Operative Management of Patella Fractures: A Comprehensive Guide
Key Takeaway
Patella fractures account for approximately 1% of all skeletal injuries, disrupting the knee's extensor mechanism and patellofemoral articulation. Management hinges on restoring articular congruity and extensor continuity. While undisplaced fractures may be managed nonoperatively, displaced fractures or those with retinacular disruption require rigid internal fixation. Techniques such as modified tension band wiring or cannulated screw fixation allow for early mobilization, optimizing functional recovery and minimizing post-traumatic arthrosis.
Introduction to Patella Fractures
Fractures of the patella constitute approximately 1% of all skeletal injuries. As the largest sesamoid bone in the human body, the patella plays a critical biomechanical role by increasing the moment arm of the quadriceps tendon, thereby enhancing the mechanical advantage of the extensor mechanism. Injuries to the patella result from either direct or indirect trauma, and frequently, a combination of both forces.
The anterior subcutaneous location of the patella renders it highly vulnerable to direct trauma, such as the knee striking the dashboard during a motor vehicle collision or from a direct fall onto the anterior aspect of the knee. These direct-impact injuries are typically comminuted or displaced and are frequently associated with severe chondral injury to the distal femur or the patellar articular surface itself.
Conversely, fractures caused by indirect mechanisms typically result from a violent, eccentric contraction of the quadriceps muscle against a flexed knee. These fractures are usually transverse in configuration and are highly likely to be associated with significant tears of the medial and lateral retinacular expansions. The most significant clinical consequences of a patellar fracture are the loss of continuity of the extensor mechanism and the potential for post-traumatic arthrosis due to incongruity of the patellofemoral articulation.
Clinical Evaluation and Diagnosis
Patients with patellar fractures generally present with an acute hemarthrosis, localized anterior knee pain, and focal tenderness. In fractures that are significantly displaced or accompanied by concomitant retinacular tears, a palpable defect (step-off) may be present between the fracture fragments.
Clinical Pearl: The inability of the patient to actively extend the affected knee or perform a straight-leg raise (SLR) is the hallmark sign of a disrupted extensor mechanism and a torn retinaculum. This clinical finding is an absolute indication for surgical intervention.
Occasionally, active knee extension is limited purely by pain rather than mechanical disruption. In such ambiguous cases, the hemarthrosis can be aspirated under strict sterile conditions, followed by an intraarticular injection of local anesthetic (e.g., lidocaine). Once the pain is relieved, the patient should be reassessed; if the extensor mechanism is intact, active knee extension will be restored.
Evaluating Open Fractures
An open wound in the vicinity of a patellar fracture must be treated with a high index of suspicion for an open fracture, which constitutes an orthopedic surgical emergency. If uncertainty exists regarding whether a traumatic wound communicates with the knee joint, a saline load test is mandatory.
Under sterile conditions, an 18-gauge needle and a 50-mL syringe are used to aspirate the knee joint (often yielding hemarthrosis). Leaving the needle in place, 50 mL of sterile saline is injected into the joint. If the saline flows out through the traumatic wound, the fracture is definitively open. Note that this test may not be 100% reliable in cases of very small traumatic arthrotomies where tissue planes act as a one-way valve.
Radiographic Evaluation
Standard radiographic evaluation of a suspected patellar fracture must include anteroposterior (AP), lateral, and axial (Merchant or skyline) views.
- Lateral View: Best for visualizing transverse fractures and assessing the degree of fragment displacement and articular step-off.
- Axial View: Essential for evaluating vertical fractures, marginal fractures, osteochondral injuries, and patellofemoral joint congruity.
- Comparison Views: A contralateral knee radiograph is occasionally necessary to differentiate an acute fracture from a bipartite patella. A bipartite patella represents a failure of fusion (usually of the superolateral pole), features smooth, sclerotic margins, and is bilateral in the majority of cases.
Classification of Patella Fractures
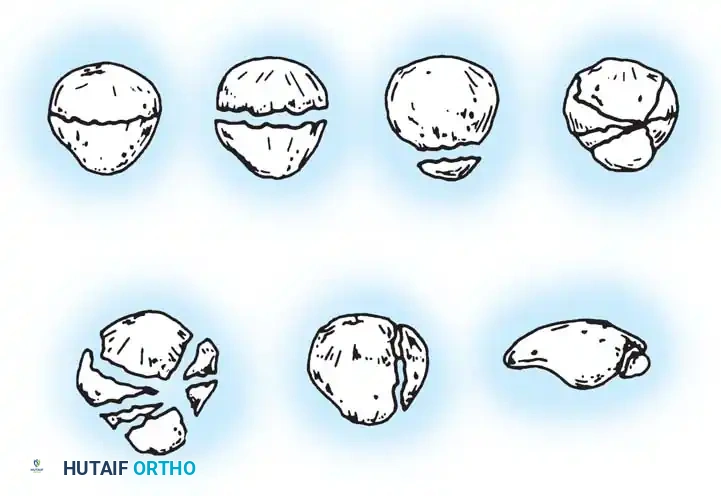
Patellar fractures are broadly classified as undisplaced or displaced, and are further subclassified according to their specific geometric configuration.
- Transverse Fractures: The most common pattern. They usually involve the central third of the patella but can also occur at the proximal (apical) or distal (basal) poles. A variable amount of comminution may be present at the poles.
- Vertical Fractures: Usually involve the middle and lateral thirds of the patella. If only the extreme medial or lateral edge is affected, it is termed a marginal fracture. Displacement and retinacular disruption rarely occur in vertical fractures.
- Comminuted/Stellate Fractures: Result from high-energy direct trauma and are associated with a variable amount of displacement and severe articular cartilage damage.
- Osteochondral Fractures: Often associated with patellar dislocations, involving shearing of the articular cartilage and underlying subchondral bone.
Indications for Treatment
Nonoperative Management
Closed fractures with minimal displacement, minimal articular incongruity, and an intact extensor retinaculum can be successfully managed nonoperatively. Boström established widely accepted criteria for nonoperative treatment:
* Fragment separation (diastasis) of less than 3 to 4 mm.
* Articular incongruity (step-off) of less than 2 to 3 mm.
Nonoperative treatment consists of immobilizing the knee in extension in a cylinder cast or a rigid hinged knee brace locked in extension for 4 to 6 weeks. Weight-bearing is generally allowed as tolerated in full extension. In Boström's long-term follow-up study, fractures meeting these criteria and treated nonoperatively yielded the best overall functional results. However, Edwards, Johnell, and Redlund-Johnell demonstrated that patients with more than 2 mm of diastasis or 1 mm of incongruity frequently developed chronic complaints and reduced quadriceps strength if treated nonoperatively.
Operative Management
Operative intervention is indicated for:
1. Fractures associated with extensor mechanism failure (inability to perform a straight-leg raise).
2. Open fractures.
3. Fractures with greater than 2 to 3 mm of displacement or articular incongruity.
The primary surgical goals are the anatomic restoration of articular congruity and the robust repair of the extensor mechanism, utilizing fixation secure enough to permit early postoperative range of motion (ROM). Delaying surgery unfavorably affects the outcome; however, if severe soft-tissue contusions or abrasions are present and become superficially infected, surgery must be delayed for 7 to 10 days until the soft-tissue envelope recovers and the risk of deep infection is minimized.
Surgical Techniques and Biomechanics
Accepted methods for operative fixation include a variety of wiring techniques, cannulated screw fixation, partial patellectomy, and, rarely, total patellectomy.
Tension Band Wiring Principles
Wiring techniques are most frequently utilized for transverse fractures. The fundamental biomechanical principle of the tension band is the conversion of tensile forces acting on the anterior cortex of the patella (generated by the quadriceps) into compressive forces at the articular surface during knee flexion.
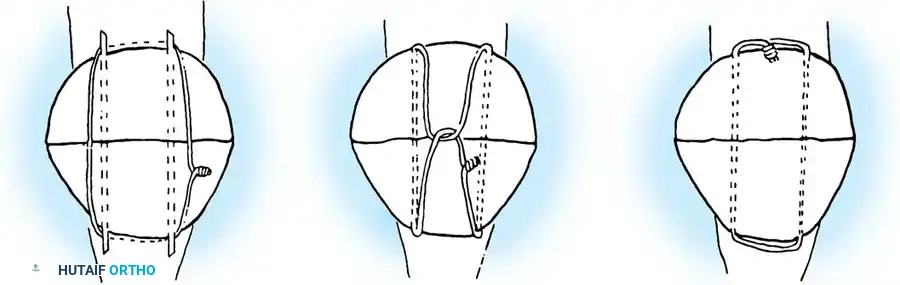
Weber et al. experimentally compared the rigidity of various constructs, including circumferential wiring, standard tension band wiring, Magnusson wiring, and modified tension band wiring (utilizing two anteriorly placed wires combined with two transfixing longitudinal Kirschner wires). They concluded that the most secure fixation was achieved with the modified tension band wiring technique. Weber emphasized anchoring the fixation wire directly into the bone rather than threading it solely through the soft tissues if early motion is to be initiated.
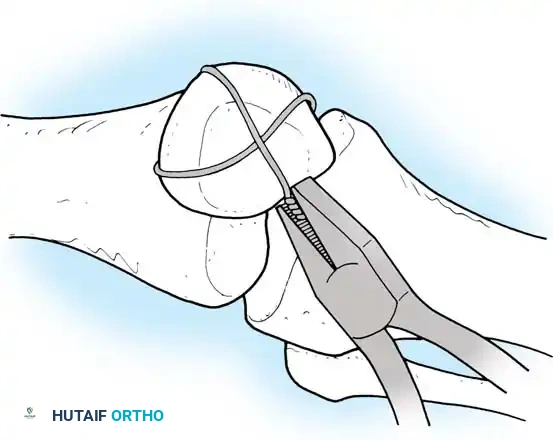
Surgical Warning: When tensioning the wire, ensure symmetric tightening. Use heavy pliers or a wire tensioner to pull the wire taut before twisting, ensuring the twist does not simply coil upon itself but actively compresses the fracture site.
Alternative Wiring Configurations
Various wiring configurations have been described to address specific fracture patterns, particularly when comminution is present.
- Pyrford Technique: Described by Curtis, this involves a circumferential cerclage wire combined with a second tension band wire passed through the tendon. Cadaveric studies show this provides improved fixation in comminuted fractures.
- Lotke Longitudinal Anterior Band Wiring: Utilizes heavy non-absorbable sutures or wires passed longitudinally.
- Magnuson Wiring: An older technique utilizing a continuous wire woven through the proximal and distal tendons.
Benjamin et al. evaluated these techniques and found the modified tension band technique provided superior fixation, particularly in osteopenic bone.
Cannulated Screw Fixation with Tension Band
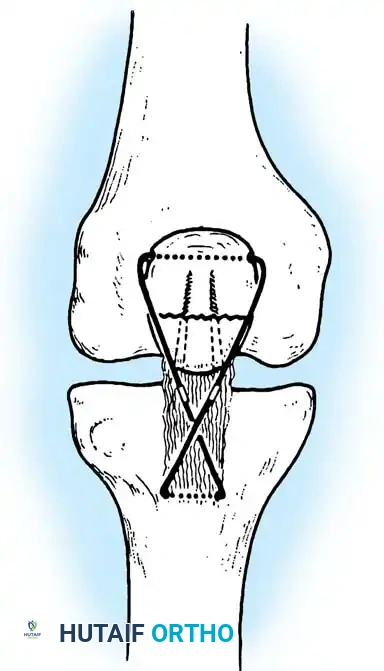
Recent biomechanical advancements have popularized the use of cannulated screws combined with a tension band wire. Carpenter et al. demonstrated that transverse fractures fixed with a tension band wire passed through parallel cannulated screws failed at the highest load compared to K-wires or screws alone.
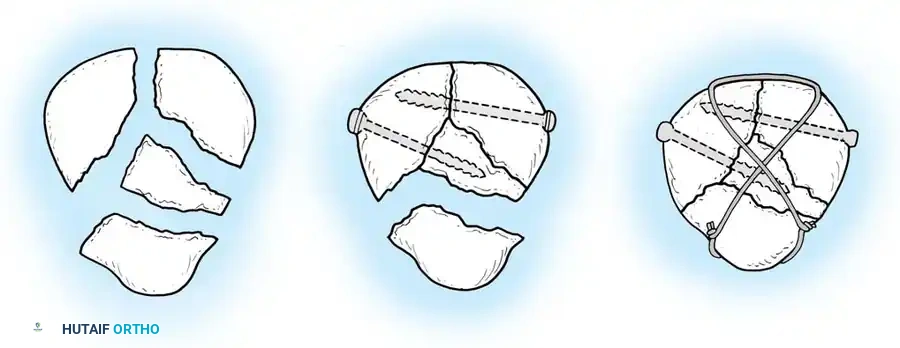
Berg described the fixation of displaced transverse fractures using a figure-of-eight wire passed through parallel cannulated compression screws. Advantages of this construct include:
* A low-profile construct that minimizes hardware irritation (a common complication of K-wires backing out).
* Enhanced interfragmentary compression provided by the lag screws.
* Superior biomechanical stability allowing for aggressive early restricted motion.
* Utility as a salvage method following the failure of traditional tension band wiring.
For transverse fractures with large, robust fragments, a tension band modified with cannulated screws is currently the preferred technique. If peripheral comminution is present, a supplemental circumferential cerclage wire can be added.
Partial and Total Patellectomy
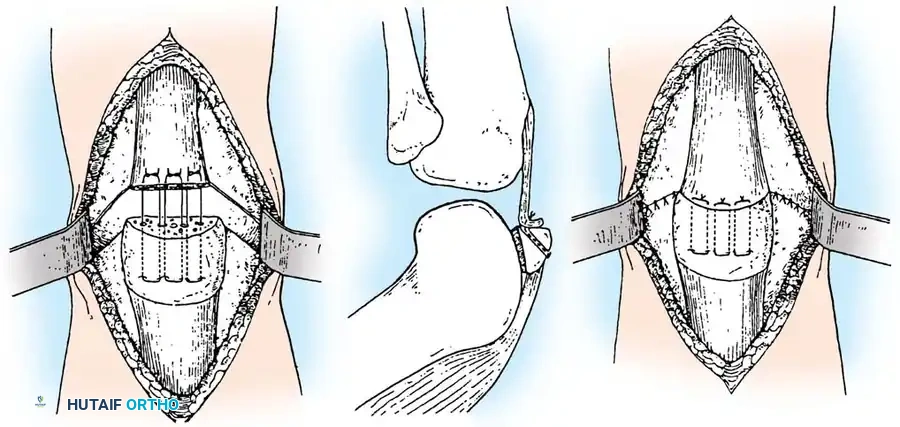
When severe comminution involves the extreme proximal or distal pole, making stable internal fixation impossible, a partial patellectomy is indicated.

The goal is to preserve as much viable patellar bone stock as possible to maintain the mechanical advantage of the extensor mechanism. The comminuted fragments are excised, and the patellar tendon (or quadriceps tendon) is reattached to the remaining healthy bone using heavy non-absorbable sutures passed through longitudinal transosseous drill holes.
Total patellectomy is strictly considered a salvage procedure for irreparable, severely comminuted fractures where no viable articular surface can be reconstructed. It results in a significant loss of quadriceps strength and alters knee kinematics, leading to long-term functional deficits.
Arthroscopically Assisted Percutaneous Fixation
For select transverse fractures with minimal comminution, arthroscopically assisted percutaneous screw fixation has been described. Tandogan et al. and Turgut et al. reported excellent outcomes with full restoration of knee ROM. Makino et al. successfully utilized arthroscopically assisted percutaneous screw and tension band fixation, allowing patients to return to their pre-fracture functional levels with minimal soft-tissue morbidity.
Management of Open Patella Fractures
Open fractures of the patella require immediate surgical intervention. The protocol includes emergent administration of intravenous antibiotics, tetanus prophylaxis, and urgent operative debridement and irrigation.
Torchia and Lewallen reviewed 47 open patellar fractures, noting a deep infection rate of 10.7%. They observed that fractures treated with cerclage wiring were more likely to become infected, likely due to the extensive soft-tissue stripping required to pass the wire circumferentially. Therefore, in open fractures, soft-tissue stripping must be kept to the absolute minimum necessary to stabilize the fracture.
Catalano et al. reported on 79 open patellar fractures treated with ORIF and extensor mechanism repair, achieving good or excellent knee scores in the vast majority of patients. They strongly recommended procedures that preserve bone stock and reestablish extensor integrity, reserving total patellectomy only for unsalvageable cases. Early soft-tissue coverage (within 5 days) is paramount to reducing the incidence of deep infection.
Associated Complex Knee Trauma: Tibial Plateau and Condylar Fractures
High-energy trauma resulting in patellar fractures may also cause severe concomitant injuries to the proximal tibia. The management of these complex periarticular injuries requires advanced reconstructive techniques.
External Fixation for Tibial Shaft and Condylar Involvement
When extensive comminution of the tibial shaft or condyles precludes standard internal plating, circular external fixation (Ilizarov technique) is a powerful tool.
- Frame Construction: Temporarily place the proximal ring below the level of condylar involvement. After achieving condylar reduction, the ring is slid proximally on threaded rods to the level of the fibular head, and all proximal wires are attached to this fixation ring.
- Distal Fixation: Position the middle ring just distal to any shaft fracture component, and place the distal ring at the level of the ankle joint. If extensive shaft comminution is present, apply an additional ring to the midportion of the shaft to complete a four-ring frame.
- Alignment: Attach the proximal ring to the proximal wires, ensuring the ring is perfectly parallel to the joint line. Pass a distal transfixion wire at the level of the distal tibia, parallel to the ankle joint. Tensioning this wire forces the proximal and distal rings to become parallel, thereby restoring the mechanical axis of the lower extremity.
- Fibular Buttress: The fibular head can be utilized as a biological buttress plate. By placing an olive wire obliquely through the fibular head and into the lateral tibial condyle, tensioning the wire compresses the fibular head directly onto the lateral condyle, supporting the articular reduction.
Aftertreatment: Weight-bearing is delayed for approximately 3 months to allow intraarticular fracture lines and bone grafts to consolidate. Once radiographic union is confirmed, the external fixation frame is removed, and the patient is transitioned to a hinged knee brace to facilitate aggressive rehabilitation.
Osteochondral Autografts for Comminuted Lateral Tibial Condylar Fractures
In rare instances of catastrophic knee trauma, Wilson and Jacobs described an innovative salvage method for treating severely depressed, unsalvageable comminuted fractures of the lateral tibial condyle.
In this procedure, the patella is entirely excised and utilized as an osteochondral autograft to replace the destroyed articular surface of the lateral tibial condyle.
* Indications: This operation is not indicated for standard split fractures or typical depressions. It is strictly reserved for extreme comminution where restoration of a functional articular surface using standard elevation and grafting is impossible.
* Outcomes: Jacobs reported 13 knees treated with this technique, all yielding satisfactory results with stable, painless knees and complete extension (flexion varied from 50 degrees to normal).
* Surgical Pearl: Reconstruction of the condyle with an autogenous patellar graft is often preferable to a massive prosthetic implant in the acute trauma setting. However, extreme caution must be exercised during graft preparation. If the transplanted patella is "wafered" too thinly, demonstrable osteonecrosis and subsequent structural collapse will occur. When prepared correctly, the patella gradually incorporates into the tibial condyle, providing a durable biological articular surface.
Postoperative Rehabilitation
Successful outcomes following patella fracture fixation rely heavily on meticulous postoperative rehabilitation.
- Phase I (0-2 weeks): The knee is immobilized in a hinged knee brace locked in full extension. Weight-bearing as tolerated (WBAT) in extension is permitted. Isometric quadriceps sets and straight-leg raises are initiated immediately to prevent muscular atrophy.
- Phase II (2-6 weeks): If rigid fixation (e.g., modified tension band with cannulated screws) was achieved, progressive passive and active-assisted ROM is initiated. Flexion is typically advanced by 30 degrees every 1-2 weeks, protecting the repair from excessive eccentric loads.
- Phase III (6-12 weeks): Once radiographic evidence of consolidation is present, the brace is discontinued. Progressive resistance exercises, closed kinetic chain strengthening, and functional training are emphasized.
Hardware removal is generally not recommended unless the patient develops symptomatic hardware prominence (most common with K-wires backing out), which occurs in up to 20-30% of cases. If required, removal should be delayed until at least 6 to 12 months postoperatively to ensure complete osseous union.
Associated Surgical & Radiographic Imaging

📚 Medical References
- patella fractures with fi gure-eight wiring through parallel cannulated compression screws, J Orthop Trauma 11:573, 1997.
- Bickel WH, Johnson KA: Z-plasty patellectomy, Surg Gynecol Obstet 132:985, 1971.
- Böstman O, Kiviluoto O, Nirhamo J: Comminuted displaced fractures of the patella, Injury 13:196, 1981.
- Boström A: Fracture of the patella: a study of 422 patellar fractures, Acta Orthop Scand Suppl 143:1, 1972.
- Brooke R: The treatment of fractured patella by excision: a study of morphology and function, Br J Surg 24:733, 1936-1937.
- Burton VW, Thomas HM: Results of excision of the patella, Surg Gynecol Obstet 135:753, 1972.
- Burvant JG, Thomas KA, Alexander R, et al: Evaluation of methods of internal fi xation of transverse patella fractures: a biomechanical study, J Orthop Trauma 8:147, 1994.
- Carpenter JE, Kasman R, Matthews LS: Fractures of the patella, J Bone Joint Surg 75A:1550, 1993.
- Catalano JB, Iannacone WM, Marczyk S, et al: Open fractures of the patella: long-term functional outcome, J Trauma 39:439, 1995.
- Chang MA, Rand JA, Trousdale RT: Patellectomy after
You Might Also Like
