Mastering Surgical Approaches to the Spine: Anterior, Posterior, and Combined Techniques
Key Takeaway
Selecting the optimal surgical approach to the spine requires a profound understanding of regional anatomy, biomechanics, and pathology. This comprehensive guide details anterior, lateral, and posterior spinal approaches, including transoral, retropharyngeal, and extended maxillotomy techniques. Designed for orthopedic surgeons and neurosurgeons, it provides step-by-step operative instructions, relative indications, and critical neurovascular safeguards to optimize patient outcomes and minimize perioperative complications in complex spinal reconstructions.
SURGICAL APPROACHES TO THE SPINE: AN EVOLUTION OF TECHNIQUE
Historically, the posterior approach for the correction of spinal deformities and decompression was the undisputed gold standard. However, as spinal biomechanics became better understood, profound attention shifted toward the anterior approach to the spinal column. Many pioneers in the field of anterior spinal surgery recognized that anterior spinal cord decompression was absolutely necessary in conditions such as spinal tuberculosis (Pott's disease). They observed that a posterior laminectomy not only failed to relieve anterior compressive pathology but also removed critical posterior tension-band structures, leading to catastrophic iatrogenic destabilization and progressive kyphosis.
Today, the selection of a surgical approach is dictated by the location of the pathology, the need for biomechanical stabilization, and the patient's physiological tolerance for specific exposures.
💡 Clinical Pearl: The Biomechanical Imperative
The anterior column of the spine supports approximately 80% of axial compressive loads, while the posterior column resists tensile forces. When pathology (tumor, infection, trauma) destroys the anterior column, an anterior approach allows for direct decompression and the placement of load-sharing structural grafts or cages, which are biomechanically superior to posterior-only constructs in these scenarios.
Relative Indications for Anterior Spinal Approaches
The decision to utilize an anterior approach is guided by specific clinical scenarios where posterior access is either inadequate or contraindicated.
1. Traumatic Lesions
* Fractures with documented neurocompression secondary to retropulsed bone or disc fragments anterior to the dura.
* Incomplete spinal cord injury (for cord recovery) with anterior extradural compression.
* Complete spinal cord injury (for root recovery) with anterior extradural compression.
* Late-onset pain or progressive paralysis after remote injuries with anterior extradural compression.
* Traumatic herniated intervertebral disc.
2. Infectious Pathologies
* Open biopsy for definitive microbiological diagnosis.
* Radical débridement of osteomyelitis/discitis and anterior strut grafting.
3. Degenerative Conditions
* Cervical spondylotic radiculopathy (hard or soft disc herniations).
* Cervical spondylotic myelopathy (OPLL, multilevel spondylosis).
* Thoracic disc herniation (where posterior laminectomy carries a high risk of cord injury).
* Cervical, thoracic, and lumbar interbody fusions.
4. Neoplastic Disease
* Extradural metastatic disease causing anterior cord compression.
* Primary vertebral body tumors requiring en bloc resection (e.g., chordoma, giant cell tumor).
5. Spinal Deformity
* Kyphosis—congenital or acquired (requiring anterior release).
* Scoliosis—congenital, acquired, or idiopathic (for anterior release and fusion).
UPPER CERVICAL SPINE: ANTERIOR APPROACHES
The upper cervical spine (Occiput to C2) presents unique anatomical challenges due to the presence of the mandible, pharynx, and critical neurovascular structures (carotid arteries, vertebral arteries, lower cranial nerves).
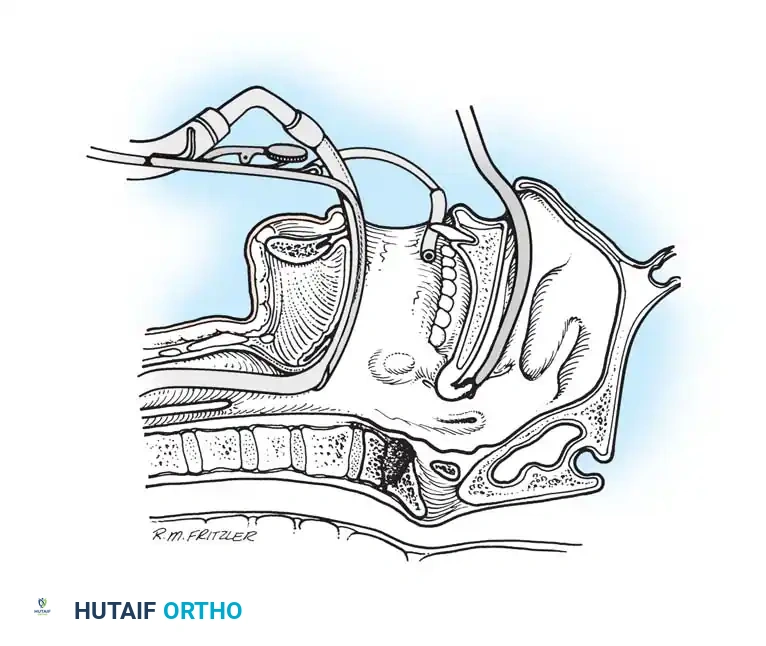
Anterior Transoral Approach (Spetzler Technique)
The transoral approach provides direct, midline access to the anterior ring of C1, the odontoid process, and the body of C2. It is the approach of choice for extradural midline pathology, such as rheumatoid pannus, basilar invagination, or midline tumors.
Step-by-Step Surgical Technique:
* Positioning: Position the patient supine using a Mayfield head-holding device or with skeletal traction through Gardner-Wells tongs. The neck is slightly extended. Continuous monitoring of the spinal cord through somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs) is mandatory. The surgeon typically sits directly over the patient’s head.
* Preparation: Pass a red rubber catheter down each nostril, retrieving them from the oropharynx, and suture them to the uvula. Apply gentle traction to the catheters to pull the uvula and soft palate superiorly and out of the operative field. Warning: Take extreme care not to cause necrosis of the septal cartilage by applying excessive pressure.
* Exposure: Insert a McGarver (or Crockard) transoral retractor into the open mouth. Use it to retract the tongue inferiorly and hold the endotracheal tube out of the way. The operating microscope is highly recommended to improve illumination and magnification in this deep, limited exposure.
* Asepsis: Prepare the oropharynx meticulously with hexachlorophene (pHisoHex) and povidone-iodine (Betadine) solutions.
* Incision: Palpate the anterior tubercle of C1 beneath the posterior pharyngeal wall. Make a midline longitudinal incision in the wall of the posterior pharynx from the superior aspect of C1 to the top of C3.
* Dissection: Obtain hemostasis with bipolar electrocautery. Pitfall: Do not overcauterize, as thermal necrosis of the pharyngeal mucosa significantly increases the risk of postoperative wound dehiscence and catastrophic infection.
* Bony Exposure: With a periosteal elevator, subperiosteally dissect the edges of the pharyngeal incision laterally from the anterior ring of C1 and the anterior aspect of C2. Use heavy traction stitches to maintain the mucosal flaps laterally.
* Decompression: Under direct microscopic vision, perform a meticulous débridement of C1 and C2 using a high-speed air drill, rongeurs, and curettes. When approaching the posterior longitudinal ligament and the dura, switch to a diamond burr to safely remove the last remnants of cortical bone.
* Reconstruction: If the cervical spine requires anterior fusion, harvest a corticocancellous graft from the patient’s iliac crest, fashion it to fit the defect, and impact it securely.
* Closure: Irrigate the operative site copiously with antibiotic solution. Close the posterior pharynx in multiple interrupted layers using absorbable sutures.
Postoperative Protocol:
An endotracheal tube is left in place overnight to maintain an adequate airway, as pharyngeal edema can be severe. A halo-vest is typically applied, or skeletal traction may be maintained before mobilization, especially if posterior stabilization is planned as a second stage.
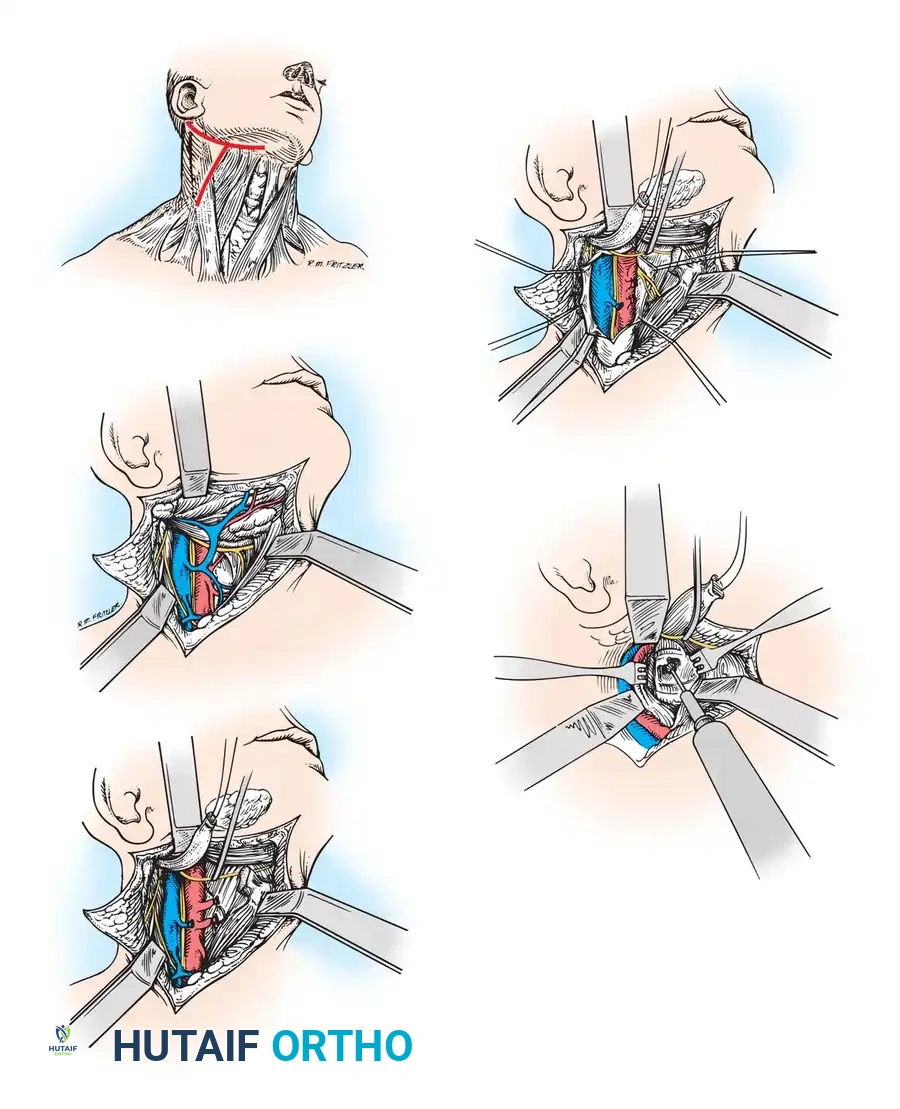
Anterior Retropharyngeal Approach (McAfee Technique)
The anterior retropharyngeal approach to the upper cervical spine is an excellent alternative for anterior débridement and stabilization. In contrast to the transoral approach, it is entirely extramucosal, significantly reducing the risk of polymicrobial wound infection and allowing for the safe placement of instrumentation.
Step-by-Step Surgical Technique:
* Positioning: Position the patient supine, preferably on a turning frame with skeletal traction through tongs or a halo ring. SSEP and MEP monitoring is required.
* Intubation: Perform fiberoptic nasotracheal intubation to prevent excessive motion of the unstable neck and to keep the oropharynx free of tubes that could depress the mandible and interfere with the superior trajectory of the exposure.
* Incision: Make a right-sided transverse skin incision in the submandibular region, approximately 2 cm below the mandible. A vertical extension along the anterior border of the sternocleidomastoid (SCM) can be added if lower cervical exposure is required.
* Superficial Dissection: Carry the dissection through the platysma muscle. Mobilize subplatysmal flaps.
* Nerve Protection: Identify the marginal mandibular branch of the facial nerve (CN VII) using a nerve stimulator. Surgical Pearl: Keep the dissection deep to the retromandibular vein and the fascia of the submandibular gland to prevent injury to this nerve.
* Vascular Control: Ligate the retromandibular vein as it joins the internal jugular vein. Ligate the facial artery and vein to allow superior mobilization of the submandibular gland.
* Deep Dissection: Mobilize the anterior border of the SCM by dividing the superficial layer of the deep cervical fascia. Palpate the carotid artery and protect the carotid sheath contents laterally.
* Gland Resection: Resect the submandibular gland if necessary for exposure, ensuring the submandibular duct (Wharton's duct) is securely ligated to prevent a salivary fistula.
* Muscular Division: Identify the digastric and stylohyoid muscles. Tag and divide the intermediate tendon of the digastric muscle. Warning: The facial nerve can be injured by aggressive superior retraction on the stylohyoid muscle. Dividing these muscles allows the hyoid bone and hypopharynx to be mobilized medially.
* Nerve Identification: Identify the hypoglossal nerve (CN XII) as it crosses the external carotid artery, and retract it superiorly. Identify and mobilize the superior laryngeal nerve.
* Retropharyngeal Space: Continue dissection into the retropharyngeal space between the carotid sheath laterally and the larynx/pharynx medially. Ligate branches of the carotid artery (superior thyroid, lingual, facial) and internal jugular vein that tether the sheath.
* Prevertebral Fascia: Following adequate lateral retraction of the carotid sheath, divide the alar and prevertebral fascial layers longitudinally to expose the longus colli muscles.
* Bony Work: Remove the longus colli muscles subperiosteally from the anterior arch of C1 and the body of C2. Critical Hazard: Stay strictly midline to avoid injury to the vertebral arteries, which are located laterally in the transverse foramina. Meticulously débride the involved osseous structures and perform bone grafting as indicated.
* Closure: Close the wound over closed-suction drains. Repair the digastric tendon. Close the platysma and skin flaps in layers.
Postoperative Protocol:
The patient is maintained in skeletal traction with the head of the bed elevated to reduce venous congestion and airway swelling. Intubation is continued until pharyngeal edema resolves (usually 48–72 hours).
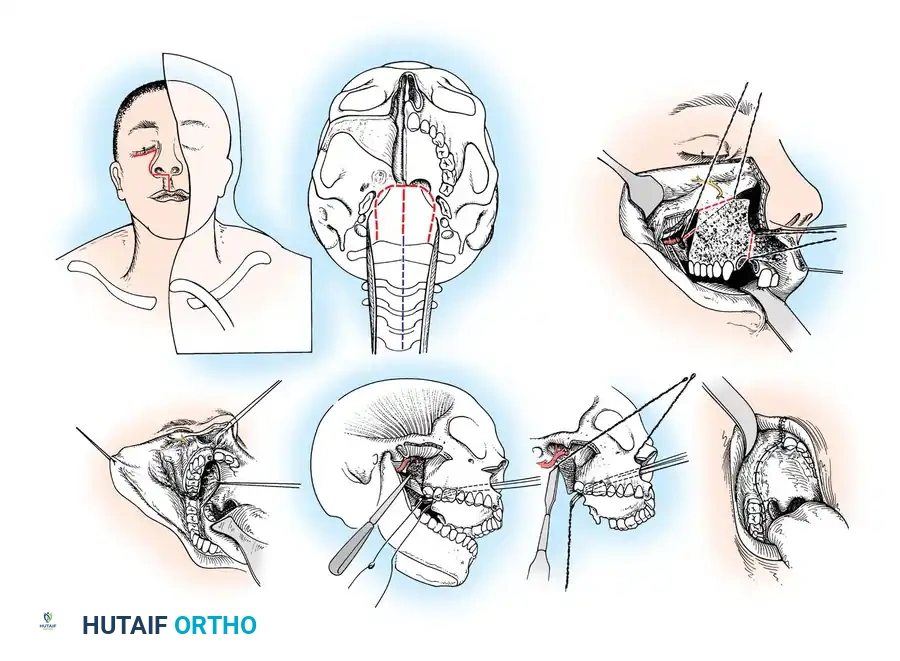
Extended Maxillotomy and Subtotal Maxillectomy (Cocke Technique)
For massive tumors extending from the clivus down to C5, an extended maxillotomy provides unparalleled anterior access. This highly complex, multidisciplinary approach requires an otolaryngologist, a neurosurgeon, and an orthopedic spine surgeon.
Step-by-Step Surgical Technique:
* Preparation: Position the patient with the head elevated 25 degrees. Perform a tracheostomy to secure the airway and a percutaneous endoscopic gastrostomy (PEG) for postoperative nutrition.
* Incision: Expose the superior maxilla through a modified Weber-Ferguson skin incision. Make a vertical incision through the upper lip in the philtrum, extending transversely along the nasolabial groove to the lower eyelid.
* Osteotomies: Elevate the mucoperiosteum of the maxilla. Extract the central incisor tooth. Use a Gigli saw to perform precise osteotomies of the maxilla, malar bone, and ascending process of the maxilla.
* Exposure: Retract the hard palate, soft palate, and pharynx medially. Remove the coronoid process of the mandible to expose the lateral pterygoid plate. Ligate the internal maxillary artery. This massive exposure allows for en bloc resection of chordomas or extensive skull base osteomyelitis.
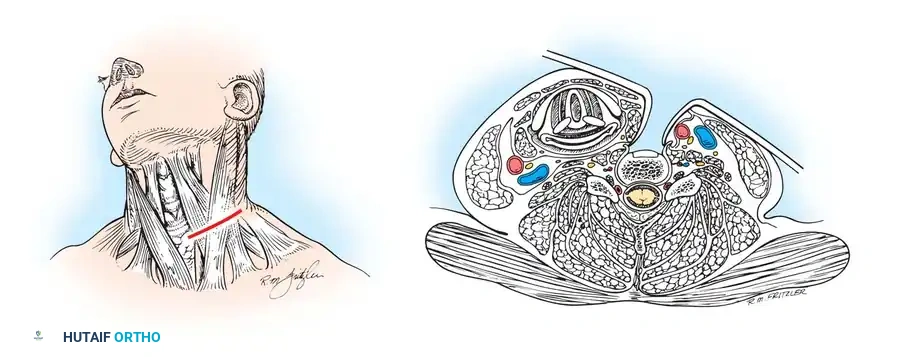
SUBAXIAL CERVICAL SPINE: ANTERIOR APPROACHES
The standard anterior cervical approach (Smith-Robinson) is the workhorse of cervical spine surgery, utilized for Anterior Cervical Discectomy and Fusion (ACDF) and corpectomies.
Superficial Landmarks and Incision:
The approach is typically performed from the left side to decrease the risk of injury to the recurrent laryngeal nerve, which has a more constant and protected course on the left (looping under the aortic arch) compared to the right (looping under the subclavian artery). A transverse incision is made in a natural skin crease corresponding to the target level (e.g., cricoid cartilage for C6).
Superficial Dissection:
The subcutaneous tissue is divided, exposing the platysma muscle. The platysma is divided in line with the skin incision. Subplatysmal flaps are elevated superiorly and inferiorly to allow for mobile retraction. The superficial layer of the deep cervical fascia is incised along the anterior border of the sternocleidomastoid muscle.
Deep Dissection:
The dissection proceeds bluntly between the carotid sheath (containing the carotid artery, internal jugular vein, and vagus nerve) laterally, and the visceral axis (trachea, esophagus, and recurrent laryngeal nerve) medially. The omohyoid muscle may be retracted or divided if accessing the mid-cervical spine (C4-C6).
Prevertebral Exposure:
The prevertebral fascia is identified and incised longitudinally. The longus colli muscles are elevated subperiosteally using a Cobb elevator and retracted laterally beneath the lips of a self-retaining retractor. This exposes the anterior longitudinal ligament, the intervertebral discs, and the vertebral bodies. Surgical Pearl: Always confirm the midline by identifying the medial borders of the longus colli muscles to avoid eccentric dissection and potential injury to the vertebral artery.
THORACIC AND THORACOLUMBAR APPROACHES
Accessing the anterior thoracic and lumbar spine requires navigating the thoracic cavity, the diaphragm, and the retroperitoneal space.
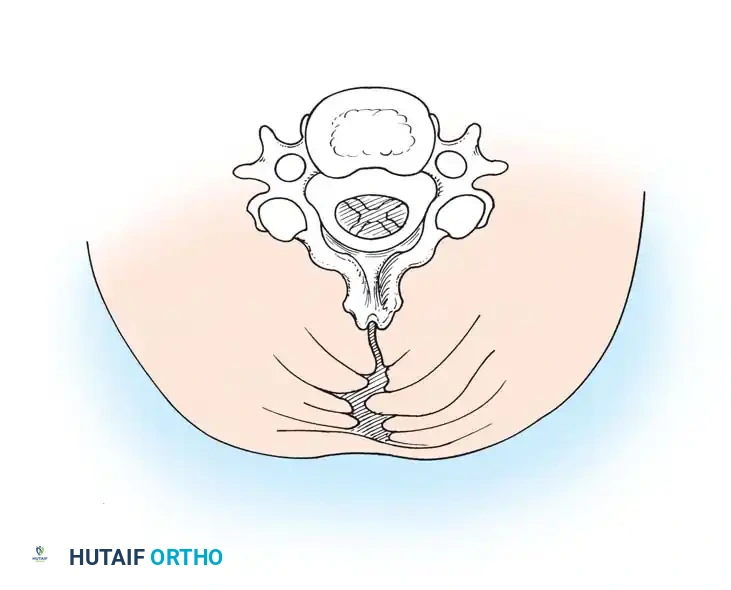
Costotransversectomy and Lateral Extracavitary Approach
When anterior pathology exists but a formal thoracotomy is contraindicated (e.g., severe pulmonary disease), a posterolateral approach can provide access to the anterior column.
Technique:
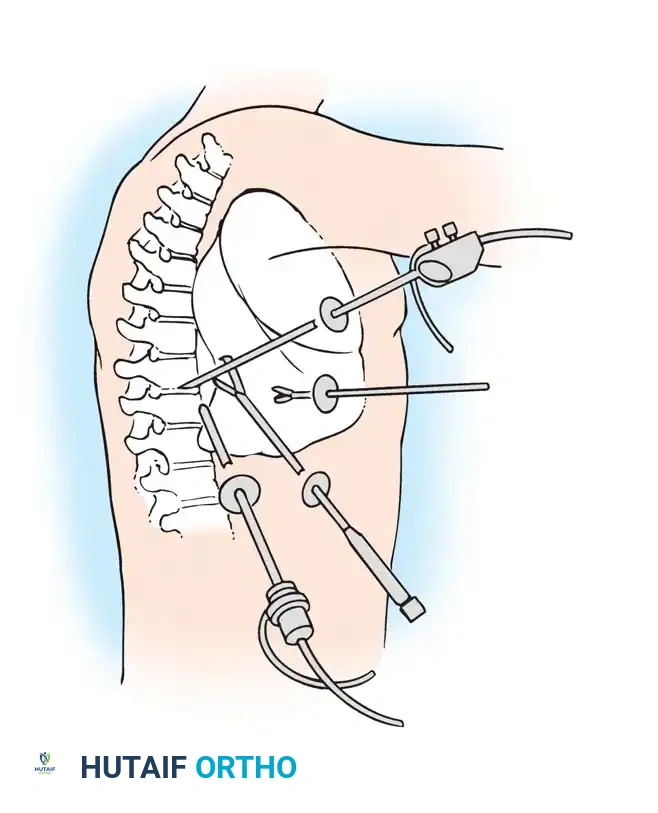
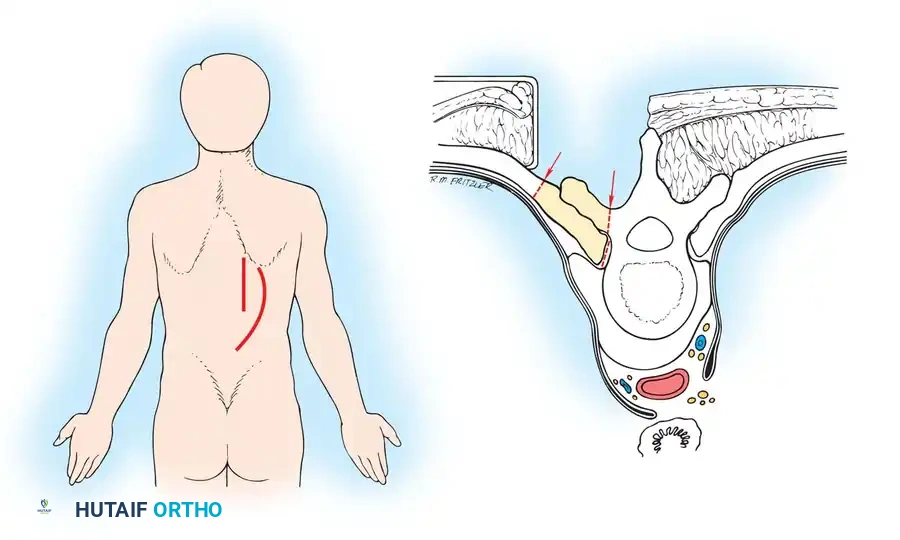
A midline or paramedian curving incision is made. The paraspinal muscles are mobilized medially. The ribs corresponding to the level of pathology are identified. The transverse process and the proximal 3 to 5 cm of the rib are resected. The intercostal nerve is identified and traced to the neuroforamen. By staying extrapleural, the surgeon can follow the lateral aspect of the vertebral body to perform a corpectomy and place an anterior strut graft, all from a posterior-based incision.
Thoracoabdominal Approach
For extensive pathology spanning the thoracolumbar junction (T11-L2), the thoracoabdominal approach provides unparalleled, simultaneous access to the lower thoracic and upper lumbar spine.
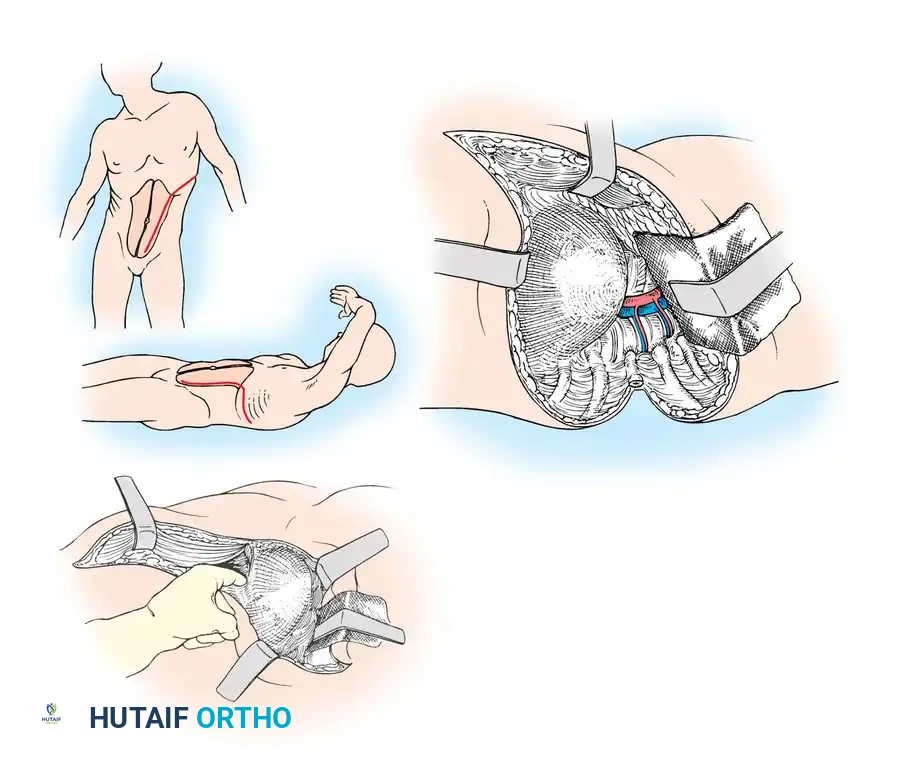
Technique:
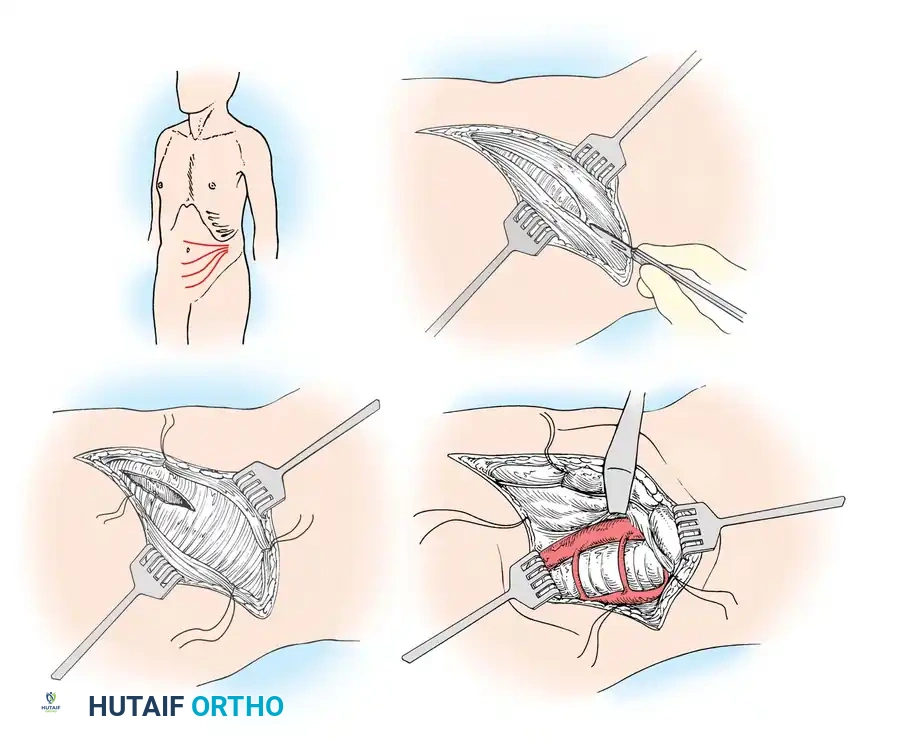
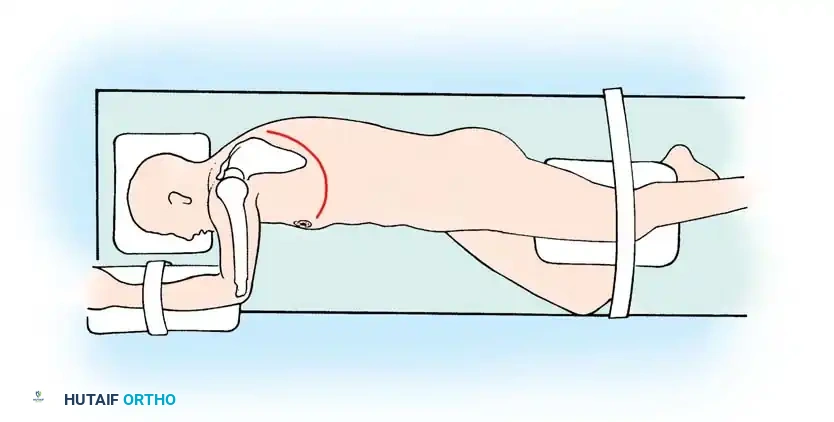
The patient is positioned in the lateral decubitus position. An incision is made over the 10th or 11th rib, extending obliquely across the costal margin toward the lateral border of the rectus abdominis. The rib is resected subperiosteally. The thoracic cavity is entered through the rib bed. The retroperitoneal space is accessed by bluntly sweeping the peritoneum medially. The diaphragm is circumferentially detached near its peripheral insertion (leaving a 2 cm cuff for repair) to unite the thoracic and retroperitoneal cavities. The aorta (if approached from the left) or vena cava (if right) is carefully mobilized to expose the anterior spine.
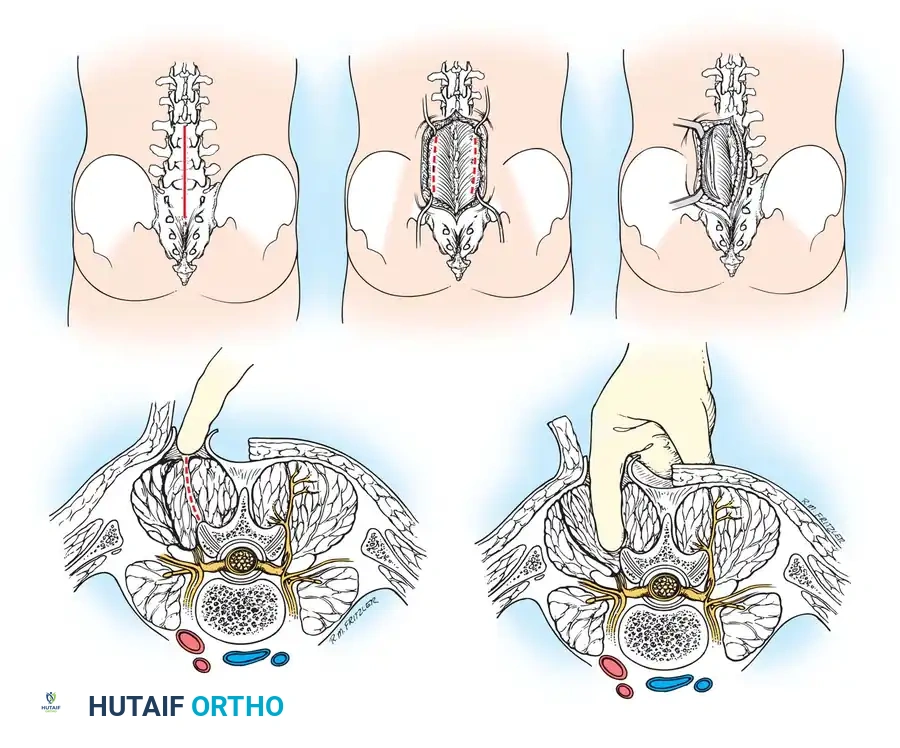
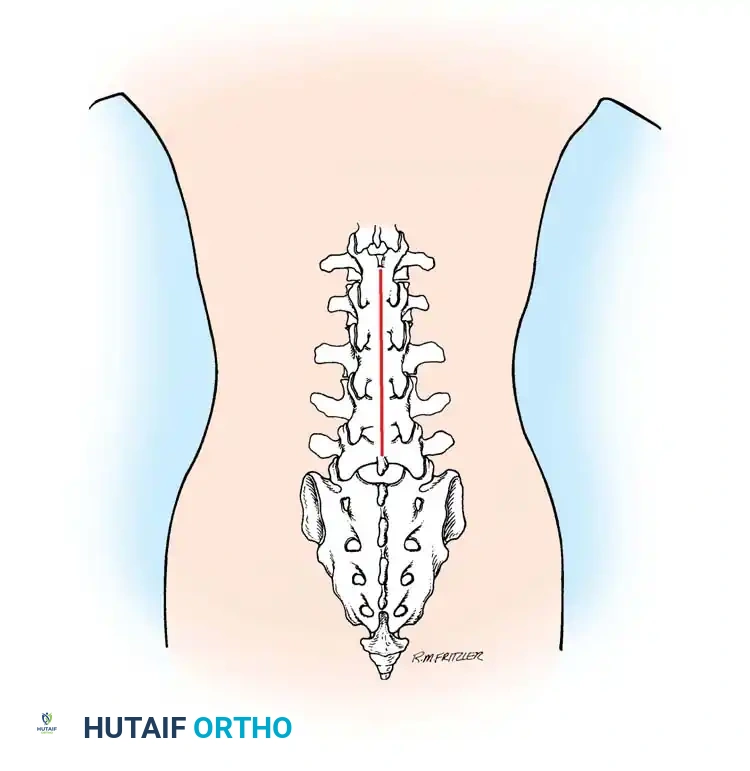
POSTERIOR SURGICAL APPROACHES
While anterior approaches are vital for load-sharing and direct decompression of anterior pathology, posterior approaches remain the foundation of spinal surgery for posterior element decompression (laminectomy), deformity correction (pedicle screw fixation), and posterior column stabilization.
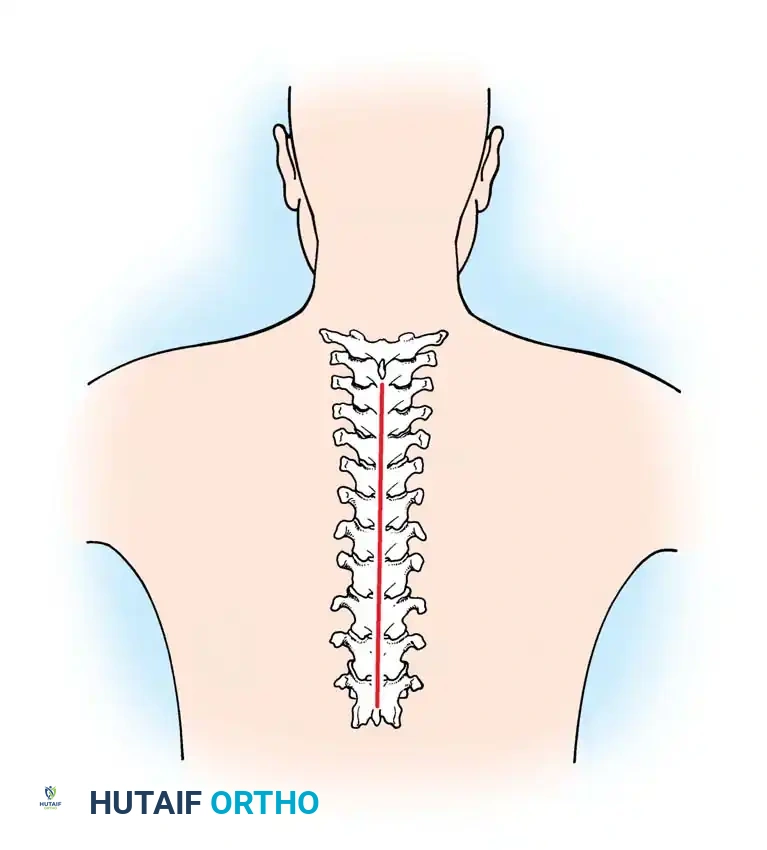
Posterior Cervical Approach
The posterior cervical approach is utilized for laminectomy, laminoplasty, and lateral mass or pedicle screw fixation.
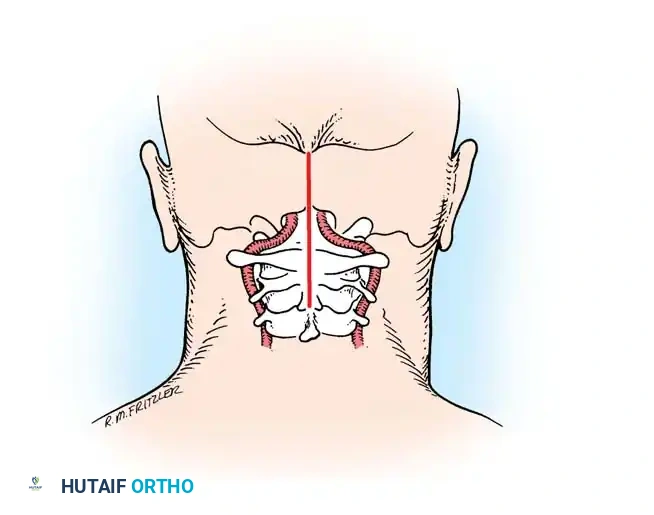
Incision and Superficial Dissection:
The patient is positioned prone with the head secured in a Mayfield pin fixator. A strict midline incision is made from the external occipital protuberance down to the spinous process of C7 or T1.
Midline Avascular Plane:
The dissection must remain strictly in the midline avascular plane, bisecting the ligamentum nuchae. Straying laterally into the paraspinal musculature leads to excessive bleeding and denervation of the muscles.
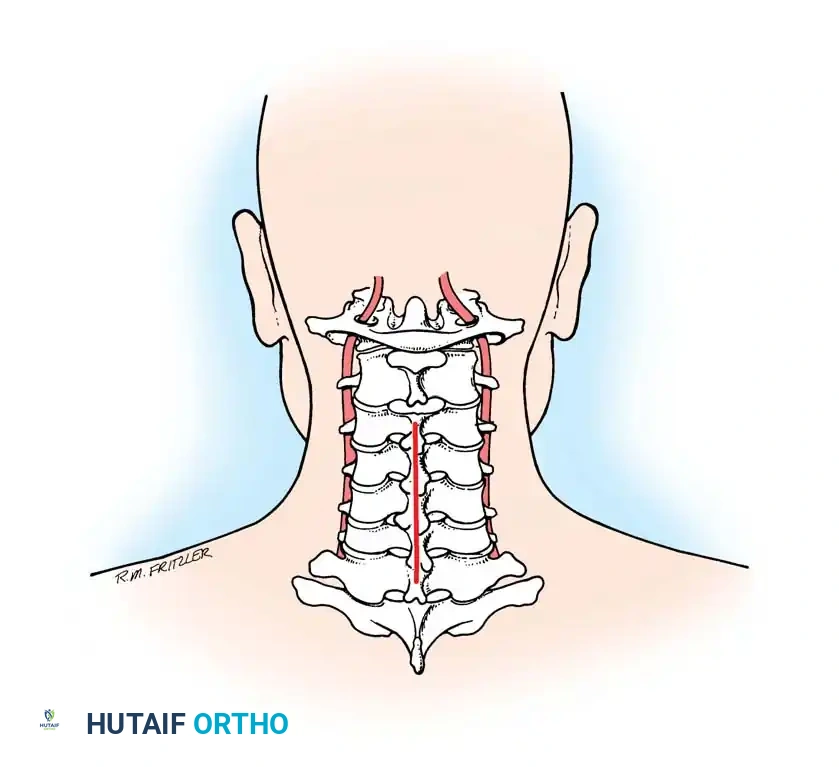
Deep Muscle Dissection:
Once the spinous processes are reached, the paraspinal muscles (splenius capitis, semispinalis cervicis) are stripped subperiosteally using electrocautery and Cobb elevators.
Associated Surgical & Radiographic Imaging
You Might Also Like


