Modified Woodward Repair: Fixing High Elevation of the Scapula
Key Takeaway
Your ultimate guide to Modified Woodward Repair: Fixing High Elevation of the Scapula starts here. Sprengel deformity is a congenital shoulder anomaly characterized by the high elevation of the scapula, which is often hypoplastic and medially rotated. This condition results from interrupted normal caudal migration of the scapula during fetal development. It is present at birth and may involve an omovertebral bone connecting the scapula to cervical vertebrae.
Introduction and Epidemiology
Sprengel deformity represents a complex congenital anomaly of the shoulder girdle characterized by the high elevation of a hypoplastic scapula, accompanied by medial rotation of its inferior pole. First described in the literature by Eulenberg in 1863 as a congenital "high dislocation of the scapula," the condition is the most common congenital defect of the shoulder, though it remains a rare entity overall. In 1880, Willet and Walsham contributed to the foundational understanding of the deformity by describing the omovertebral bone, a broad osseous, cartilaginous, or fibrous band connecting the superomedial angle of the scapula to the lower cervical spine.
Epidemiologically, Sprengel deformity occurs sporadically, though familial occurrences with autosomal dominant inheritance patterns have been documented. The deformity exhibits a distinct predilection for female patients, with a female-to-male ratio frequently reported as 3 to 1. Unilateral presentation is most common, with the left shoulder involved more frequently than the right. Bilateral involvement occurs in approximately 10 to 30 percent of cases, presenting a unique clinical challenge characterized by a shortened, webbed neck appearance and severe restriction of bilateral upper extremity elevation.

The exact etiology of Sprengel deformity remains definitively unknown, but pathogenesis is universally attributed to the arrest of the normal caudal migration of the scapula during fetal development. Several theories have been proposed to explain this embryological failure. One prominent theory suggests that cerebrospinal fluid escapes through a bleb in the membrane of the roof of the fourth ventricle into the adjacent tissue of the neck, causing a localized inflammatory response and subsequent malformation. Other proposed mechanisms include increased intrauterine pressure, heredity factors, and primary defective musculature formation that prevents normal mechanical descent.
Because the insult occurs early in embryogenesis, Sprengel deformity is highly associated with other congenital anomalies. Concomitant conditions include Klippel-Feil syndrome (present in up to 30 percent of cases), congenital scoliosis, cervical spina bifida, diastematomyelia, rib deformities (fused or missing ribs), clavicular hypoplasia, and extraskeletal anomalies such as tracheoesophageal fistulas, anal stenosis, and renal malformations. The natural history of the deformity dictates that the abnormal scapula will grow proportionally with the child; however, the relative position of the scapula to the thorax remains constant, and associated spinal anomalies may progress, further exacerbating the clinical deformity.
Surgical Anatomy and Biomechanics
A profound understanding of the embryological and pathoanatomical features of the shoulder girdle is prerequisite for surgical intervention. In normal fetal development, the scapula forms as a cervical appendage adjacent to the C5 vertebral level during the fifth week of gestation. By the end of the third month, differential growth of the axial skeleton and active caudal migration result in the scapula descending to its final position overlying the dorsal thorax between the T2 and T8 vertebrae.
In Sprengel deformity, the scapula is not only abnormally elevated but also morphologically dysplastic. The bone exhibits a decreased vertical diameter, rendering it wider than it is tall. The supraspinous portion of the scapula is frequently elongated, hooked, and rotated anteriorly, creating a convexity that conforms to the apical contour of the dorsal thorax. The entire scapula is rotated such that the glenoid faces inferiorly and the inferior pole is rotated medially toward the spine.

The omovertebral connection is a hallmark pathoanatomical feature, present in approximately 30 to 50 percent of cases. This anomalous band originates from the superomedial angle of the scapula and inserts into the spinous process, lamina, or transverse process of the lower cervical vertebrae, most commonly C6. The composition of this connection varies along a spectrum from dense fibrous tissue to hyaline cartilage to solid cortical bone. When osseous, it may articulate with the scapula via a pseudoarthrosis or be entirely confluent with the scapular body.

The regional musculature is intrinsically involved in the pathology. The periscapular muscles—specifically the trapezius, levator scapulae, and rhomboid major and minor—are frequently hypoplastic, fibrotic, or entirely absent. The trapezius is the most consistently affected muscle, often demonstrating significant fibrotic replacement of normal muscle bellies. This fibrotic tethering, combined with the abnormal orientation of the glenoid and the mechanical block of the omovertebral bone, severely restricts scapulothoracic articulation. Biomechanically, normal shoulder abduction requires a 2 to 1 ratio of glenohumeral to scapulothoracic motion. In Sprengel deformity, the loss of scapulothoracic rotation mechanically limits total shoulder abduction and forward elevation, often restricting motion to less than 90 degrees.
Neuromuscular anatomy demands meticulous attention during surgical correction. The spinal accessory nerve (Cranial Nerve XI) courses deep to the trapezius, supplying motor innervation. The dorsal scapular nerve (C5 root) and the accompanying dorsal scapular artery course deep to the rhomboids and levator scapulae near the medial border of the scapula. The suprascapular nerve courses through the suprascapular notch; in a dysplastic scapula, the morphology of this notch is often altered, placing the nerve at higher risk of traction injury during inferior relocation of the scapula.
Indications and Contraindications
Clinical decision-making regarding surgical intervention is heavily guided by the Cavendish Classification, which categorizes the deformity based on cosmetic appearance and the degree of elevation.
- Grade 1: Very mild deformity; shoulders are level, and the deformity is invisible when dressed.
- Grade 2: Mild deformity; shoulders are level or nearly level, but the superomedial angle of the scapula is visible as a lump when dressed.
- Grade 3: Moderate deformity; visible asymmetry with shoulder elevation of 2 to 5 cm.
- Grade 4: Severe deformity; shoulder elevation greater than 5 cm, with the superior angle of the scapula near the occiput, often accompanied by neck webbing.
Surgical intervention is primarily indicated for Cavendish Grade 3 and Grade 4 deformities to improve cosmetic appearance and optimize shoulder kinematics. The ideal age for surgical correction is between 3 and 8 years. Surgery in children younger than 3 years is challenging due to the small size of the anatomical structures and a higher risk of recurrence. Conversely, surgery in patients older than 8 to 10 years carries a significantly increased risk of brachial plexus traction injury, as the neurovascular structures have adapted to the shortened state and are less tolerant of the acute stretch required for inferior scapular relocation.
| Clinical Scenario | Management Strategy | Rationale and Considerations |
|---|---|---|
| Cavendish Grade 1 or 2 | Non-Operative | Mild cosmetic deformity; function is typically preserved. Physical therapy to maximize ROM. |
| Cavendish Grade 3 or 4 (Age 3 to 8) | Operative (Modified Woodward) | Ideal surgical candidates. High potential for functional improvement and cosmetic correction. |
| Cavendish Grade 3 or 4 (Age > 8-10) | Operative with Caution (Clavicle Osteotomy) | High risk of brachial plexus stretch. Concurrent clavicle osteotomy is often mandatory to decompress the thoracic outlet. |
| Severe Bilateral Deformity | Staged Operative | Bilateral simultaneous correction increases morbidity and surgical time. Staged procedures are preferred. |
| Severe Untreated Cervical Spine Anomalies | Relative Contraindication | Klippel-Feil or severe cervical scoliosis must be evaluated; aggressive scapular pull-down against a rigid, deformed spine may cause neurological compromise. |
Pre Operative Planning and Patient Positioning
Comprehensive preoperative evaluation begins with a meticulous physical examination. The surgeon must document the degree of shoulder asymmetry, the presence of neck webbing, torticollis, and any palpable omovertebral mass. Bilateral active and passive range of motion, specifically forward elevation and abduction, must be precisely measured. A thorough neurological examination of the upper extremities is mandatory to establish a baseline, given the risk of postoperative brachial plexus palsy.
Standard radiographic evaluation includes anteroposterior and lateral views of the cervical spine, thoracic spine, and bilateral shoulders. These plain films assess the degree of scapular elevation, the presence of an omovertebral bone, and concomitant spinal anomalies such as congenital scoliosis or Klippel-Feil syndrome.

Advanced imaging is highly recommended. A three-dimensional computed tomography (3D CT) scan of the shoulder girdle provides invaluable topographical anatomy of the dysplastic scapula and clearly delineates the origin and insertion of the omovertebral connection. Because of the high incidence of intraspinal anomalies (e.g., diastematomyelia, tethered cord, syringomyelia), magnetic resonance imaging (MRI) of the total spine is routinely indicated. In infants younger than 4 months, ultrasonography of the spinal cord may be utilized as a screening tool, though definitive surgical planning usually requires MRI.
Patient positioning is critical for the success of the Modified Woodward procedure. The patient is placed in the prone position on a radiolucent Jackson table or chest rolls. The head must be securely supported using a Mayfield tong system or a specialized horseshoe headrest, ensuring the cervical spine is maintained in a neutral alignment without excessive flexion or extension. The operative arm, and ideally the contralateral arm for comparison, must be draped free. Draping the arm free allows the surgeon to dynamically assess shoulder range of motion during the procedure and, more importantly, permits the evaluation of tension on the brachial plexus during the inferior relocation of the scapula. Intraoperative neuromonitoring, including somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs) of the brachial plexus and upper extremity, is considered the standard of care to immediately identify neurovascular compromise during scapular descent.
Detailed Surgical Approach and Technique
The Modified Woodward procedure is the workhorse surgical technique for Sprengel deformity. Unlike the Green procedure, which involves detaching the muscles from the scapula itself, the Woodward technique detaches the origins of the trapezius and rhomboids from the spinous processes, allowing the entire muscle-scapula complex to be mobilized and advanced inferiorly.
Incision and Superficial Dissection
A longitudinal midline incision is made over the spinous processes, extending from the upper cervical spine (approximately C4) down to the lower thoracic spine (T9 or T10). The subcutaneous tissues are sharply dissected to expose the deep fascia overlying the spinous processes. The deep fascia is incised strictly in the midline to minimize bleeding. Subperiosteal dissection is utilized to elevate the skin and subcutaneous flaps laterally, exposing the origin of the trapezius muscle bilaterally.
Muscle Detachment and Deep Dissection
The lateral border of the lower portion of the trapezius is identified. The surgeon develops the plane deep to the trapezius, carefully separating it from the underlying latissimus dorsi. The fascial origin of the trapezius is sharply detached from the spinous processes. This detachment is carried superiorly to the cervical spine. As the trapezius is reflected laterally, the underlying rhomboid major and minor muscles are exposed.
The rhomboids are similarly detached from their origins on the spinous processes. It is imperative to maintain the integrity of the aponeurotic origins of these muscles, as they will be utilized for the subsequent inferior repair. Deep to the rhomboids, the levator scapulae is identified at its insertion on the superomedial angle of the scapula. The spinal accessory nerve, which courses vertically along the deep surface of the trapezius, and the dorsal scapular nerve and artery, which run parallel to the medial border of the scapula, must be meticulously protected during this mobilization.

Omovertebral Bone Resection and Scapular Modification
Once the musculature is reflected laterally, the superomedial angle of the scapula and the omovertebral connection are directly visualized. If an omovertebral bone or fibrous band is present, it must be excised entirely. The resection should be extra-periosteal; leaving residual periosteum can lead to heterotopic ossification and recurrence of the tether.
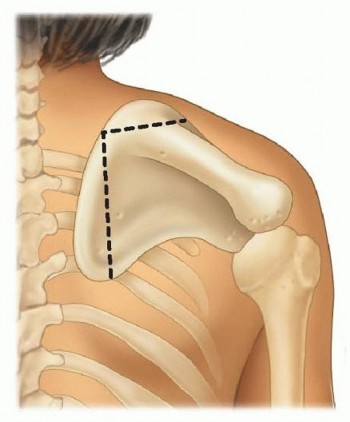
Following the release of the omovertebral tether, the superomedial angle of the scapula is addressed. This portion of the scapula is typically deformed, elongated, and curves anteriorly over the thorax. Retaining this deformed bone will result in a prominent, unsightly mass in the supraclavicular fossa once the scapula is pulled inferiorly. Therefore, an extra-periosteal resection of the superomedial angle is performed. Care must be taken not to extend the resection too far laterally into the suprascapular notch, which would jeopardize the suprascapular nerve.
Clavicular Osteotomy Consideration
In older children (typically >8 years) or in cases of severe deformity, the inferior displacement of the scapula can cause the clavicle to compress the brachial plexus and subclavian vessels against the first rib. To prevent this thoracic outlet-type compression, a concurrent morcellized clavicle osteotomy or partial clavicle resection may be required prior to scapular relocation. This prophylactic step shortens the clavicle and widens the costoclavicular space.
Scapular Relocation and Fixation
With the tethering structures released and the superomedial angle excised, the scapula is mobilized. The surgeon grasps the scapula and translates it inferiorly, simultaneously rotating the inferior pole laterally to orient the glenoid in a more anatomical, forward-facing position. During this maneuver, the neuromonitoring technician must continuously assess SSEP and MEP signals. If signal degradation occurs, the scapula must be allowed to migrate superiorly until signals normalize, dictating the maximum safe limit of correction.

Once the optimal, safe position is achieved, the aponeuroses of the rhomboids and trapezius are sutured back to the spinous processes at a more inferior level. Heavy, non-absorbable sutures are passed through the spinous processes or the robust midline supraspinous ligament. The redundant fold of the trapezius aponeurosis at the inferior aspect of the incision is often excised or imbricated to provide a smooth contour. A closed suction drain is placed deep to the muscle layer, and the wound is closed in meticulous anatomical layers.
Complications and Management
Surgical correction of Sprengel deformity is a major undertaking with a distinct complication profile. The most devastating complication is brachial plexus palsy, which occurs secondary to traction on the nerves during the inferior pull of the scapula or compression of the neurovascular bundle between the clavicle and the first rib. Continuous intraoperative neuromonitoring is the primary defense against this complication.
| Complication | Estimated Incidence | Prevention and Salvage Strategy |
|---|---|---|
| Brachial Plexus Palsy | 2 - 5% | Prevention: Use SSEPs/MEPs. Perform concurrent clavicle osteotomy in older children. Limit inferior pull if signals drop. Salvage: Immediate release of fixation if noted postoperatively. Most are neuropraxias that resolve with time and therapy. |
| Hypertrophic Scarring / Keloid | 10 - 20% | Prevention: Meticulous layered closure, avoidance of excessive tension on the skin, use of sub-cuticular sutures. Salvage: Silicone sheeting, intralesional corticosteroid injections, laser therapy. |
| Scapular Winging | 5 - 10% | Prevention: Secure, robust fixation of the trapezius and rhomboid aponeurosis to the spinous processes. Salvage: Prolonged immobilization. Revision surgery if aponeurotic avulsion occurs. |
| Incomplete Correction / Recurrence | 10 - 15% | Prevention: Complete extra-periosteal excision of the omovertebral bone and superomedial angle. Salvage: Revision surgery is technically demanding and carries higher neurovascular risk; often managed non-operatively if functional. |
| Spinal Accessory Nerve Injury | < 2% | Prevention: Precise identification and protection of the nerve during reflection of the trapezius. Salvage: Nerve exploration and grafting if transected; tendon transfers (e.g., Eden-Lange procedure) for chronic palsy. |
Post Operative Rehabilitation Protocols
Postoperative management is designed to protect the surgical repair while preventing severe stiffness of the shoulder girdle.
Phase 1: Protection and Healing (Weeks 0 to 4)
Immediately postoperatively, the patient is placed in a Velpeau sling or a custom shoulder immobilizer. The primary goal during this phase is to allow the reattached musculature to heal to the midline fascia and spinous processes. Active movement of the elbow, wrist, and hand is encouraged immediately to prevent distal edema and stiffness. Passive pendulum exercises of the shoulder may be initiated at 2 weeks, but active elevation and abduction are strictly prohibited to prevent avulsion of the muscular repair.
Phase 2: Early Motion (Weeks 4 to 8)
At 4 weeks, the sling is discontinued. The patient begins a supervised physical therapy program focusing on active-assisted range of motion. Supine forward elevation using a wand or pulley system is initiated. Scapular mobilization techniques are employed to prevent adhesions between the scapula and the thoracic wall. Pool therapy (aquatic therapy) is highly beneficial during this phase, as buoyancy assists with elevation and reduces the gravitational load on the healing muscles.
Phase 3: Strengthening and Functional Restoration (Weeks 8 to 12+)
By 8 weeks, the muscular attachments are generally secure enough to tolerate active strengthening. Therapy transitions to active range of motion exercises and progressive resistance training. Emphasis is placed on strengthening the periscapular stabilizers, particularly the lower trapezius, rhomboids, and serratus anterior, to optimize the newly established scapulothoracic kinematics. Full return to unrestricted activities and sports is typically permitted between 4 and 6 months postoperatively, contingent upon the recovery of near-normal strength and dynamic scapular control.
Summary of Key Literature and Guidelines
The academic foundation for the surgical management of Sprengel deformity relies on a few seminal papers and modern retrospective reviews.
The original procedure was detailed by Woodward in 1961 (Journal of Bone and Joint Surgery), fundamentally changing the approach from scapular-based muscle detachment (the Green procedure) to spinal-based detachment. Woodward’s technique allowed for a more physiological relocation of the entire muscle-bone unit, reducing the incidence of ischemic muscle necrosis and improving the cosmetic contour of the neck.
Cavendish’s 1972 publication established the clinical grading system that remains the universal standard for preoperative assessment and surgical indication. The Cavendish classification shifted the focus from purely radiographic measurements to the clinical and cosmetic impact of the deformity, which correlates more directly with patient and parent satisfaction.
Modern literature, including extensive reviews by Grogan et al. and Mears et al., has validated the long-term efficacy of the Modified Woodward procedure. Outcome studies consistently demonstrate an average improvement in shoulder abduction of 15 to 30 degrees, alongside significant improvements in the Cavendish cosmetic grade. The addition of the clavicular osteotomy, popularized by Morrill and others, has been well-documented in recent literature as a critical adjunct in older children, significantly reducing the historical rates of brachial plexus palsy associated with aggressive inferior scapular translation. Current orthopedic guidelines strongly advocate for surgical intervention in severe cases between the ages of 3 and 8 years, utilizing the Modified Woodward technique combined with rigorous intraoperative neuromonitoring.
Clinical & Radiographic Imaging
You Might Also Like