologic injury and therefore should not preclude an athlete from participation in contact sports. However, the current understanding is that the actual risks of permanent neurologic injury from cervical stenosis are significant. The Torg ratio was previously used for diagnosis but is more recently thought to be of low predictive value as reported by Cantu. Current methods for diagnosis of cervical spinal stenosis rely on MRI and CT. Current diagnosis is based on comparisons of measurements with normal values. A cervical canal of less than 13 mm is considered stenotic whereas a diameter of less than 10 mm is considered absolute stenosis as reported by Crowl and Kong. This patient has symptomatic stenosis and should not be cleared for contact sports. A neck roll will not prevent neurologic injury in the presence of cervical spinal stenosis. Electrodiagnostic studies are not likely to add any additional significant findings with central canal stenosis. Cervical traction is not of value in the long-term. Epidural steroid injections or a methylprednisolone dose pack are not of value in this situation.
####
#### REFERENCES: Torg JS, Naranja RJ Jr, Pavlov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
#### Cantu RC: The cervical spinal stenosis controversy. Clin Sports Med 1998;17:121-126. Crowl AC, Kong JF: Cervical Spine, in Johnson DL, Mair SD (eds): Clinical Sports Medicine. Philadelphia, PA, Mosby Elsevier, 2006, pp 143-149.
####
QUESTION 17
During open reduction and internal fixation of a both bone forearm fracture, restoration of the radial bow has been most associated with which of the following?
1
Improvement in wrist extension strength
2
Improvement in wrist flexion strength
3
Restoration of forearm rotation
4
Restoration of elbow range of motion
5
Decreased incidence of synostosis
Restoration of the anatomy of the radial bow directly correlates with the range of motion postoperatively (pronation-supination).
The referenced study by Schemitsch et al found that restoration of the normal radial bow was related to the functional outcome. A good functional result
(more than 80 percent of normal rotation of the forearm) was associated with restoration of the normal amount and location of the radial bow. Similarly, the recovery of grip strength was associated with restoration of the location of the radial bow toward normal.
QUESTION 18
All of the following may be seen with preganglionic lesion EXC EPT:
1
Horner syndrome
2
Hemi-diaphragmatic palsy
3
Positive Histamine test
4
Tinel sign
Tinel sign is seen with postganglionic lesions.
QUESTION 19
Epidural analgesia in the postoperative period after total joint replacement is widely used and is associated with all of the following complications except:
1
Nausea
2
Respiratory depression
3
Peroneal nerve palsy
4
Femoral nerve palsy
5
Hypotension
Nausea, hypotension, respiratory depression, and peroneal nerve palsy are associated with epidural analgesia. Be aware of an epidural bleed secondary to anticoagulation efforts for deep venous thrombosis prophylaxis
QUESTION 20
A 53-year-old man reports acute, severe left shoulder pain after undergoing abdominal surgery 10 days ago. Initial management, consisting of anti-inflammatory drugs, physical therapy, and a subacromial injection of corticosteroid, fails to provide relief. Reexamination of the shoulder 2 months after the onset of symptoms reveals atrophy of the infraspinous and supraspinous fossa and profound weakness of active abduction and external rotation. His neck is supple with a full range of motion. Plain radiographs and an MRI scan of the shoulder are normal. What diagnostic study should be performed next in the evaluation of this patient?**
1
Shoulder arthrography
2
MRI of the cervical spine
3
CT of the head
4
Technetium Tc 99m bone scan
5
Electromyography and nerve conduction velocity studies
Suprascapular nerve palsy is a fairly uncommon yet well-known cause of shoulder pain and weakness. A variety of causes have been described, including compression by a ganglion cyst, an anomalous or thickened superior transverse scapular ligament, a humeral and scapular fracture, and traction or kinking of the nerve in the suprascapular notch.
In this patient, the injury is most likely caused by traction or compression of the nerve in the suprascapular notch as the result of positioning during abdominal surgery; therefore, the studies of choice are electromyography and nerve conduction velocity studies. While MRI of the cervical spine may be of some value in ruling out a radiculopathy, the clinical history does not support such a cause for this condition.
REFERENCES: Rengachary SS, Neff JP, Singer PA, Brackett CE: Suprascapular entrapment neuropathy: A clinical, anatomical, and comparative study. Part 1: Clinical study. Neurosurgery 1979;5:441-446.
Rengachary SS, Burr D, Lucas S, Hassanein KM, Mohn MP, Matzke H: Suprascapular entrapment neuropathy: A clinical, anatomical and comparative study. Part 2: Anatomical study. Neurosurgery 1979;5:447-451.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthoscopy 1990;6:301-305.
QUESTION 21
In the evaluation of somatosensory-evoked potential waveforms for intraoperative neuromonitoring for spinal surgery, the minimum criteria for determining potentially significant changes include
1
# 10% decrease in amplitude, 50% decrease in latency.
2
# 10% decrease in amplitude, 50% increase in latency.
3
# 0% loss of amplitude, transient increase in latency.
4
# 50% decrease in amplitude, 10% increase in latency.
5
# 50% decrease in amplitude, 10% decrease in latency.
The established criteria for interpreting a significant change are 50% decrease in signal amplitude, 10% latency increase, and/or a complete loss of potential. Intraoperative spinal cord monitoring during spinal surgery generally consists of a combination of monitoring modalities.Somatosensory-evoked potentials in combination with intraoperative electromyography can provide adequate coverage of sensory and motor components of spinal cord and nerve root function. Significant changes in evoked potential waveform characteristics can reflect dysfunction of the ascending somatosensory system.
QUESTION 22
Arthrodesis of the ankle in a 34-year-old woman should be performed with the ankle positioned in:
1
10° plantarflexion, neutral rotation
2
10° dorsiflexion, 5° external rotation
3
Neutral dorsiflexion, 5° valgus
4
10° plantarflexion, 15° external rotation
5
10° plantarflexion, 5° internal rotation
Although the woman may wish to wear shoes of varying height, there is sufficient plantarflexion occurring through the transverse tarsal joint to permit the wearing of high-heel shoes. Any plantarflexion of the fusion will cause arthritis of the transverse tarsal joint, particularly the talonavicular joint. Dorsiflexion of an ankle arthrodesis is associated with a calcaneus position and heel pain. The ankle should be fused in a similar position for both male and female patients.
QUESTION 23
The greatest amount of step-off that is well-tolerated in a Bennettâs fracture is:
1
0 mm
2
1 mm to 2 mm
3
2 mm to 3 mm
4
3 mm to 4 mm
5
4 mm to 5 mm
Studies by Livesley, Kjaer-Petersen, and others have shown that patients with fractures with more than a 1-mm step-off after reduction were more likely to develop arthritis at the thumb carpometacarpal joint. Although some studies have not shown functional outcome correlating with the presence of arthritis, Oosterbos and De Boer found that all their patients with fair and poor overall results had nonanatomic reductions. Although a cadaveric study by C ullen has shown that a 2-mm step-off may be acceptable, this contrasts with the clinical evidence currently available.
QUESTION 24
Which of the following areas of the osteoclast is responsible for attachment to the bone surface prior to the bone resorption process:
1
Golgi apparatus
2
Ribosome
3
Clear zone
4
Ruffled border
5
Secretory vesicles
Active osteoclasts resorb the mineral and organiCmatrix of bone and attach to the exposed bone matrix. When osteoclasts are studied with an electron microscope, there are two prominent findings â a ruffled border and a clear zone. In the clear zone, the osteoclast seals off the area of bone to be resorbed by attaching to the bone surface. The osteoclast attaches to the bone surface through a receptor-mediated process with the assistance of proteins called integrins. The ruffled border is an area found in the infoldings of the cell membrane. At the area of the ruffled border, the osteoclasts lower the pH with hydrogen ions through the carboniCanhydrase system. This lowered pH increases the solubility of the apatite crystals and the mineral can be removed. The organiCcomponents of the bone are then hydrolyzed through acidiCproteolytiCdigestion.
QUESTION 25
Severe neurological manifestations have been attributed with accumulation of what metal ion in the brain:
1
Al
2
Co
3
Cr
4
V
5
Ni
Several neurological manifestations have been attributed to Al intoxication in humans, including memory loss, jerking, ataxia, and neurofibrillary degeneration. The development of some neuropathological conditions, including amyotrophiClateral sclerosis, Parkinsonian, dementia, dialysis encephalopathy, and senile plaques of Alzheimerâs disease, may be related to the accumulation of Al in the brain
QUESTION 26
-
Which of the following findings is the most specific for ankylosing spondylitis?
1
Positive HLA-B27 antigen
2
Chest expansion limited to less than 2.5cm
3
Generalized ligamentous laxity
4
Positive rheumatoid factor (greater than 1 to 64)
5
The presence of Achilles tendonitis for more than three months
QUESTION 27
Subchondral drilling for cartilage defects is effective for:
1
Varus alignment
2
Valgus alignment
3
Subchondral sclerosis
4
Fibrocartilage formation
5
Rheumatoid arthritis
Subchondral drilling allows the blood supply to form clot-containing stem cells from which fibrocartilage forms. It is not indicated in patients with systemiCdisease like rheumatoid arthritis. It is ineffective for varus or valgus alignment or subchondral sclerosis
QUESTION 28
An 18-year-old rugby player has had pain in his ring finger after missing a tackle 1 week ago. Examination reveals tenderness in the distal palm, and he is unable to actively flex the distal interphalangeal (DIP) joint. Radiographs are normal. What is the most appropriate management? ](http://www.orthobullets.com/anatomy/12300/2017-moc-hand-89-day-study-plan)
1
Acute tendon repair
2
DIP joint extension splinting for 6 weeks
3
DIP and proximal interphalangeal joint extension splinting for 6 weeks
4
Buddy taping to the middle finger for 2 weeks
5
Early range-of-motion exercises and return to play as pain permits
QUESTION 29
Which of the following is considered a reasonable goal for arthroplasty surgery in rotator cuff arthropathy?
1
Restore normal humeral head glenoid contact location
2
Restore full active overhead motion
3
Restore proper glenoid version with bone preparation and use of a cemented glenoid component
4
Achieve formal decompression and acromioplasty with resection of the coracoacromial ligament and distal clavicle
5
Achieve a secure closure of the subscapularis with an appropriate head size
Absence of the rotator cuff results in superior migration of the humeral head because of unopposed deltoid function. This proximal migration results in eccentric loading of glenoid components with early loosening. Hemiarthroplasty yields good pain relief with limited goals of active elevation of 90 degrees. The coracoacromial arch should be preserved. Achieving satisfactory subscapularis tension is preferred to the use of an oversized humeral component.
REFERENCES: Zeman CA, Arcand MA, Cantrell JS, Skedros JG, Burkhead WZ Jr: The rotator cuff-deficient arthritic shoulder: Diagnosis and surgical management. J Am Acad Orthop Surg 1998;6:337-348.
Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for the treatment of defects in the rotator cuff and the surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491.
Williams GR Jr, Rockwood CA Jr: Hemiarthroplasty in rotator cuff-deficient shoulders. J Shoulder Elbow Surg 1996;5:362-367.
Zuckerman JD, Scott AJ, Gallagher MA: Hemiarthroplasty for cuff tear arthropathy. J Shoulder Elbow Surg 2000;9:169-172.
QUESTION 30
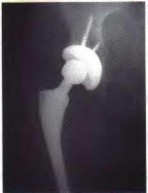
A 42-year-old male sustains a left leg injury as the result of a high-speed motor vehicle collision. Physical exam reveals a grossly deformed left leg with a 1 centimeter open wound over the anterolateral aspect of his tibia; no gross neurovascular deficits are noted. Injury radiographs are shown in Figures A and B. He undergoes immediate tibial nailing with debridement and primary closure of his traumatic wound. Which of the following is the Gustilo-Anderson classification for his fracture?
!img
!img
1
I
2
II
3
IIIA
4
IIIB
5
IIIC
Figures A and B show a significantly comminuted, segmental tibial fracture. In this scenario, the fracture is appropriately classified as a Grade III because there is a highly comminuted, segmental fracture which is always associated with significant periosteal stripping. The patient's leg was able to be closed primarily, which means that it should be classified as a IIIA.
Gustilo et al reviews 18 years of open fracture treatment and outcomes. They reported that débridement and copious irrigation, with primary closure for type I and II fractures and secondary closure for type III fractures resulted in a 5% infection rate (9% for type III fractures). Initial wound cultures were positive in 70.3% despite an infection rate of that patient group of only 2.5%.
Incorrect Answers:
Answer 1: Gustilo Type I wounds have a clean skin lesion that are < 1 cm, and a simple fracture with minimal comminution.
Answer 2: Gustilo Type II wounds have a skin lesion > 1 cm, no extensive soft tissue damage, minimal crushing, and moderate comminution and contamination.
Answer 4: Gustilo Type IIIB are defined as wounds that require a flap for salvage.
Answer 5: Gustilo Type IIIC have an exposed fracture with arterial damage that requires repair.
QUESTION 31
-is the initial lateral radiograph of the foot of a 55-year-old woman who felt a pop in her left foot as she stepped off the curb. She subsequently had severe heel pain and could not bear weight.Examination in the emergency department revealed a bony prominence over the posterior aspect of the heel with blanching of the surrounding skin. What is the most appropriate orthopaedic management?
!img
1
Immediate cast immobilization with maximum plantar flexion
2
Immediate surgical treatment with percutaneous reduction and screw fixation
3
Immediate open reduction and internal fixation via an extensile lateral approach
4
Short leg splint, elevation, and delayed open reduction and internal fixation
5
Short leg splint, elevation, and conversion to cast immobilization when soft-tissue swelling has resolved
QUESTION 32
#### Which of the following can be seen in the heart of a well-conditioned athlete?
1
#### Decreased stroke volume
2
#### Decreased cardiac output
3
#### Decreased resting heart rate
4
#### Decreased ventricular wall thickness
5
#### Decreased vagal tone
#### DISCUSSION: The well-conditioned heart of an athlete leads to increased ventricular wall thickness which in turn increases the amount of blood ejected from the heart per given stroke (stroke volume). The increased parasympathetic (vagal) tone also leads to a lower (decreased) resting heart rate. Cardiac output is equal to stroke volume x heart rate and is increased during exercise in a well-conditioned athlete.
#### REFERENCES: Basilico FC: Cardiovascular disease in athletes. Am J Sports Med 1999;27:108-121. Huston TP, Puffer JC, Rodney WM: The athletic heart syndrome. N Engl J Med 1985;313:24-32.
#### An 18-year-old boxer sustained a blow to his right eye in a boxing match. Examination on the sideline reveals hyphema, reduced visual acuity and color vision, and a visual field cut. What is the next step in management?
1. #### Eye patch and ophthalmology evaluation in 2 days
2. #### Fluorescein eye stain
3. #### Emergent CT
4. #### High-dose systemic steroids
5. #### Observation PREFERRED RESPONSE: 3
#### DISCUSSION: With the examination demonstrating reduced visual acuity and visual field changes,
#### 2010 Sports Medicine Examination Answer Book • 81
####
QUESTION 33
##### A 12-year-old boy is seen 1 week after injuring his knee while playing soccer. He notes pain and swelling. Examination reveals an effusion, laxity with Lachman testing, and he walks with a limp. Radiographs and an MRI scan are shown in Figures 95a through 95d. Treatment should consist of which of the following?
#####
1
##### Physical therapy
2
##### Anterior cruciate ligament reconstruction
3
##### Anterior cruciate ligament reconstruction when the child reaches skeletal maturity
4
##### Anatomic reduction and internal fixation of the fracture fragments
5
##### Casting in extension
##### DISCUSSION: The radiographs and MRI scan show a displaced tibial eminence fracture. Meyer and McKeever classified these injuries, with type 1 being a nondisplaced tibial eminence fracture; type 2 being a displaced tibial eminence fracture with a posterior hinge, and type 3 being a displaced tibial eminence fracture. Tibial eminence fractures in children are equivalent to anterior cruciate ligament tears in adults. Treatment should be anatomic reduction, which often requires an arthroscopic or open procedure, followed by fixation.
##### REFERENCES: Green NE, Swiontkowski MF: Skeletal Trauma in Children, ed 3. Philadelphia, PA, WB Saunders, 2003, pp xvi, 452-455, 638.
##### Zionts LE: Fractures around the knee in children. J Am Acad Orthop Surg 2002;10:345-355.
#####
#####
#####
##### 2010 Pediatric Orthopaedic Examination Answer Book • 79
#####
##### Figure 96
QUESTION 34
Which of the following conditions is not associated with an increased risk of congenital vertical talus?
1
Sacral agenesis
2
C erebral palsy
3
Myelomeningocele
4
ArthrogryposisV
5
Nail patella syndrome
Patients with cerebral palsy do not have an increased risk of congenital vertical talus, but they may develop an acquired neuromuscular vertical talus.
Patients with myelomeningocele have approximately a 5% to 10% risk of vertical talus, far above that of the general population.
Arthrogryposis is associated with an increased risk of vertical talus.
Nail patella syndrome is associated with an increased risk of vertical talus. Sacral agenesis is associated with an increased risk of vertical talus.
QUESTION 35
of 100
A 47-year-old man undergoes a 3-column osteotomy as part of scoliosis surgery. During closure, somatosensory-evoked potentials decrease.
1
Proximal junctional kyphosis (PJK)
2
Adjacent segment degeneration
3
Intraoperative neurological injury
4
Postsurgical wound infection
- Intraoperative neurological injury
QUESTION 36
In treating which of the following elbow fractures is it most important to begin early range of motion:
1
Salter I physeal fracture of distal humerus
2
Intercondylar (T-condylar) fracture of distal humerus
3
Supracondylar fracture of distal humerus
4
Lateral condyle fracture
5
Lateral epicondyle fracture
Intercondylar fractures have a significant risk of loss of motion because of the magnitude of injury, intra-articular extension, and older age of patient.
Salter I physeal fractures typically occur in young children. They usually pose no difficulty with regaining motion after 4 to
6 weeks of immobilization.
Supracondylar fractures usually are followed by regaining motion after healing despite immobilization of up to 6 weeks or more.
Patients with this fracture usually regain their motion after healing. Because this is a nonarticular fracture, loss of motion is not a high risk.
QUESTION 37
A 15-year-old white boy presents to your office with inability to elevate his right shoulder and flex his elbow. He sustained a fall from an all-terrain vehicle 8 weeks ago. He landed on the right shoulder and says his neck was twisted away at the time of fall. He was seen at the local emergency department; skull, chest, cervical and thoracic spine, and shoulder x-rays showed no damage. There was no loss of consciousness and he has no chest pain or breathing difficulties. He was observed in the hospital until stable and was referred to follow up in the hand clinic at 4 weeks and scheduled for an electromyogram.
C linical examination reveals weakness of deltoid, supraspinatus, infraspinatus, teres minor, biceps, brachialis, brachioradialis, and extensor carpi radialis longus. The remainder of his forearm musculature is preserved and he can grasp and release and pinch. Sensations are decreased along the distribution of axillary nerve. There is 3 cm wasting of his arm and 2 cm of his forearm. Tinel sign is positive around the clavicle. Horner signs are absent and his arm lies against the body. The EMG report shows fibrillation potentials in the weak muscles. The parents are concerned and say they have not seen any improvement. The boy reports that he is now able to flex his elbow. When asked to demonstrate you notice that he flexes his wrist and pronates his forearm to âswingâ his elbow into flexion.
What is the least helpful test in further management of this patient:
1
Magnetic resonance imaging
2
C omputer tomography scan of the neck
3
Repeat electromyogram after 4 weeks
4
Somatosensory evoked potential (SSEP)
C omputer tomography scan of the cervical spine will not be of any use as it will neither show the pseudomeningoceles nor provide any information on brachial plexus. C T scan may be needed in case of a suspected neck injury but does not form part of a
brachial plexus work up.
QUESTION 38
### Which of the following surgical maneuvers is most likely to enhance proper patellar tracking during total knee arthroplasty and minimize the need for a lateral retinacular release?
###
1
### Use of a mobile-bearing prosthesis
2
### Anterior placement of the tibial tray
3
### Internal rotation of the femoral component
4
### Internal rotation of the tibial component
5
### External rotation of the tibial component
### DISCUSSION: Slight external rotation of the tibial component medializes the tibial tubercle and helps reduce the tendency for lateral patellar maltracking. Mobile bearings have not been shown to improve patellar tracking.
###
### Internal rotation of the tibial or femoral component will accentuate patellar maltracking. AP positioning of the tibial tray will affect the force across the patella, but it is not likely to affect patellar tracking.
###
### REFERENCES: Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 323-337. Pagnano MW, Trousdale RT, Stuart MJ, et al: Rotating platform knees did not improve patellar tracking: A prospective randomized study of 240 primary total knee arthroplasties. Clin Orthop Relat Res 2004:428:221-227.
###
### Figure 77a Figure 77b
###
QUESTION 39
Which of the following is most important to achieve a good outcome following a Syme amputation?
1
trimming any dog ears
2
a viable and stable heel pad
3
achilles tendon lengthening
4
preserving the malleoli
5
tenodesing the extensor digitorum longus to the tibial shaft
A Syme amputation is effectively a tibiotalar disarticulation, which provides an end-bearing stump that could potentially allow ambulation without a prosthesis over short distances. It works better for tumor and trauma, but the heel pad must be viable. The two most common problems are 1) skin sloughing from compromised vascular supply and 2) migration of the heel pad due to instability. A hypermobile heel pad can cause difficulty with prosthesis wear and damage to the soft tissues which can eventually lead to failure. Both malleoli are usually removed in the procedure, except in children or during the first stage procedure of a diabetic or infection case. The tibialis anterior is usually tenodesed to the anterior heel pad along with the EDL tendon to avoid posterior migration of the heel pad.
QUESTION 40
A 10-year-old patient with Hurler syndrome has undergone a bone marrow transplant and is currently medically stable. He has developed a painful thoracolumbar kyphosis that measures 50° with 25% subluxation T12 on L1. Recommended treatment includes which of the following:
1
Exercise program for the trunk extensor muscles
2
Thoracolumbar orthosis
3
Halo traction followed by orthosis
4
Posterior spinal fusion
5
Anterior and posterior spinal fusion
Anterior and posterior fusion will correct the translation, instability, and ensure a solid fusion.
Exercises will not correct the subluxation, which is the cause of the pain. A thoracolumbar orthosis is not corrective or well tolerated.
There is no need for halo traction.
Posterior fusion alone is not enough to control this focal instability if the patient is well enough to tolerate a more involved procedure.
QUESTION 41
of 100
Which image seen during arthroscopic treatment is most likely associated with this patient’s condition?
A
!img
b !img
c
!img
d !img
1
Figure 10a
2
Figure 10b
3
Figure 10c
4
Figure 10d
This patient’s clinical presentation is consistent with internal impingement accompanied by glenohumeral internal rotation deficit (GIRD). Although throwers may have increased external rotation, their overall arc of motion should be the same as on the nonthrowing side. In comparison, patients with GIRD experience a marked decrease in arc of motion, particularly in internal rotation.
Internal impingement represents a spectrum of findings that can include superior and posterior labral tears, undersurface (articular-sided) tearing of the posterior supraspinatus, posterior glenoid wear, and scar formation of the posterior capsule. Myers and associates demonstrated internal impingement is associated with GIRD, although the latter by itself may be asymptomatic and perhaps a sports-specific adaptation. However, posterior capsular tightness can lead to posterosuperior translation of the humerus during throwing, leading to these injuries. Internal impingement is common among overhead throwing athletes and occurs during the late cocking and early acceleration phases of throwing. Humeral migration during the abducted/externally rotated throwing position results in abutment of the greater tuberosity against the posterosuperior glenoid labrum, which impinges the rotator cuff (Paley and associates).
Pain is often posterior, but symptoms can be vague. Patients may have examination findings consistent with rotator cuff weakness and superior labrum anterior to posterior (SLAP)/biceps involvement. Radiograph findings can be negative, although a Bennett lesion involving hypertrophy and mineralization of the posterior capsular injury may be seen (Wright and Paletta). A CT scan may show glenoid retroversion (Crockett and associates), while MR imaging should be reviewed for a possible partial articular-sided rotator cuff tear, SLAP tear, or increased signal in the posterosuperior labrum or greater tuberosity.
Treatment of this condition should be the focus on therapy, and most cases can be treated nonsurgically. Stretching aimed at the posterior capsule (ie, sleeper stretch) has been reported as effective (Tyler and associates, Litner and associates). Burkhart and associates also demonstrated posterior capsular stretching can help prevent throwing injuries. Because cuff pathology may be present, physical therapy also should include rotator strengthening, scapular stabilization, and addressing of issues related to throwing mechanics (Drakos and associates). Kibler and associates published a comprehensive rehabilitation guideline. Surgical intervention is reserved for those who fail 6 months of nonsurgical treatment and is directed by intra-articular pathology (debridement vs repair of the rotator cuff and labrum) (Braun and associates).
RECOMMENDED READINGS
13. [Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part I: pathoanatomy and biomechanics. Arthroscopy. 2003 Apr;19(4):404-20. Review. PubMed PMID: 12671624. ](http://www.ncbi.nlm.nih.gov/pubmed/12671624)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12671624)
14. [Braun S, Kokmeyer D, Millett PJ. Shoulder injuries in the throwing athlete. J Bone Joint Surg Am. 2009 Apr;91(4):966-78. doi: 10.2106/JBJS.H.01341. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/19339585)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19339585)
15. [Crockett HC, Gross LB, Wilk KE, Schwartz ML, Reed J, O'Mara J, Reilly MT, Dugas JR, Meister K, Lyman S, Andrews JR. Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. Am J Sports Med. 2002 Jan-Feb;30(1):20-6. ](http://www.ncbi.nlm.nih.gov/pubmed/11798991)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11798991)
16. [Drakos MC, Rudzki JR, Allen AA, Potter HG, Altchek DW. Internal impingement of the shoulder in the overhead athlete. J Bone Joint Surg Am. 2009 Nov;91(11):2719-28. doi: 10.2106/JBJS.I.00409. Review. PubMed PMID: 19884449.](http://www.ncbi.nlm.nih.gov/pubmed/19884449)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19884449)
17. [Kibler WB, McMullen J, Uhl T. Shoulder rehabilitation strategies, guidelines, and practice. Orthop Clin North Am. 2001 Jul;32(3):527-38. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/11888148)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11888148)
18. [Lintner D, Mayol M, Uzodinma O, Jones R, Labossiere D. Glenohumeral internal rotation deficits in professional pitchers enrolled in an internal rotation stretching program. Am J Sports Med. 2007 Apr;35(4):617-21. Epub 2007 Feb 9. PubMed PMID: 17293473. ](http://www.ncbi.nlm.nih.gov/pubmed/17293473)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17293473)
19. [Myers JB, Laudner KG, Pasquale MR, Bradley JP, Lephart SM. Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med. 2006 Mar;34(3):385-91. Epub 2005 Nov 22. PubMed PMID: 16303877. ](http://www.ncbi.nlm.nih.gov/pubmed/16303877)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16303877)
20. [Paley KJ, Jobe FW, Pink MM, Kvitne RS, ElAttrache NS. Arthroscopic findings in the overhand throwing athlete: evidence for posterior internal impingement of the rotator cuff. Arthroscopy. 2000 Jan-Feb;16(1):35-40. PubMed PMID: 10627343. ](http://www.ncbi.nlm.nih.gov/pubmed/10627343)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10627343)
21. [Tyler TF, Nicholas SJ, Lee SJ, Mullaney M, McHugh MP. Correction of posterior shoulder tightness is associated with symptom resolution in patients with internal impingement. Am J Sports Med. 2010 Jan;38(1):114-9. doi: 10.1177/0363546509346050. Epub 2009 Dec 4. ](http://www.ncbi.nlm.nih.gov/pubmed/19966099)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19966099)
22. [Wright RW, Paletta GA Jr. Prevalence of the Bennett lesion of the shoulder in major league pitchers. Am J Sports Med. 2004 Jan-Feb;32(1):121-4. PubMed PMID: 14754734. ](http://www.ncbi.nlm.nih.gov/pubmed/14754734)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14754734)
QUESTION 42
of 100
What is the most likely diagnosis?
1
Osteomyelitis
2
Osteoid osteoma
3
Stress fracture
4
Adamantinoma
- Osteoid osteoma_
QUESTION 43
Posttraumatic physeal arrest is most common at which of the following locations?
1
Proximal tibia
2
Proximal humerus
3
Distal radius
4
Distal humerus
5
Distal tibia
Posttraumatic physeal arrest occurs most commonly in the distal medial tibia. Using MRI, Echlund and associates confirmed this finding. Arrest of the distal radius and proximal humerus are rare after trauma. Traumatic injuries of the distal femoral and distal ulnar physis have a high incidence of growth arrest as well.
REFERENCES: Ecklund K, Jaramillo D: Patterns of premature physeal arrest: MR imaging of 111 children. AJR Am J Roentgenol 2002; 178:967-972.
_YAtotoartanadQpyiQter GN: Physeal bridge resection. J Am Acad Orthop Surg 2005; 13:4_
Figure 64a Figure 64b
QUESTION 44
of 100
!img
Figure 54 is the lateral radiograph of a 55-year-old man who is evaluated for a 2-year history of pain and stiffness of his right metatarsophalangeal (MTP) joint. Upon examination he has dorsal bossing, severe crepitation, and pain
with passive range of motion. There is pain with the "grind" test. Dorsiflexion is limited to 0 degrees. No sesamoid tenderness is present. What is the most appropriate surgical treatment?
1
Chevron bunionectomy
2
Cheilectomy and removal of loose body
3
MTP arthrodesis
4
Resection of proximal phalanx
The radiograph reveals end-stage degenerative changes of the first MTP joint with a dorsal loose body. MTP arthritis and decreased joint dorsiflexion is referred to as hallux rigidus. A chevron bunionectomy is used to correct hallux valgus deformity without arthritis. The cheilectomy is used in lesser degrees of joint destruction. Resection of the proximal phalanx results in a floppy toe and is generally not recommended.
# RECOMMENDED READINGS
McNeil DS, Baumhauer JF, Glazebrook MA. Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int. 2013 Jan;34(1):15-32. doi: 10.1177/1071100712460220. Review. PubMed PMID: 23386758.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23386758)
Deland JT, Williams BR. Surgical management of hallux rigidus. J Am Acad Orthop Surg. 2012 Jun;20(6):347-58. doi: 10.5435/JAAOS-20-06-347. Review. PubMed PMID: 22661564.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2022661564)
# CLINICAL SITUATION FOR QUESTIONS 55 THROUGH 58
Figures 55a and 55b are the anteroposterior and lateral radiographs of a 57-year-old man who fell off of a ladder 10 days ago and landed on his left foot. He is now unable to weight bear on the left. He has no history of trauma to this foot, and his medical history is unremarkable. Upon examination his left foot is swollen and tender. Pulses and sensation are intact.
A B
QUESTION 45
How much should training time and intensity be increased per week to avoid bone stress injury:
1
10%
2
20%
3
30%
4
40%
5
50%
Generally, it is best to increase training time and intensity by 150 nm) can stimulate phagocytosis in specialized cells such as macrophages. Once internalized, metal particles can induce cytotoxicity, chromosomal damage, and oxidative stress. The toxicity of particles is modified by passivation and particle size. These factors both influence the dissolution of metal from the surface, which may account for biological activity. Evidence of cell damage, such as irregular cell membranes and enlarged mitochondria, may be induced by the physical properties of the particles
QUESTION 46
Figure 21 shows a coronal T1-weighted MRI scan of the knee. The arrow indicates what anatomic structure? ](http://www.orthobullets.com/anatomy/10120/medbullets-onboarding--draft-html)
!img
1
Posterior cruciate ligament: anterolateral bundle
2
Posterior cruciate ligament: posteromedial bundle
3
Meniscofemoral ligament
4
Popliteus
5
Oblique popliteal ligament
QUESTION 47
of 100
Video 2 shows the squeeze test for a biceps tendon rupture. This test
!img
1
is performed with the elbow in flexion to minimize the function of the brachialis.
2
can help surgeons evaluate the biceps tendon by lengthening the musculotendinous unit.
3
can help surgeons diagnose a partial biceps tear.
4
likely can generate a false-positive result when the lacertus fibrosus is torn.
- is performed with the elbow in flexion to minimize the function of the brachialis._
QUESTION 48
Slide 1 Slide 2 Slide 3
A 44-year-old obese man presents for treatment of acute ankle pain. He does not have a history of trauma or a systemic history of note. His opposite foot has had multiple episodes of acute pain in the past, lasting from 3 to 5 days. On examination, the
ankle is warm, swollen, and exquisitely tender to palpation and any range of motion (Slide1, Slide 2, and Slide 3). C oncerned about the source of pain, you aspirate the joint and send the sample for analysis. You expect to find:
1
Gram-positive cocci
2
Gram-negative rods
3
Normal joint fluid
4
Sodium monourate crystals
5
A high red cell count
This patient most likely has an acute attack of gout. The prior episodes of foot pain and the sudden onset lasting 5 days for each bout is characteristic. The ankle is not a common location for gout (the most frequent site is the hallux metatarsophalangeal joint). The treatment should consist of injection of a corticosteroid into the joint and administration of appropriate oral anti-inflammatory medication.
QUESTION 49
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
1
proximal clavicle and sternocostal margin.
2
proximal humerus.
3
coracoid process.
4
distal clavicle and acromion.
5
anterior scapula.
The patient has a pectoralis major rupture, an injury that occurs most commonly during weight lifting. Grade III injuries represent complete tears of either the musculotendinous junction or an avulsion of the tendon from the humerus, the most common injury site. Examination will most likely reveal ecchymoses and swelling in the proximal arm and axilla, and strength testing will show weakness with internal rotation and in adduction and forward flexion. Axillary webbing, caused by a more defined inferior margin of the anterior deltoid as the result of rupture of the pectoralis, can be seen as the swelling diminishes. Surgical repair is the treatment of choice for complete ruptures. Nonsurgical treatment is associated with significant losses in adduction, flexion, internal rotation, strength, and peak torque. The pectoralis major originates from the proximal clavicle and the border of the sternum, including ribs two through six. The pectoralis major inserts (rather than originates) on the humerus. The coracoid process is the insertion site for the pectoralis minor, as well as the origin for the conjoined tendon. The pectoralis major has no attachment or origin from the scapula. The anterior deltoid originates from the lateral one third of the clavicle and the anterior acromion.
REFERENCES: Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
QUESTION 50
of 100
Figure 1 is the sagittal MR image of a 56-year-old woman who has a 3-year history of severe back pain. Her pain is worse with flexion at the lumbosacral junction and is relieved with extension. She denies any pain in her lower extremities and has no symptoms of neurogenic claudication. Which mediators play roles in the pathogenesis of this condition?
!img
1
Transforming growth factor-beta (TGF-β), bone morphogenetic protein-2 (BMP-2), latent membrane protein 1
2
Tissue inhibitor of matrix metallo-proteinase-1 (MMP-1), growth and development factor5, noggin
■
The patient has degenerative disk disease with diskogenic back pain. Several studies in both humans and animals have implicated TNF-α, IL-1, and MMP in extracellular matrix degeneration and disk degradation. TGF-β, BMP-2, latent membrane protein 1, and growth and development factor-5 are all postulated to play anabolic roles in the intervertebral disk. Biglycan is a small leucine-rich proteoglycan that regulates extracellular matrix assembly within the disk. Noggin and gremlin are biochemical factors not involved in disk degradation.
QUESTION 51
1247) When comparing the fibular plating techniques shown in Figures A and B, the plate position shown in Figure B is associated with which of the following?
!img
!img
1
Increased stiffness
2
Increased strength
3
Decreased rate of hardware prominence
4
Increased risk of intra-articular screw penetration
5
Increased peroneal tendinitis
Lateral plating of the distal fibula has an increased risk of intra-articular screw penetration with the trajectory of the screws distally; bicortical screws will be intra-articular in nature, whereas posterior plating screws will exit anteriorly.
Figure A shows an antiglide (posterior) plating of the distal fibula, while Figure B shows a lateral neutralization plating of the distal fibula. Both methods are acceptable, but posterior antiglide plating is associated with increased construct stiffness and strength, decreased hardware prominence, decreased rates of ankle joint screw penetration, and improved biomechanical findings in osteoporotic bone. However, posterior plating is associated with an increased rate of peroneal tendonitis and irritation. Illustration A shows a lateral radiograph of a posterior fibular plate.
The referenced article by Ostrum et al is a case series of 32 patients who had antiglide plating; he reported a 100% union rate, 95% patient satisfaction rate, and only 4/32 reported peroneal tendinitis, with all resolving by 2
months.
The other referenced article by Schaffer et al reported that the posterolateral antiglide plate demonstrated improved biomechanical stability as compared to the lateral plating, with increased construct stiffness and load to failure.
QUESTION 52
Flexor tendon nutrition is derived from:
1
The vincula
2
The pulleys
3
Synovial diffusion
4
All of the above
5
A and C only
Flexor tendon nutrition in the uninjured state is derived via the vincula, which contain blood vessels for nutrition. Injured tendons obtain nutrition via diffusion of synovial fluid. The pulley system does not contribute to flexor tendon nutrition.
QUESTION 53
A tailorâs bunion is an abnormal prominence of the lateral aspect of the 5th metatarsal head. Similar to hallux valgus deformities, tailorâs bunions can be due to a widened intermetatarsal angle between the 4th and 5th metatarsal shafts. The normal 4-5 intermetatarsal angle is:
1
Less than 8°-9°
2
Less than 12°
3
Less than 15°
4
Less than 20°
5
Less than 25°
4-5 intermetarsal angle in normal feet averages 6.2 degrees. Different authors believe an abnormally wide 4-5 intermetatarsal angle to be anything greater than 8°-9°.
QUESTION 54
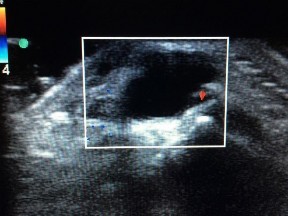
Figure 1 is the ultrasound of a 23-year-old patient who has had a volar radial 1.5-cm tender and painful wrist mass for 6 months. The additional workup prior to surgery should consist of
!img
---
1
serum and urine protein electrophoresis.
2
a chest CT scan.
3
MRI with intravenous contrast.
4
age-appropriate presurgical laboratory studies.
The ultrasound shows a homogeneous anechoic mass consistent with a ganglion cyst. As a benign lesion, no further workup or biopsy is required prior to a marginal surgical excision other than age-appropriate laboratory studies. An MRI study with contrast would provide no diagnostic benefit.
QUESTION 55
**The diagnosis of gout can be made either by the presence of tophaceous deposits in the skin or bursae of the extremities or by the presence of which of the following?**
1
Elevated urine pH
2
Elevated serum uric acid
3
Calcium pyrophosphate crystals in the synovial fluid
4
Monosodium urate crystals in the synovial fluid
5
Elevated serum phosphate
#
**
Gout is an inflammatory arthritis caused by the presence of monosodium urate crystals in the joint. It is characterized acutely by a painful joint that remits after 1 to 2 weeks and recurs periodically. The diagnosis of gout can be made by confirming the presence of monosodium urate crystals in the joint fluid
aspirated from the inflamed joint. Patients with gout may also have tophaceous deposits within the skin or bursae of the extremities. Elevated urine pH, serum uric acid, and serum phosphate can all be associated with numerous conditions and are not specific to gout. Calcium pyrophosphate crystals are associated with chondrocalcinosis (pseudogout).
QUESTION 56
Which of the following methods has the highest sensitivity in detecting skeletal lesions in patients with Langerhans cell histiocytosis:
1
Physical examination
2
Skeletal survey
3
Ultrasound
4
Bone scan
5
Indium labeled white blood cell study
Skeletal survey is the most sensitive means of detecting lesions of eosinophilic granuloma (Langerhans cell histiocytosis). Bone scan detects most, but not all, of the lesions. Some lesions lack enough osteoblastic activity to appear on bone scan. Lesions are not detected on physical exam unless they are large enough to cause pain or tenderness. Indium labeled white cell studies are not used in this condition.
QUESTION 57
A 36-year-old man has a 2-day history of acute lower back pain with severe radicular symptoms in the left lower extremity. The patient has a positive straight leg test at 40 degrees on the left side and mild decreased sensation on the dorsum of the left foot. What is the most appropriate management at this time?
1
# Urgent admission to the hospital for surgical intervention
2
# Immediate MRI of the lumbar spine as an outpatient
3
# Anti-inflammatory medications and activity modification
4
# Caudal epidural steroid injection
5
# Electromyography
In the absence of any severe progressive neurologic deficits or other red flags, the most appropriate management for an acute lumbar disk herniation is nonsurgical care. Conservative treatments such as limited bed rest, anti-inflammatory medications, and judicious use of pain medications are appropriate in this clinical situation. Up to 90% of patients will experience a resolution of symptoms without the need for surgical intervention within a 3-month window. In the acute setting, with no neurologic deficits, immediate MRI of the lumbar spine is neither beneficial nor warranted. Likewise,without signs of an acute deficit, emergent surgical intervention and caudal epidural steroid injections are not needed.
QUESTION 58
Figure 7 shows the radiograph of an otherwise healthy 65-year-old man who injured his right dominant shoulder while skiing 18 months ago. He did not seek treatment at the time of the injury. He now reports intermittent soreness when playing golf but has no other limitations. Examination reveals full range of motion and no tenderness, but he has slight pain with a crossed arm adduction stress test. He is neurologically intact. Initial management should consist of
1
excision of the distal clavicle.
2
open reduction and internal fixation with intramedullary partial threaded pins.
3
open reduction and internal fixation with a reconstruction plate, screws, and bone grafting.
4
bone grafting and use of heavy sutures to secure the clavicle to the coracoid.
5
observation and nonsteroidal anti-inflammatory drugs.
The radiograph shows a displaced type II distal clavicle fracture with nonunion. Because the patient’s symptoms are minimal, the injury can be treated like a grade III acromioclavicular separation. Present management should consist of ice, anti-inflammatory drugs, activity modification, and perhaps physical therapy. If nonsurgical management fails to provide relief, the surgical options are varied with no uniformity in the literature regarding surgical treatment of this injury.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Craig EV: Fractures of the clavicle, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 428-482.
QUESTION 59
of 100
Figure 35 is the radiograph of a 37-year-old woman who began having right forefoot pain about 4 weeks ago after increasing her daily running mileage. She denies any specific injury. Upon examination she has tenderness over the medial forefoot with mild swelling. In addition to her activity level, what is the primary etiology of the radiograph finding?
!img
1
Osteoporosis
2
Hallux valgus deformity
3
Hallux rigidus
4
A relatively long second metatarsal
Stress fractures are the result of physiological bone response to increased stress. Increased stress on bone triggers an increase in remodeling, which begins with resorption of bone at the site of stress. Ongoing stress can overwhelm bone strength, resulting in a fracture. In the foot this most commonly is seen in the second metatarsal at the junction of the middle and distal thirds. Contributing factors to increased loading of the second metatarsal include hallux valgus (decreased hallux loading transfers to the second metatarsal head), hallux rigidus (offloading of the hallux attributable to pain increases second metatarsal loading), and a long second metatarsal (increased duration of contact during push-off in the stance phase).
# RECOMMENDED READINGS
Shindle MK, Endo Y, Warren RF, Lane JM, Helfet DL, Schwartz EN, Ellis SJ.
Stress fractures about the tibia, foot, and ankle. J Am Acad Orthop Surg. 2012 Mar;20(3):167-
[76/. doi: 10.5435/JAAOS-20-03-167. Review. PubMed PMID: 22382289. ](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[ ](http://www.ncbi.nlm.nih.gov/pubmed/22382289)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22382289)
[Donahue SW, Sharkey NA. Strains in the metatarsals during the stance phase of gait: implications for stress fractures. J Bone Joint Surg Am. 1999 Sep;81(9):1236-44. PubMed PMID: 10505520. ](http://www.ncbi.nlm.nih.gov/pubmed/10505520)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10505520)
QUESTION 60
of 100
Compared with iliac crest bone graft, rh2 bone morphogenetic protein (BMP) has a higher rate of
1
reoperation after lumbar fusion.
2
death when used in the anterior cervical spine.
3
cost efficacy when the cost of implants and cost of reoperation are considered.
4
pseudarthrosis in lumbar fusion.
■
BMP is contraindicated for use in the anterior cervical spine. The U.S. Food and Drug Administration produced a warning to not use BMP in anterior cervical surgery due to a higher risk of death (secondary to soft-tissue swelling). When it is used in the lumbar spine, BMP results in lower reoperation rates, higher fusion, and greater cost efficacy when the cost of implants and reoperation are considered.
QUESTION 61
A 16-year-old girl sustained the injury shown in Figure 7a. CT scans are shown in Figures 7b through 7d. The results of treatment of this injury have been shown to most correlate with which of the following factors?
1
Surgical approach
2
Location of the transverse fracture
3
Timing of surgery
4
Accuracy of reduction
5
Use of skeletal traction
The patient has a very low T-type acetabular fracture; however, the head is not congruent under the dome so surgical reduction is necessary. The anterior and posterior columns are displaced and will move independent from each other. The extended iliofemoral is the only approach allowing for visualization and reduction of each column. A combined anterior and posterior approach may also be used. The timing of surgery should be within the first 3 weeks of injury to optimize chances of obtaining an accurate reduction because this is an important factor in determining outcome.
REFERENCES: Letournel E, Judet R (eds): Fractures of the Acetabulum, ed 2.
Berlin, Germany, Springer-Verlag, 1991.
Matta JM: Fractures of the acetabulum: Accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am
1996;78:1632-1645.
QUESTION 62
The net effect of calcitonin on the calcium and phosphorus concentrations in the extracellular fluid and serum is:
1
Increased calcium, increased phosphate
2
Increased calcium, decreased phosphate
3
Decreased calcium
4
Increased calcium, no effect on phosphate
5
Transient decrease in serum calcium
Parathyroid hormone, the active form of vitamin D (1,25 dihydroxyvitamin D), and calcitonin each have a net effect on calcium and phosphorus concentrations in extracellular fluid and serum:
Net Effect
Parathyroid hormone Increased serum calcium
Decreased serum phosphate
Vitamin D3 (1,25 dihydroxyvitamin D) Increased serum calcium
Increased serum phosphate
Calcitonin Decreased serum calcium
(transient)
QUESTION 63
of 100
What is the average time to radiographic union of this fracture?
1
3 weeks
2
4 weeks
3
6 weeks
4
8 weeks
- 6 weeks_
QUESTION 64
-
A 13-year-old quarterback feels a “pop” in his knee while being tackled. Radiographs of the knee and results of a Lachman’s test are normal. Examination reveals tenderness over the distal femoral physis. To help confirm the diagnosis, management should first include
1
an MRI scan
2
arthroscopic examination
3
AP and frog-lateral radiographs of the pelvis and hips
4
varus and valgus stress radiographs of the knee
5
physical examination of the knee under anesthesia
Injuries involving the distal femoral epiphysis cartilage plate are fairly common. Appropriate management should include a complete knee exam with a standard series of X-rays. Of particular importance is to notice any varus or valgus deformity. Stephens et al. (JBJS 1974:56A) measured varus and valgus deformities clinically and roentgenographically. A varus or valgus deformity greater than 3 degrees as compared with the uninjured side was considered clinically significant. Such deformities are highly suggestive of a physeal injury. A MRI may show the injury, but is expensive as is an arthroscopy or examination under anesthesia.
QUESTION 65
Which of the following is true of a knee disarticulation as compared to a transtibial amputation?
1
Faster self-selected walking speeds
2
Improved performance on the Sickness Impact Profile (SIP) questionnaire
3
Physicians were more satisfied with the cosmetic appearance
4
Decreased use of a prosthetic
5
Decreased dependence with patient transfers
Knee disarticulation level is associated with the worst functional result 2 years after injury (compared to transmetatarsal, Symes, AKA, or BKA). The prosthetic use is decreased with a knee disarticulation as compared to a transtibial amputation.
The cohort study by MacKenzie et al prospectively followed 161 patients that were part of the Lower Extremity Assessment Project (LEAP). These patients underwent an above-the-ankle amputation at a trauma center within 3 months following the injury and followed for 2 years. This study revealed that through-the-knee amputations had significantly worse scores for the objective performance measures of self-selected walking speed, independence in transfers, walking, and stair-climbing. Through-the-knee amputees also had worse SIP scores than AKA and BKA patients. Physicians were also less satisfied with both the clinical and the cosmetic recovery of the patients with a through-the-knee amputation. It should be noted that patients with a BKA had a faster walking speed than those with an AKA. Despite the worse SIP scores for through-the-knee amputations, patients actually reported less pain than those with an AKA or BKA, though this wasn't statistically significant.
QUESTION 66
of 100
A right-hand-dominant 45-year-old man sustained an injury to the anterior aspect of his right elbow during sudden elbow flexion while trying to lift a heavy load 3 days ago. He reports the sensation of a sudden, sharp pain at the time of injury, which has since subsided. He has ecchymosis in the anterior and medial elbow regions and has difficulty with resisted forearm supination with the elbow in a flexed position. A diagnosis of an acute distal biceps tendon rupture is made, and, after having a discussion with the patient, surgical treatment is chosen. During surgical reattachment, what is the relationship of the distal biceps tendon within the antecubital fossa to the median nerve and recurrent radial artery before the tendon attaches to the bicipital tuberosity?
1
The tendon travels lateral (radial) to the median nerve and posterior (deep) to the recurrent radial artery
2
The tendon travels lateral (radial) to the median nerve and anterior (superficial) to the recurrent radial artery
3
The tendon travels medial (ulnar) to the median nerve and posterior (deep) to the recurrent radial artery
4
The tendon travels medial (ulnar) to the median nerve and anterior (superficial) to the recurrent radial artery
During surgical repair of a distal biceps tendon rupture, regardless of the surgical approach or technique, an understanding of the regional anatomy is important. The tendon passes distally into the antecubital fossa. The antecubital fossa is defined by the brachioradialis radially and the pronator teres ulnarly. A sheath surrounds the biceps tendon as it passes through the antecubital fossa toward its insertion on the radial tuberosity. The lateral antebrachial cutaneous nerve lies superficially in the subcutaneous tissue of the antecubital fossa. The nerve parallels the brachioradialis. While still superficial, the tendon is contiguous with the lacertus fibrosus that becomes confluent medially with the fascia overlying the flexor-pronator mass. The brachial artery lies just beneath the lacertus fibrosus at the level of the elbow flexion crease. The tendon travels just lateral (radial) to the median nerve within the antecubital fossa and passes posterior (deep) to the recurrent radial artery before it attaches to the radial tuberosity. Full forearm supination allows visualization of the tendinous insertion on the radial tuberosity.
RECOMMENDED READINGS
23. Leslie BM, Ranger H. Biceps tendon and triceps tendon ruptures. In: Baker CL, Plancher KD, eds. _Operative treatment of elbow injuries_. New York: Springer-Verlag; 2002:110-122.
24. [Eames MH, Bain GI, Fogg QA, van Riet RP. Distal biceps tendon anatomy: a cadaveric study. J Bone Joint Surg Am. 2007 May;89(5):1044-9. PubMed PMID: 17473142. ](http://www.ncbi.nlm.nih.gov/pubmed/17473142)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17473142)
QUESTION 67
Figure 1 is the MR image of a high school soccer player who sustained a right knee injury during a game while making a cut toward the ball. He felt a pop and his leg gave way. During physical examination, as the knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a "clunk" within the knee. What is the most likely biomechanical basis for the "clunk"?
!img
!img
!img
!img
1
In extension with internal rotation/valgus force, the medial tibial plateau is subluxated; with flexion, the medial tibial plateau reduces.
2
In extension with internal rotation/valgus force, the medial tibial plateau is reduced; with flexion, the medial tibial plateau subluxates.
3
In extension with internal rotation/valgus force, the lateral tibial plateau is reduced; with flexion, the lateral plateau subluxates.
4
In extension with internal rotation/valgus force, the lateral tibial plateau is subluxated; with flexion, the lateral plateau reduces.
This patient sustained an isolated anterior cruciate ligament (ACL) injury based upon the mechanism described and examination findings. The finding that produces the “clunk” is the pivot-shift maneuver, which is positive in a knee with an incompetent ACL. With an ACL-deficient knee in full extension and internal rotation, the lateral tibial plateau subluxates anteriorly. As the knee is flexed, the lateral tibial plateau slides posteriorly into a reduced position, causing an audible clunk. Response D correctly describes the pathomechanics that result in the audible clunk heard during the pivot-shift maneuver. Responses A and B are incorrect because they describe the medial tibial plateau, which is not part of the pathomechanics of the pivot shift. Response C is incorrect because in extension, the lateral tibial plateau _is subluxated, not reduced._
QUESTION 68
In approaching the lateral lumbar spine through the psoas, the lumbosacral plexus is in danger of being injured. The location of the plexus is best described as which of the following? ](http://www.orthobullets.com/anatomy/10053/psoas)
1
More dorsal in the upper lumbar spine and more ventral in the lower lumbar spine
2
More ventral in the upper lumbar spine and more dorsal in the lower lumbar spine
3
Equally dorsal (junction of anterior two thirds and posterior one third) in the psoas along the lumbar spine
4
Equally ventral (junction of anterior one third and posterior two thirds)in the psoas along the lumbar spine
5
In the midportion of the psoas along the lumbar spine
QUESTION 69
What is the most likely complication following treatment of the humeral shaft fracture shown in Figure 6?
1
Nonunion
2
Shoulder pain
3
Infection
4
Elbow injury
5
Radial nerve injury
The humerus was treated with an intramedullary nail. Findings from two prospective randomized studies of intramedullary nailing or compression plating of acute humeral fractures have shown approximately a 30% incidence of shoulder pain with antegrade humeral nailing. This is the most common complication in both of these series. Nonunions are present in approximately 5% to 10% of humeral fractures treated with an intramedullary nail. Infection has an incidence of approximately 1%. Elbow injury is unlikely unless the nail is excessively long. Rarely, injury to the radial nerve is possible if it is trapped in the intramedullary canal.
REFERENCES: Chapman JR, Henley MB, Agel J, et al: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
McCormack RG, Brien D, Buckley RE, et al: Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail: A prospective, randomised trial. J Bone Joint Surg Br 2000;82:336-339.
QUESTION 70
Figures 1 through 3 are the radiographs of a 55-year-old woman who fell on her outstretched right arm, resulting in acute elbow pain and swelling. On examination, she has lateral elbow bruising and tenderness, with a mechanical block to forearm supination and pronation. She has no medial tenderness. During surgery through a direct lateral approach, the surgeon observes a completely bare lateral epicondyle and surgical repair is performed, resulting in a stable and congruent joint. Initial postoperative rehabilitation should include
1
3 weeks of cast immobilization.
2
elbow extension exercises with the forearm supinated.
3
elbow extension exercises with the forearm pronated.
4
elbow extension exercises with the forearm in neutral rotation.
Radial head fractures are thought to occur as a result of valgus posterolateral rotary load across the elbow, although the mechanism can certainly vary. Minimally or nondisplaced fractures without any clinical instability or block to motion can often be successfully managed non-surgically. Fractures with >2 mm of displacement or fragments that block motion require surgical repair. A critical aspect during surgery is identifying concomitant injury to the lateral collateral ligament complex (LCL). When encountered, the LCL is most often avulsed from its origin at the lateral epicondyle, resulting in a bare area. After the radial head is either repaired or replaced (Figures 4 and 5), the LCL should
16
be repaired back to its anatomic origin. Postoperatively, the surgeon must communicate to the therapist that elbow extension exercises should be performed with the forearm in pronation as a result of the compromised LCL, as this position places the least stress on the ligamentous repair. Elbow extension exercises in supination or neutral are recommended for compromise of the medial collateral ligament, or combined medial and lateral ligament injury, respectively. Without any medial elbow bruising, swelling, or tenderness, it is unlikely that the patient has an injury to the medial collateral ligament.
QUESTION 71
-
An otherwise healthy 65-year-old man has had chronic pain in his prosthetic knee for the past 9 months. Repeated aspirations reveal a coagulase-negative staphylococcus infection. To eradicate the infection while maintaining the best possible joint function, management should consist of
1
Long-term administration of IV and oral antibiotics
2
Open soft-tissue debridement, retention of prosthetic components, and IV antibiotics
3
Immediate exchange arthroplasty with antibiotic-impregnated cement
4
Two-stage surgical prosthetic exchange and IV antibiotics
5
Resection arthroplasty and IV antibiotics
Postoperative wound infections following total joint arthroplasty are generally classified as acute or chronic. The time period is either 2 or 4 weeks from the time of implantation depending on whom you read. This will, generally, determine if you can attempt a one-stage procedure. The other considerations are the bacteria’s resistance to antibiotics and whether or not it produces glycocalyx. If the microorganism elaborates glycocalyx it is highly likely that it will remain after surgical removal of the implants and debridement of the joint.
Present recommendations are to avoid a one-stage reconstruction in a patient in whom a glycocalyx elaborating microorganism has been isolated. In one study 52% of the isolates of S. epidermidis and 28% of the isolates of S. aureus elaborated glycocalyx. The microbiology laboratory can be asked to determine if the microorganisms elaborate glycocalyx. In the present case it should be assumed that the staphylococci elaborate glycocalyx and are resistant to antibiotics. A two-stage procedure is indicated for these reasons alone.
Antibiotic therapy alone has been used for a select group of patients who could not medically tolerate either a one-stage or a two-stage arthroplasty. The patient in this case is listed as otherwise healthy.
The decision to perform a resection arthroplasty as a definitive procedure without reimplantation is based on the bacteria’s resistance to antibiotics, quality of the local soft tissues, the complexity of the reconstruction, the patient’s refusal to have another operation, the patient’s overall health, or a combination of these factors. None of which appear to be present in this case.
QUESTION 72
Which of the following is the seating arrangement recommended for a 5-year-old in a family automobile:
1
Lap belt in the middle of the back seat
2
Lap and shoulder belt in the back seat
3
Lap and shoulder belt and booster seat in back
4
Rear-facing child seat in back
5
Lap and shoulder belt and booster seat in front
C hildren ages 4 to 8 (40 lbs to 60 lbs) are at risk for airbag injuries and should not be in the front seat. In addition, they require booster seats to allow proper fitting of the shoulder harness on the upper torso. Rear-facing seats are only appropriate for infants. C hildren should not be in the front seat until after age 12 and over 100 lbs.
QUESTION 73
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?**
1
Contact between the rotator cuff and the posterior-superior labrum
2
Anterior instability
3
A ganglion cyst of the spinoglenoid notch
4
Osteonecrosis of the humeral head
5
Posterior subluxation
Internal impingement of the shoulder is now a well-recognized cause of shoulder pain in the throwing athlete. First described by Walch and associates, it involves contact of the rotator cuff and labrum in the maximally externally rotated and abducted shoulder, such as in the late cocking phase of the throwing motion. Schickendantz and associates have shown this contact to be physiologic in most patients and becoming pathologic with repetitive overhead activity.
REFERENCES: Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
McFarland EG, Hsu CY, Neira C, O’Neil O: Internal impingement of the shoulder: A clinical and arthroscopic analysis. J Shoulder Elbow Surg 1999;8:458-460.
QUESTION 74
Initial repair of the large U-shaped rotator cuff tear shown in Figure 12 consists of closing the tear side-to-side to take advantage of margin convergence. The most significant biomechanical consequence of this repair step results in
1
increased strength of the rotator cuff repair by creating thicker repair construct.
2
decreased size of the defect exposing the humeral head.
3
decreased stress in the rotator cuff at the site of the side-to-side repair.
4
decreased stress in the rotator cuff at the free margin and greater tuberosity interface.
5
decreased stress in the rotator cuff crescent cable.
Margin convergence refers to the phenomenon that occurs with side-to-side closure of large U- or L-shaped rotator cuff tears in which the free margin of the tear converges toward the greater tuberosity as the side-to-side tear progresses. The creation of the converged cuff margin creates decreased strain in the free margin of the repaired cuff, resulting in a decreased strain in the repair sutures. While the size of the humeral head defect is made smaller with side-to-side closure, biomechanically, this is less significant. The mild increase in thickness of the repair at the side-to-side margin is less important than a reduction in stress in the repaired tissue. Stress in the crescent cable region of the cuff actually increases and becomes more physiologic in transmitting force from the cuff to the greater tuberosity.
REFERENCES: Burkhart SS: A stepwise approach to arthroscopic rotator cuff repair based on biomechanical principles. Arthroscopy 2000;16:82-90.
Burkhart SS, Athanasiou KA, Wirth MA: Margin convergence: A method of reducing strain in massive rotator cuff tears. Arthroscopy 1996;12:335-338.
QUESTION 75
A 12-year-old boy sustains open comminuted midshaft tibial and fibular fractures while playing indoor soccer. The wound is grossly clean and measures 7 cm with some periosteal stripping. Antibiotics and tetanus toxoid are administered immediately in the emergency department. Following irrigation and debridement of the wound in the operating room, treatment should include
1
a long leg cast.
2
a reamed nail.
3
an unreamed nail.
4
an external fixator.
5
plates and screws.
Open fractures in children have similar rates of short-term complications such as compartment syndrome, vascular injury, and nerve injury when compared to adult fractures. Primary wound closure should be used for Gustillo and Anderson type 1 or uncomplicated type 2 fractures after surgical debridement. Skeletal stabilization may consist of external fixation, flexible nails, or casting with or without supplementary pin fixation. For an open comminuted midshaft fracture, external fixation is the treatment of choice. Reamed intramedullary nailing is contraindicated in children with an open physis. Plate fixation has a high complication rate in severe open fractures.
REFERENCES: Jones BG, Duncan RD: Open tibial fractures in children under 13 years of age-10 years experience. Injury 2003;34:776-780.
Bartlett CS III, Weiner LS, Yang EC: Treatment of type II and type III open tibia fractures in children. J Orthop Trauma 1997;11:357-362.
Robertson P, Karol LA, Rab GT: Open fractures of the tibia and femur in children. J Pediatr Orthop 1996;16:621-626.
Cullen MC, Roy DR, Crawford AH, et al: Open fracture of the tibia in children. J Bone Joint Surg Am 1996;78:1039-1047.
QUESTION 76
Figures below show the radiographs, MRI, and MR arthrogram obtained from a 25-year-old collegiate
soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy.When counseling patients who have a cam deformity, the orthopaedic surgeon should note that
!img
!img
1
osteoarthritis of the hip is likely to occur later in life.
2
correction prevents later development of osteoarthritis.
3
most acetabular tears are symptomatic, and surgical treatment will be necessary.
4
this is an inherited deformity.
Multiple studies have confirmed that cam or pincer anatomy is commonly present in asymptomatic hips. According to a large systematic review, cam deformities are present in approximately one-third of asymptomatic hips in young adults, and the proportion is higher than 50% in the subgroup of athletes. Ganz and associates proposed that femoral acetabular impingement is the root cause of osteoarthritis in most nontraumatic, nondysplastic hips, and functional improvement with surgical correction of the deformity has been demonstrated. Despite the link between cam deformity and hip osteoarthritis, a corresponding link between the correction of the deformity and prevention of osteoarthritis has never been proven. The results of cam deformity correction, typically including repair of the degenerative labral tear, are much poorer when substantial joint space loss is present. A typical joint space cutoff of 2 mm or less is used to recommend against hip preservation surgery.
QUESTION 77
-Bacterial resistance to tetracycline is confirmed by ribosome protection, tetracycline modification, and
1
altered RNA polymerase.
2
altered membrane binding protein.
3
increased drug efflux.
4
DNA gyrase mutation.
## RESPONSES FOR QUESTIONS 25 THROUGH 27
1. Radiation
2. Ethylene oxide
3. Remelting
4. Annealing
## Ultra-high-molecular-weight polyethylene (UHMWPE) is a commonly used polymer in total hip and knee replacement. Please refer to the list of terms above in reference to UHMWPE and select the most appropriate response to the questions below.
QUESTION 78
A 37-year-old electrician is diagnosed with a frozen shoulder after sustaining an electrical injury at work 2 weeks ago. Examination reveals that he cannot actively or passively externally rotate or abduct the arm. The glenohumeral joint and scapula move in a 1:1 ratio. Radiographs are shown in Figures 15a and 15b. The best course of action
should be**
1
vigorous physical therapy for passive range of motion.
2
manipulation of the shoulder under anesthesia.
3
an intra-articular steroid injection.
4
an axillary radiograph.
5
MRI.
The patient’s history, examination, and radiographs are classic for locked posterior dislocation of the glenohumeral joint. Posterior dislocation of the shoulder remains the most commonly missed dislocation of a major joint. Up to 80% are missed on initial presentation. The primary cause for failure to accurately diagnose this injury is inadequate radiographic evaluation. The typical presentation is a shoulder locked in internal rotation with loss of abduction. An axillary view not only will make the definitive diagnosis but will help assess the size of the articular surface defect and help plan treatment. This view can be done expediently as part of every trauma series. The AP view is suspicious for a posteriorly dislocated humerus with loss of the humeral neck profile, a vacant glenoid sign, and an anterior humeral head compression fracture (reverse Hill-Sachs lesion).
REFERENCES: Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosement, IL, American Academy of Orthopaedic Surgeons, 1997, pp 181-189.
Rockwood CA Jr, Thomas SC, Matsen FA III: Subluxations and dislocations about the glenohumeral joint, in Rockwood CA Jr, Green DP, Bucholz RW (eds): Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, vol 1, pp 1058-1065.
QUESTION 79
Which of the following scoring techniques is the weakest when used to compare specifiCphysical dynamics of a prosthesis:
1
Hospital for Special Surgery knee score
2
Knee Society score
3
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score
4
Iowa knee score
5
Mayo CliniCknee score
The Hospital for Special Surgery knee score and the Knee Society score provide more detailed information about the physical dynamics of a prosthesis than the WOMACscore. A combination of the three scores correlate well in their measurement of total knee replacement outcomes
QUESTION 80
of 100
Figures 16a and 16b are the radiograph and MR image of a 15-year-old dance athlete with 2 weeks of pain at the left distal femur, a limp, and an inability to dance. Knee motion is 0 to 135 degrees with minimal pain and there is no effusion. Her temperature is 37.0°C, WBC is 12000 /µL (rr, 4500-11000 /µL), CRP is 0.8 mg/L (rr, 0.08-3.1 mg/L), and ESR is 21 mm/h (rr, 0-20 mm/h).
1
Aspiration, cultures, surgical irrigation and debridement, and intravenous (IV) nafcillin
2
Aspiration, cultures, surgical irrigation and debridement, and IV vancomycin
3
Aspiration, cultures, Lyme serology, and oral amoxicillin
4
Biopsy, culture, curettage, bone graft, and possible internal fixation
5
Physical therapy, ibuprofen, and an antinuclear antibody test
Figures 14a through 14e show a 13-year-old boy with osteomyelitis of the distal tibia and a large subperiosteal abscess. The patient has failed treatment with IV ceftriaxone, and methicillin-resistant Staphylococcus aureus infection is likely. Aspiration, cultures, irrigation and debridement, IV vancomycin, an infectious disease consult, and an evaluation for possible deep vein thrombosis is prudent initial treatment. Figure 15a through 15c show a 7-year-old girl who sustained a deer tick bite while vacationing in Connecticut. She has Lyme arthritis and a Lyme “bulls-eye” rash on the same leg. Aspiration, cultures, Lyme serology, and oral amoxicillin for 30 days is prudent initial treatment. Figures 16a and 16b are the radiograph and MR image of a 15-year-old dance athlete with a probable minor fracture via a benign cyst of the distal femur. The geographic cyst may be a nonossifying fibroma, eosinophilic granuloma, Brodie abscess, or simple bone cyst. Biopsy, culture, curettage and bone graft, and possible internal fixation is reasonable initial treatment.
Figure 17
QUESTION 81
**An orthopaedic surgeon in his first year of practice is negotiating with a private for-profit hospital to be their employed trauma specialist. The state of employment is known to have a high rate of malpractice claims because of a favorable plaintiff legal environment. During the course of negotiations, malpractice insurance is being discussed. The surgeon should ask the hospital to provide which type of malpractice insurance policy?**
1
Claims made with "nose" coverage
2
Claims made without tail coverage
3
No policy because of employed status and sovereign immunity
4
Occurrence coverage
5
Occurrence coverage with "nose" coverage
#
**
An occurrence policy provides coverage for all claims made during employment irrespective of when it is filed (during or postemployment) and therefore is the best option. Claims made policy only covers suits for the time employed. A prepurchased "tail" is needed to provide coverage for cases that occurred during employment but filed postemployment. Nose coverage is applicable if the surgeon was previously employed and did not have tail coverage from previous employment, but this surgeon just emerged from training where it is not applicable. Claims made without tail coverage is unwise because the surgeon would be unprotected or have to purchase his own policy postemployment.
Only in certain situations does sovereign immunity exist, and generally not in a for-profit system. Occurrence coverage with nose coverage
is incorrect because it does not apply to this surgeon with no previous employment or claims policy lacking tail coverage.
QUESTION 82
of 100
#### A 12-year-old boy with a history of Duchenne muscular dystrophy is being evaluated for progressive scoliosis. He now has 35° long thoracolumbar scoliosis, which was 20° only 6 months ago. He has a pelvic obliquity of 20°. He is a full-time wheelchair user. What is the most appropriate next step for this patient's spine deformity care?
####
1
Immediate bracing for at least 20 hours a day until skeletal maturity
####
2
If he is not on glucocorticoids, consider to start
####
3
Posterior spinal fusion and instrumentation down to pelvis
####
4
Posterior spinal fusion and instrumentation down to L5
#### ■
#### Duchenne muscular dystrophy is a recessive, X-linked, inherited disorder. Most (90%) untreated boys with this disorder develop progressive scoliosis, secondary to muscle weakness, after becoming full-time wheelchair users. Several studies suggest that the long-term use of glucocorticoids has prolonged effects against detrimental aspects of Duchenne muscular dystrophy.
#### The widespread use of glucocorticoids for patients with Duchenne muscular dystrophy has dramatically decreased the development of scoliosis and need for subsequent surgical intervention. There is still much to be learned about the impact of glucocorticoids on the spine, including the duration of glucocorticoid treatment needed to reduce the risk of a progressive curve and whether this treatment merely delays the onset. In recent studies in which researchers followed young men into their twenties, it was shown that glucocorticoids protect against the development of scoliosis well past skeletal maturity.
#### Posterior spinal instrumentation and fusion are recommended in those whose spinal curve is >20°, are prepubertal, and are not on glucocorticoids because progression of the curve is expected. Although patients taking glucocorticoids may still develop a scoliosis, it is reasonable to wait until progression is documented. When surgery is done to correct scoliosis, it is recommended that those with a pelvic obliquity of >15° also have stabilization and fusion into the pelvis. This helps patients with seating and positioning. Fusion to the L5 is sufficient for patients who do not have a severe pelvic obliquity. With surgical intervention of the spine, the aim is to reduce the patient’s pain, improve his ability to sit comfortably, and prevent further progression.
####
QUESTION 83
of 100
If the culture results are positive, which treatment will most likely resolve the infection?
1
Arthroscopic debridement
2
Intravenous antibiotics
3
Single-stage revision
4
Double-stage revision
Osteolysis of this magnitude is uncommon in the setting of an uncemented hemiarthroplasty. Further workup for infection is indicated, such as aspiration under fluoroscopy or ultrasound. Infection needs to be ruled out before proceeding. Observation and physical therapy are not indicated. Arthroscopy has been shown in several studies to have greater sensitivity and specificity than aspiration and can be especially effective to obtain cultures of slow-growing organisms such as Propionibacterium acnes. Blood tests are unreliable, and a bone scan would not reliably differentiate between loosening and infection. Arthroscopic debridement would not be reliable for treatment. Intravenous antibiotics can be used for suppression, but the best results in terms of resolving the infection would be achieved with 2-stage revision.
RECOMMENDED READINGS
31. [Dilisio MF, Miller LR, Warner JJ, Higgins LD. Arthroscopic tissue culture for the evaluation of periprosthetic shoulder infection. J Bone Joint Surg Am. 2014 Dec 3;96(23):1952-8. doi: 10.2106/JBJS.M.01512. PubMed PMID: 25471909. ](http://www.ncbi.nlm.nih.gov/pubmed/25471909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25471909)
32. Hersch JC, Dines DM. Arthroscopy for failed shoulder arthroplasty. Arthroscopy. 2000 Sep;16(6):606-
[12/. PubMed PMID: 10976121. ](http://www.ncbi.nlm.nih.gov/pubmed/10976121)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10976121)
33. [Foruria AM, Fox TJ, Sperling JW, Cofield RH. Clinical meaning of unexpected positive cultures (UPC) in revision shoulder arthroplasty. J Shoulder Elbow Surg. 2013 May;22(5):620-7. doi: 10.1016/j.jse.2012.07.017. Epub 2012 Sep 13. PubMed PMID: 22981448. ](http://www.ncbi.nlm.nih.gov/pubmed/22981448)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22981448)
QUESTION 84
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5° of angulation. When the MCP joint is flexed 30°, a radially directed stress produces 45° of angulation. Radiographs are otherwise normal. Management should consist of
1
a thumb spica cast and reassessment in 3 weeks.
2
a thumb spica cast and reassessment in 6 weeks.
3
repair of the ulnar collateral ligament of the MCP joint.
4
adductor pollicis advancement on the proximal phalanx.
5
repair of the MCP joint dorsal capsule.
Injuries to the ulnar collateral ligament of the MCP joint of the thumb commonly occur in recreational skiers. Historically, this injury has been referred to as “gamekeeper’s thumb.” The ligament consists of the proper collateral ligament and the more volar accessory collateral ligament. In extension, the accessory ligament is taut, and in flexion, the proper ligament is taut. For a complete tear of the ligament complex to occur, there must be laxity in full extension. Incomplete tears respond well to thumb spica splinting or casting for 2 to 3 weeks and gradual resumption of range of motion. Prolonged immobilization of incomplete injuries leads to higher rates of MCP joint stiffness.
REFERENCES: Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint.
J Am Acad Orthop Surg 1997;5:224-229.
QUESTION 85
##### A 14-year-old boy is lifting weights and feels a sudden pain in his back, associated with sciatica bilaterally. The sciatica persists for several weeks. The radiograph shown in Figure 7a is negative, and the CT scan shown in Figure 7b is available for evaluation. An MRI scan is read as a disk bulge. Management should consist of
#####
1
##### resection of the fragment through a microdiskectomy approach.
2
##### epidural steroid injections until symptoms improve.
3
##### laminectomy with surgical excision of the limbus fragment.
4
##### activity restrictions until the symptoms improve.
5
##### chiropractic manipulation.
#####
#####
#####
##### DISCUSSION: A limbus or apophyseal fracture caused by heavy lifting or twisting is commonly seen in older children and adolescents. Patients describe feeling a popping sensation and report radicular symptoms. Radiographs usually are not sufficient to diagnose the injury. MRI or CT should be used to determine the exact location of the fracture. Nonsurgical management is rarely successful. A wide laminectomy with surgical excision of the limbus fragment is recommended if neurologic symptoms are present.
#####
##### REFERENCE: Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, p 694.
#####
#####
##### **2010 Pediatric Orthopaedic Examination Answer Book • 13**
#####
##### Figure 8
#####
QUESTION 86
The most common risk factors for stress fractures is:
1
Leg length discrepancy
2
Training regimen
3
Muscle strength
4
Low bone mineral density
5
Footwear
Numerous risk factors for stress fracture exist. Most commonly, the scenario is doing âtoo much too soon.â Survey data have shown 86% of runners suffering stress fracture have had a change in duration, frequency, or intensity of training immediately prior to injury. The best independent predictors for stress fracture development in women appear to be age of menarche and calf girth
QUESTION 87
Talar body fractures are best classified by a fracture line:
1
That extends superiorly into the trochlea
2
That extends anywhere posterior to the talar neck
3
That extends inferiorly, posterior to the lateral process
4
That extends inferiorly, anterior to the lateral process
5
That extends into the talar head
Talar neck and body fractures can be difficult to distinguish, especially when they extend superiorly into the anteromedial aspect of the trochlea. These two fractures have a different prognosis. The authors recommend classification of these fractures based on the inferior fracture line; if anterior to lateral process of the talus, then it is a neck fracture; if posterior to lateral process of the talus, then it is a body fracture.
QUESTION 88
Slide 1
A 23-year-old carpenter fell off a roof 4 weeks ago. He has pain in the ankle and a deformity. The lateral radiograph is presented (Slide). Which of the following treatments is most likely to return this patient to work with a functioning foot and ankle:
1
Open reduction internal fixation of the calcaneus fracture
2
Short leg cast, no weight bearing for 8 weeks, followed by physical therapy
3
Immediate vigorous physical therapy emphasizing range of motion
4
Open reduction internal fixation of the calcaneus fracture with primary subtalar arthrodesis
5
Physical therapy, followed by subtalar arthrodesis at 6 months
The calcaneus fracture is associated with subluxation of the subtalar joint, giving the appearance of injury to the talus and calcaneus. The true extent of the injury cannot be determined without a computed tomography scan; however, the question is not as to the outcome of treatment, but the ability to return this patient to his occupation. At 4 weeks following injury, while open reduction internal fixation of the fracture is possible, anatomic reduction may be difficult. The most likely means of returning this patient to work is with early arthrodesis, which should be combined with an open reduction internal fixation of the calcaneus.
QUESTION 89
An 19-year-old male presents to the emergency room following an motor vehicle accident as an unrestrained driver. Examination reveals unilateral jugular vein engorgement. Chest and special view
# radiographs are seen in Figures A and B respectively. Following CT scan of the chest, the next step in management is
!img
!img
1
Nonsurgical management and follow-up CT scan in 6 weeks
2
Closed reduction in the emergency room under sedation
3
Closed reduction in the operating room under general anesthesia with thoracic surgery on standby, followed by immobilization for 4 weeks
4
Closed reduction in the operating room under general anesthesia with thoracic surgery on standby, followed by compression plating
5
Open reduction in the operating room under general anesthesia, followed by transarticular pinning with K-wires
This patient has a right posterior sternoclavicular (SC) dislocation. Management involves closed reduction and bracing. Closed reduction should be performed with a thoracic surgeon available in the event of mediastinal involvement.
The SC joint can dislocate anteriorly or posteriorly. Posterior dislocations are first treated with closed reduction. If closed reduction fails, open reduction is indicated. Early complications of posterior SC dislocation include pneumothorax, laceration/erosion/occlusion of great vessels, esophageal rupture and brachial plexus compression. Late complications include tracheoesophageal fistula, stridor and dysphagia.
Groh et al. reviewed traumatic SC injuries. Reduction maneuvers in posterior SC dislocation include: (1) traction on the arm and slowly bringing it into extension, (2) traction with the arm in adduction and posterior pressure applied to the shoulder, and (3) pulling anteriorly on a towel clip encircling the medial clavicle. Chronic instability after posterior SC dislocations can be managed with figure-of-8 semitendinosus graft or medial clavicle resection and reattachment of the clavicle to the first rib with dacron tape.
Glass et al. performed a systematic review on SC dislocations. They found mediastinal compression occurred 30% of the time with posterior dislocations.
Figures A and B are radiographs demonstrating asymmetry of the SC joints, characteristic of a right posterior SC dislocation (Figure B is not a serendipity view). Illustration A demonstrates how in POSTERIOR dislocation, the clavicle appears INFERIOR, and in ANTERIOR dislocation, the clavicle appears SUPERIOR on a serendipity view radiograph respectively. Illustration B shows the imaging technique for a serendipity view radiograph. Illustration C is a reconstructed CT image of the patient showing left posterior SC dislocation.
Incorrect Answers:
Answer 1: Nonsurgical management is not advised because of potential complications of posterior dislocations. Unstable dislocations will remain dislocated at 6 weeks if untreated.
Answer 2: Closed reduction in the emergency room is ill-advised because of potential mediastinal involvement. An operating room and thoracic surgeon should be available during the reduction maneuver.
Answer 4: Compression plating across the sternoclavicular joint is not recommended.
Answer 5: Pinning with K-wires is contraindicated because of potential catastrophic consequences of wire migration.
QUESTION 90
A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman test with a soft endpoint, varus laxity at 30°, and a positive dial test at 30° that dissipates at 90° of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. Radiographic alignment is neutral. What treatment is most likely to lead to a successful outcome?
1
Revision ACL reconstruction
2
Revision ACL reconstruction and posterior cruciate ligament (PCL) reconstruction
3
Revision ACL reconstruction and posteromedial corner reconstruction
4
Revision ACL reconstruction and posterolateral corner reconstruction
The patient underwent an ACL reconstruction that has now failed. Based on his examination, he also has a posterolateral corner injury. Because this concomitant injury was not treated, the patient had undue strain on his graft, resulting in ultimate failure. Hamstring grafts are as effective as other graft types for ACL reconstruction. The medial meniscus provides secondary stabilization to the knee; however, this patient has a missed lateral ligamentous injury, and meniscus tears do not result in the development of a varus thrust. An unrecognized PCL tear likely results in mild-to-moderate medial and patellofemoral osteoarthritis without significant lateral laxity and thrust.
39
QUESTION 91
Figure 30 shows the radiograph of a 38-year-old man who reports persistent pain laterally and plantarly about the fifth metatarsal head. Examination reveals calluses dorsolaterally and plantarly about the fifth metatarsal head. Nonsurgical management has failed to provide relief. Surgical treatment should include
1
simple lateral eminence resection.
2
distal chevron osteotomy of the fifth metatarsal.
3
oblique mid-diaphyseal osteotomy of the fifth metatarsal.
4
proximal diaphyseal osteotomy of the fifth metatarsal.
5
excision of the fifth metatarsal head.
The patient has painful lateral and plantar keratoses with metatarsus quintus valgus deformity. This combination of problems is best addressed with an oblique mid-diaphyseal osteotomy that allows the distal metatarsal to be displaced medially and dorsally. Lateral eminence resection alone will not address the painful plantar keratosis. A distal chevron osteotomy has a more limited ability to address the plantar keratosis (if translated medially and slight dorsally). Proximal diaphyseal osteotomies of the fifth metatarsal are associated with an increased risk of delayed union or nonunion secondary to the relative hypovascularity in the proximal diaphysis. Excision of the fifth metatarsal head can result in a floppy fifth toe and transfer metatarsalgia.
REFERENCES: Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Moran MM, Claridge RJ: Chevron osteotomy for bunionette. Foot Ankle Int 1994;15:684-688.
QUESTION 92
A 9-month-old infant with torticollis has failed to gain weight and has recurrent lower respiratory tract infections. Neurologic examination is normal, and there is no palpable mass in the sternocleidomastoid muscle. Radiographs of the neck show no bony anomalies. Management should now include
1
a skeletal survey.
2
audiometric screening.
3
physical therapy for stretching.
4
contrast studies of the upper gastrointestinal tract.
5
reassurance to the parents that there is no underlying pathology.
QUESTION 93
-Decreased sun exposure leads to decreased bone health via what mechanism?
1
Impaired ability of the liver to hydroxylate cholecalciferol
2
Impaired ability of the kidneys to hydroxylate cholecalciferol
3
Impaired parathyroid hormone (PTH) production by the parathyroid glands
4
Impaired absorption of calcium by the gastrointestinal (GI) tract
QUESTION 94
The strongest portion of the scapholunate interosseous ligament (SLIL) is the:
1
Proximal
2
Distal
3
Volar
4
Dorsal
5
Dorsal intercarpal
The SLIL is a c-shaped structure, which is thickest dorsally. The dorsal fibers have an average thickness of 3 mm and are composed of transversely oriented fibers, which afford the greatest resistance to translation between the scaphoid and the lunate, preventing the characteristic radiographic separation and flexion deformity of the scaphoid.
QUESTION 95
A 22-year-old patient underwent successful reduction of a posterolateral elbow dislocation. Management should now consist of
1
splinting for 5 weeks.
2
active range-of-motion exercises after 1 to 3 days.
3
delayed passive stretching at 2 weeks.
4
open medial collateral ligament reconstruction.
5
open lateral collateral ligament reconstruction.
The elbow usually is stable after reduction in most elbow dislocations. Ross and associates reported that supervised motion begun immediately after reduction was effective in uncomplicated dislocations. The elbow will become stiff if immobilization is applied for an extended period of time. Immediate open treatment is not indicated for a simple elbow dislocation.
REFERENCES: Ross G, McDevitt ER, Chronister R, et al: Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med 1999;27:308-311.
O’Driscoll SW, Jupiter JB, King GJ, et al: The unstable elbow. J Bone Joint Surg Am 2000;82:724-738.
QUESTION 96
C omplete ischemia of a peripheral nerve results in irreversible damage after hours.
1
1 to 2 hours
2
2 to 4 hours
3
4 to 6 hours
4
6 to 8 hours
5
8 to 10 hours
Loss of nerve electrical conduction begins after 2 hours of complete ischemia. Peripheral nerves can tolerate up to 4 hours of complete ischemia. A neurapraxic (loss of conduction capability) injury usually recovers. After 8 hours of complete ischemia, nerves cannot recover.
Patients will lose the sense of pain in a compartment with total ischemia after 2 to 8 hours because there is no conduction to the nerve. One can expect little recovery once this painless state has occurred.
QUESTION 97
Which of the following resist articular cartilage compression and fluid flow:
1
Biglycan
2
Type II collagen fibers
3
Glycosaminoglycan aggregates
4
Anchorin II
5
Tidemark
Type II collagen fibers resist tensile and shear deformation forces in the articular cartilage.
In contrast, the glycosaminoglycan aggregates resist articular cartilage compression and fluid flow.
QUESTION 98
of 100
The pathogenesis of this condition is associated with
1
a PITX1 mutation.
2
a point polymorphism in a regulatory sequence for the COLIA-1 gene.
3
mutations in the EXT gene family.
4
mutations in the COL5A or COL3A genes.
- a PITX1 mutation.
QUESTION 99
Which of the following is an effective medication for osteopetrosis:
Interferon gamma-1 is the only treatment for osteopetrosis that is approved by the Food and Drug Administration
QUESTION 100
An otherwise healthy 31-year-old man has had right knee pain for the past 9 months. His former physician
administered a cortisone injection and ordered 6 months of physical therapy. The patient later had an arthroscopy with debridement of the right knee by another physician and completed another course of physical therapy. The patient received minimal relief from these treatments and still is not able to walk longer distances or go on hikes. On examination, he is a healthy appearing male with a body mass index of 24 kg/m2. He has a small effusion, minimal quadriceps atrophy, no tenderness about the knee, full range of motion, stable to varus and valgus stress at 30° of flexion, a grade 1 Lachman test, and a normal posterior drawer. Figures 1 through 4 are his arthroscopic views, radiograph and MRI scan from his prior surgical procedure. What is the next most appropriate step in treatment?
!img
!img
!img
!img
!img
!img
!img
!img
!img
1
Bracing with physical therapy focusing on quadriceps/vastus medialis obliquus (VMO) and hamstring strengthening
2
Osteotomy
3
Osteochondral allograft to femoral condyle
4
Arthroscopy with femoral condyle microfracture
The patient has a symptomatic cartilage lesion of his medial femoral condyle, which has not responded to nonsurgical measures, and he failed a prior arthroscopy with debridement. Based on his examination and imaging, he is ligamentously stable, has normal mechanical alignment, and has intact menisci, making him a candidate for a cartilage restoration procedure. The accompanying MRI also indicates subchondral bone involvement with increased T2 signal underlying the cartilage defect. Osteochondral allograft is the only choice that addresses both the cartilage defect, as well as compromised subchondral bone. Depending on lesion size, osteochondral autograft transfer may also be considered, but this is not presented as an answer choice.Given the radiographic finding of neutral mechanical alignment, bracing would be less effective, and the patient has already tried extensive physical therapy. Lack of malalignment also excludes tibial osteotomy as a preferred answer choice. Microfracture is best for small cartilage lesions without _significant bone marrow involvement._