Orthopedic Trauma Review | Dr Hutaif Trauma & Fractures -...
14 Apr 2026
66 min read
85 Views

Key Takeaway
Looking for accurate information on Orthopedic MCQS Trauma 0018? Humeral shaft fractures, often sustained from trauma like a motor vehicle collision, are treated surgically with open reduction internal fixation (ORIF) or intramedullary nailing (IMN). A primary difference is IMN's higher incidence of shoulder complications compared to ORIF. No significant differences in nerve injury, union, or infection rates are consistently found between the two procedures.
Orthopedic Trauma Review | Dr Hutaif Trauma &...
00:00
Start Quiz
Question 1High Yield
A 32-year-old man has a closed mid-shaft spiral humeral fracture after a fall. After a discussion of his treatment options, he wants to proceed with surgical management. When counseling him about open reduction internal fixation (ORIF) versus intramedullary nailing (IMN), what is the primary difference in outcomes between the two procedures?
Explanation
There has been an abundance of studies designed to compare ORIF with IMN of humeral shaft fractures. When the most well-designed and rigorous studies are pooled and reviewed, the only consistent difference that can be found is a higher incidence of shoulder complications with IMN compared with ORIF. No significant differences have been shown with regard to nerve injury, union, or infection.
Recommended reading:
1. [Carroll EA, Schweppe M, Langfitt M, Miller AN, Halvorson JJ. Management of humeral shaft fractures. J Am Acad Orthop Surg. 2012 Jul;20(7):423-33. doi: 10.5435/JAAOS-20-07-423. Review. PubMed PMID: ](https://www.ncbi.nlm.nih.gov/pubmed/22751161)22751161.
2. [Zhao JG, Wang J, Wang C, Kan SL. Intramedullary nail versus plate fixation for humeral shaft fractures: a systematic review of overlapping meta-analyses. Medicine (Baltimore). 2015 Mar;94(11):e599. doi: 10.1097/MD.0000000000000599. Review. PubMed PMID: ](https://www.ncbi.nlm.nih.gov/pubmed/25789949)[2578994](https://www.ncbi.nlm.nih.gov/pubmed/25789949)
Recommended reading:
1. [Carroll EA, Schweppe M, Langfitt M, Miller AN, Halvorson JJ. Management of humeral shaft fractures. J Am Acad Orthop Surg. 2012 Jul;20(7):423-33. doi: 10.5435/JAAOS-20-07-423. Review. PubMed PMID: ](https://www.ncbi.nlm.nih.gov/pubmed/22751161)22751161.
2. [Zhao JG, Wang J, Wang C, Kan SL. Intramedullary nail versus plate fixation for humeral shaft fractures: a systematic review of overlapping meta-analyses. Medicine (Baltimore). 2015 Mar;94(11):e599. doi: 10.1097/MD.0000000000000599. Review. PubMed PMID: ](https://www.ncbi.nlm.nih.gov/pubmed/25789949)[2578994](https://www.ncbi.nlm.nih.gov/pubmed/25789949)
Question 2High Yield
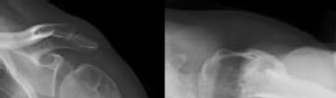
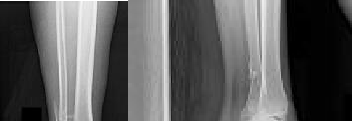
Figure 1 is the radiograph of a 49-year-old man who sustained a closed injury to his
left shoulder in a motor vehicle collision. He underwent uncomplicated ORIF (see Figure 2), but at his first post-operative visit he had persistent pain and deformity (see Figure 3). What is the primary factor contributing to this complication?
---
---
---
left shoulder in a motor vehicle collision. He underwent uncomplicated ORIF (see Figure 2), but at his first post-operative visit he had persistent pain and deformity (see Figure 3). What is the primary factor contributing to this complication?
---
---
---



Explanation
The fixation construct most likely failed due to a lack of inferomedial calcar support. Biomechanical and clinical studies have emphasized the importance of medial calcar support in preventing varus collapse. This can be accomplished in a number of ways, including anatomic reduction of the medial calcar, long locking screws that engage the inferomedial humeral head, or medial cortical reconstruction with a fibular strut.
The working length of the construct is not excessively long, and the plate length is sufficient. Though there remains a gap at the fracture site, the overall reduction is satisfactory and not the primary cause for fixation failure.
The working length of the construct is not excessively long, and the plate length is sufficient. Though there remains a gap at the fracture site, the overall reduction is satisfactory and not the primary cause for fixation failure.
Question 3High Yield
**CLINICAL SITUATION**
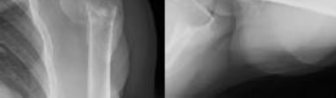
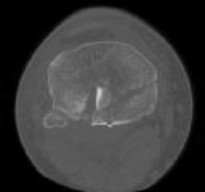
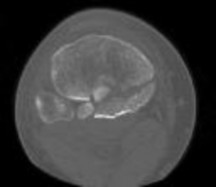
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
A pathognomonic radiographic feature of this injury is a
---
---
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
A pathognomonic radiographic feature of this injury is a
---
---


Explanation
Coronal shear fractures of the distal end of the humerus are rare. Failure to recognize the fracture pattern can lead to poor patient outcomes secondary to poor surgical decision making. The double arc sign is considered a pathognomonic finding on the lateral elbow radiograph seen in Figure 2. This is created by the subchondral bone of the capitellum and lateral trochlear ridge. Excessive internal rotation of the fracture fragment or a subpar lateral radiograph can make recognition of this sign difficulty
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Question 4High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
What is the typical intra-operative patient position for treatment of this injury?
---
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
What is the typical intra-operative patient position for treatment of this injury?
---

Explanation
Coronal shear fractures of the distal end of the humerus are rare. Failure to recognize the fracture pattern can lead to poor patient outcomes secondary to poor surgical decision making. The double arc sign is considered a pathognomonic finding on the lateral elbow radiograph seen in Figure 2. This is created by the subchondral bone of the capitellum and lateral trochlear ridge. Excessive internal rotation of the fracture fragment or a subpar lateral radiograph can make recognition of this sign difficult.
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Question 5High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
The surgical exposure that provides optimal visualization to treat this injury is
---
---
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
The surgical exposure that provides optimal visualization to treat this injury is
---
---


Explanation
Coronal shear fractures of the distal end of the humerus are rare. Failure to recognize the fracture pattern can lead to poor patient outcomes secondary to poor surgical decision making. The double arc sign is considered a pathognomonic finding on the lateral elbow radiograph seen in Figure 2. This is created by the subchondral bone of the capitellum and lateral trochlear ridge. Excessive internal rotation of the fracture fragment or a subpar lateral radiograph can make recognition of this sign difficult. Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular
cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Question 6High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
What type of screws should be available for stabilization of this injury?
---
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
What type of screws should be available for stabilization of this injury?
---

Explanation
Coronal shear fractures of the distal end of the humerus are rare. Failure to recognize the fracture pattern can lead to poor patient outcomes secondary to poor surgical decision making. The double arc sign is considered a pathognomonic finding on the lateral elbow radiograph seen in Figure 2. This is created by the subchondral bone of the capitellum and lateral trochlear ridge. Excessive internal rotation of the fracture fragment or a subpar lateral radiograph can make recognition of this sign difficult.
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral
ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral
ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Question 7High Yield
Figures 1 and 2 are the radiographs of a 46-year-old man with left shoulder pain and
limited range of motion two years after a proximal humerus fracture, which was treated non-operatively. He has forward elevation to 100 degrees with pain at the terminal arc of motion. A subsequent MRI reveals no soft tissue abnormality. After a failed course of non-operative treatment, what is the most appropriate surgical treatment?
---
limited range of motion two years after a proximal humerus fracture, which was treated non-operatively. He has forward elevation to 100 degrees with pain at the terminal arc of motion. A subsequent MRI reveals no soft tissue abnormality. After a failed course of non-operative treatment, what is the most appropriate surgical treatment?
---
Explanation
The patient has a varus malunion of his left proximal humerus. There are no signs of advanced glenohumeral arthrosis or osteonecrosis. After failed nonsurgical treatment, the surgery most likely to improve his symptoms is a valgus-producing osteotomy of the proximal humerus. Arthroscopic tuberoplasty addresses
massive rotator cuff tears or greater tuberosity malunions, but does not address the varus alignment of the articular surface. Humeral hemiarthroplasty can address the deformity but would sacrifice an otherwise normal humeral head in a relatively young patient. Reverse total shoulder arthroplasty would not be indicated in a patient this age with an intact rotator cuff.
massive rotator cuff tears or greater tuberosity malunions, but does not address the varus alignment of the articular surface. Humeral hemiarthroplasty can address the deformity but would sacrifice an otherwise normal humeral head in a relatively young patient. Reverse total shoulder arthroplasty would not be indicated in a patient this age with an intact rotator cuff.
Question 8High Yield
Figures 1 and 2 are the radiographs of a 44-year-old man who comes to the
emergency department after a fall from a ladder with pain and a closed injury to his left shoulder. He undergoes open reduction internal fixation (ORIF) of his left proximal humerus fracture. A postoperative radiograph is shown in Figure
emergency department after a fall from a ladder with pain and a closed injury to his left shoulder. He undergoes open reduction internal fixation (ORIF) of his left proximal humerus fracture. A postoperative radiograph is shown in Figure

Explanation
The patient has a surgical neck fracture with medial calcar comminution. In patients where this cannot be anatomically reconstructed to provide cortical support, a fibular allograft can be used to prevent varus collapse. A “push” screw can be seen in Figure 3, which was used to medialize the graft into a biomechanically favorable position for this fracture pattern. Although the allograft theoretically provides the other benefits listed, they are not the primary indication for this injury.
Question 9High Yield
**CLINICAL SITUATION**
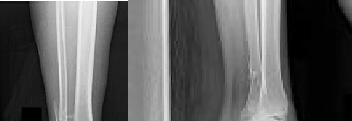
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
What represents the best indication for surgical management of the humeral shaft fracture in this patient?
---
---
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
What represents the best indication for surgical management of the humeral shaft fracture in this patient?
---
---


Explanation
The patient sustained a comminuted extra-articular distal humeral diaphyseal fracture. In isolation, this fracture would still be amenable to an attempt at closed treatment. His radial nerve palsy alone does not warrant open management, as early exploration has not shown a significant benefit in a closed fracture. In addition, despite the comminution and distal extent of the fracture, it is still amenable to closed treatment, though it may be at higher risk for malunion. However, in this patient with multiple lower extremity injuries, fixation of the humerus can facilitate early mobilization and weight-bearing with his right upper extremity, representing a relative indication for surgical management.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
Question 10High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
After a discussion with the patient, surgery is chosen for the right humerus. A posterior triceps-reflecting approach is selected. What structure marks the most proximal extent of the humerus that can be exposed through this approach?
---
---
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
After a discussion with the patient, surgery is chosen for the right humerus. A posterior triceps-reflecting approach is selected. What structure marks the most proximal extent of the humerus that can be exposed through this approach?
---
---


Explanation
The patient sustained a comminuted extra-articular distal humeral diaphyseal fracture. In isolation, this fracture would still be amenable to an attempt at closed treatment. His radial nerve palsy alone does not warrant open management, as early exploration has not shown a significant benefit in a closed fracture. In addition, despite the comminution and distal extent of the fracture, it is still amenable to closed treatment, though it may be at higher risk for malunion. However, in this patient with multiple lower extremity injuries, fixation of the humerus can facilitate
early mobilization and weight-bearing with his right upper extremity, representing a relative indication for surgical management.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
early mobilization and weight-bearing with his right upper extremity, representing a relative indication for surgical management.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
Question 11High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
Postoperative radiographs are shown in Figures 3 and
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
Postoperative radiographs are shown in Figures 3 and




Explanation
The patient sustained a comminuted extra-articular distal humeral diaphyseal fracture. In isolation, this fracture would still be amenable to an attempt at closed treatment. His radial nerve palsy alone does not warrant open management, as early exploration has not shown a significant benefit in a closed fracture. In addition, despite the comminution and distal extent of the fracture, it is still amenable to closed treatment, though it may be at higher risk for malunion. However, in this patient with multiple lower extremity injuries, fixation of the humerus can facilitate early mobilization and weight-bearing with his right upper extremity, representing a relative indication for surgical management.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
Question 12High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
The working length of the plate is best described as the length
---
---
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
The working length of the plate is best described as the length
---
---


Explanation
The patient sustained a comminuted extra-articular distal humeral diaphyseal fracture. In isolation, this fracture would still be amenable to an attempt at closed treatment. His radial nerve palsy alone does not warrant open management, as early exploration has not shown a significant benefit in a closed fracture. In addition, despite the comminution and distal extent of the fracture, it is still amenable to closed treatment, though it may be at higher risk for malunion. However, in this patient with multiple lower extremity injuries, fixation of the humerus can facilitate early mobilization and weight-bearing with his right upper extremity, representing a relative indication for surgical management.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
Question 13High Yield
What is the best treatment option for complex proximal humerus fractures in the
low-demand patient population?
low-demand patient population?


Explanation
In the recent meta-analysis by Mao and associates, there was no evidence to support the use of any of the operative modalities to treat 3- and 4-part fractures of the proximal humerus in low-demand patients. Although surgeons and patients will differ in their treatment algorithms, the recent meta-analysis showed lower complications with nonoperative treatment for these complex fractures. New treatment modalities involving fibular strut allograft, reverse total shoulder arthroplasty for elderly patients with an incompetent rotator cuff, and locked-plate fixation may prove to be superior to nonoperative treatment in select patient populations. However, not one operation has been shown to be superior to nonoperative treatment in the low-demand patient population with complex proximal humerus fractures.
**Question 15of 100**
**CLINICAL SITUATION**
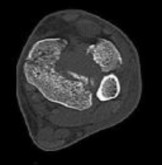
Figure 1 is the radiograph and Figure 2 is the CT image of a 45-year-old woman who fell about 20 feet off her balcony. These images show an isolated, open injury with a 3-cm open medial wound.
The best delayed definitive surgical fixation plan would include
---
1. lateral plating of the fibula and a percutaneous medial column plate.
2. intramedullary fixation of the fibula and an anterolateral tibial plate.
3. open medial column plating, percutaneous screw fixation of the joint, and lateral fibular plating.
4. screw fixation of the medial column with an anterolateral tibial plate and lateral fibular plating
Answer: D
Discussion: The timely administration of antibiotics has been shown to be the best initial treatment to reduce the incidence of infection following an open fracture. Life threatening injuries must first be addressed. But in this isolated open pilon fracture, antibiotics should be initiated early along with tetanus prophylaxis. Reduction and splinting would stabilize the fracture but these interventions should follow antibiotic coverage. Emergency department irrigation is controversial. Closed reduction and splinting, external fixation, CT scan, and delayed open reduction internal fixation would be the preferred sequence of management. External fixation to provide provisional limb stabilization would be indicated in this length unstable C type injury to provide soft tissue stabilization and prevent further chondral injury. Splinting alone would not prevent shortening and would not allow soft tissue recovery. CT scans prior to limb stabilization are not warranted because the patterns make more sense after the restoration of gross length, rotation and alignment in the external fixator. Initial fibular fixation is also not recommended in this case because the location of incisions could affect the definitive surgical tactic. In this multi-fragmentary fibular injury, anatomic reduction would be challenging and malreduction could occur and influence subsequent reconstructions. Delayed open reduction internal fixation is ideal after the resolution of soft tissue swelling.
**Question 15of 100**
**CLINICAL SITUATION**
Figure 1 is the radiograph and Figure 2 is the CT image of a 45-year-old woman who fell about 20 feet off her balcony. These images show an isolated, open injury with a 3-cm open medial wound.
The best delayed definitive surgical fixation plan would include
---
1. lateral plating of the fibula and a percutaneous medial column plate.
2. intramedullary fixation of the fibula and an anterolateral tibial plate.
3. open medial column plating, percutaneous screw fixation of the joint, and lateral fibular plating.
4. screw fixation of the medial column with an anterolateral tibial plate and lateral fibular plating
Answer: D
Discussion: The timely administration of antibiotics has been shown to be the best initial treatment to reduce the incidence of infection following an open fracture. Life threatening injuries must first be addressed. But in this isolated open pilon fracture, antibiotics should be initiated early along with tetanus prophylaxis. Reduction and splinting would stabilize the fracture but these interventions should follow antibiotic coverage. Emergency department irrigation is controversial. Closed reduction and splinting, external fixation, CT scan, and delayed open reduction internal fixation would be the preferred sequence of management. External fixation to provide provisional limb stabilization would be indicated in this length unstable C type injury to provide soft tissue stabilization and prevent further chondral injury. Splinting alone would not prevent shortening and would not allow soft tissue recovery. CT scans prior to limb stabilization are not warranted because the patterns make more sense after the restoration of gross length, rotation and alignment in the external fixator. Initial fibular fixation is also not recommended in this case because the location of incisions could affect the definitive surgical tactic. In this multi-fragmentary fibular injury, anatomic reduction would be challenging and malreduction could occur and influence subsequent reconstructions. Delayed open reduction internal fixation is ideal after the resolution of soft tissue swelling.
Question 14High Yield
**CLINICAL SITUATION**
Figure 1 is the radiograph and Figure 2 is the CT image of a 45-year-old woman who fell about 20 feet off her balcony. These images show an isolated, open injury with a 3-cm open medial wound.
Three years following surgery, which parameter will most likely predict a poor clinical outcome and failure to return to work?
---
---
Figure 1 is the radiograph and Figure 2 is the CT image of a 45-year-old woman who fell about 20 feet off her balcony. These images show an isolated, open injury with a 3-cm open medial wound.
Three years following surgery, which parameter will most likely predict a poor clinical outcome and failure to return to work?
---
---

Explanation
The timely administration of antibiotics has been shown to be the best initial treatment to reduce the incidence of infection following an open fracture. Life threatening injuries must first be addressed. But in this isolated open pilon fracture, antibiotics should be initiated early along with tetanus prophylaxis. Reduction and splinting would stabilize the fracture but these interventions should follow antibiotic coverage. Emergency department irrigation is controversial. Closed reduction and splinting, external fixation, CT scan, and delayed open reduction internal fixation would be the preferred sequence of management. External fixation to provide provisional limb stabilization would be indicated in this length unstable C type injury to provide soft tissue stabilization and prevent further chondral injury. Splinting alone would not prevent shortening and would not allow soft tissue recovery. CT scans prior to limb stabilization are not warranted because the patterns make more sense after the restoration of gross length, rotation and alignment in the external fixator. Initial fibular fixation is also not recommended in this case because the location of incisions could affect the definitive surgical tactic. In this multi-fragmentary fibular injury, anatomic reduction would be challenging and malreduction could occur and influence subsequent reconstructions. Delayed open reduction internal fixation is ideal after the resolution of soft tissue swelling.
Anterolateral buttress plating of the tibial component and lateral plating of the fibula would best resist the valgus compression failure of the lateral column. The medial side failed in tension and plating in this location would not biomechanically resist the valgus displacement. Articular reduction could also be carried out from the anterolateral side with joint reconstruction building back to the posterolateral fragment. Secondary to the central articular impaction, isolated screw fixation would
not provide stability to the metaphyseal comminution. Medial columnar screws could be used to secure the medial tension failure and would limit surface implants in the location of the open wounds.
Failure to attain a high school diploma has been related to poorer outcomes following treatment of high-energy pilon fractures. Quality of reduction does lead to better overall results but still has a drastic impact on functional outcomes. The complexity of the initial fracture also does not lead to differing outcomes at longterm follow up.
Anterolateral buttress plating of the tibial component and lateral plating of the fibula would best resist the valgus compression failure of the lateral column. The medial side failed in tension and plating in this location would not biomechanically resist the valgus displacement. Articular reduction could also be carried out from the anterolateral side with joint reconstruction building back to the posterolateral fragment. Secondary to the central articular impaction, isolated screw fixation would
not provide stability to the metaphyseal comminution. Medial columnar screws could be used to secure the medial tension failure and would limit surface implants in the location of the open wounds.
Failure to attain a high school diploma has been related to poorer outcomes following treatment of high-energy pilon fractures. Quality of reduction does lead to better overall results but still has a drastic impact on functional outcomes. The complexity of the initial fracture also does not lead to differing outcomes at longterm follow up.
Question 15High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
After closed manipulative reduction and splint placement, she is scheduled for operative treatment. The stability of the syndesmosis should be evaluated after
---
---
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
After closed manipulative reduction and splint placement, she is scheduled for operative treatment. The stability of the syndesmosis should be evaluated after
---
---


Explanation
The radiographs reveal a trimalleolar ankle fracture dislocation with an associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
1. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
2. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
3. Maximizes the surface area for ankle joint loading
4. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
1. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
2. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
3. Maximizes the surface area for ankle joint loading
4. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
Question 16High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
How is syndesmotic instability best assessed intra-operatively?
---
---
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
How is syndesmotic instability best assessed intra-operatively?
---
---


Explanation
The radiographs reveal a trimalleolar ankle fracture dislocation with an associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
5. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
6. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
7. Maximizes the surface area for ankle joint loading
8. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
5. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
6. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
7. Maximizes the surface area for ankle joint loading
8. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
Question 17High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
How is syndesmotic reduction best assessed intra-operatively?
---
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
How is syndesmotic reduction best assessed intra-operatively?
---


Explanation
The radiographs reveal a trimalleolar ankle fracture dislocation with an associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior
malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
9. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
10. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
11. Maximizes the surface area for ankle joint loading
12. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
9. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
10. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
11. Maximizes the surface area for ankle joint loading
12. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
Question 18High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
Our understanding of malreduction of the syndesmosis has changed over the years based on changes in technique and imaging. Our current understanding is that malreduction of the syndesmosis
---
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
Our understanding of malreduction of the syndesmosis has changed over the years based on changes in technique and imaging. Our current understanding is that malreduction of the syndesmosis
---

Explanation
The radiographs reveal a trimalleolar ankle fracture dislocation with an associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
13. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
14. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
15. Maximizes the surface area for ankle joint loading
16. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
13. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
14. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
15. Maximizes the surface area for ankle joint loading
16. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
Question 19High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
Anatomic reduction and stabilization of the posterior malleolus fracture component
---
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
Anatomic reduction and stabilization of the posterior malleolus fracture component
---

Explanation
The radiographs reveal a trimalleolar ankle fracture dislocation with an
associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior
malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
17. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
18. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
19. Maximizes the surface area for ankle joint loading
20. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior
malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
17. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
18. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
19. Maximizes the surface area for ankle joint loading
20. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
Question 20High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
What is the morphology of the posterior malleolar fracture component?
---
---
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
What is the morphology of the posterior malleolar fracture component?
---
---


Explanation
The radiographs reveal a trimalleolar ankle fracture dislocation with an
associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
21. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
22. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
23. Maximizes the surface area for ankle joint loading
24. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
21. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
22. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
23. Maximizes the surface area for ankle joint loading
24. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
Question 21High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
This knee injury is best described as a
---
---
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
This knee injury is best described as a
---
---


Explanation
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Question 22High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Initial surgical management should consist of
---
---
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Initial surgical management should consist of
---
---


Explanation
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but
typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but
typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Question 23High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Figures 3 through 8 are the axial and sagittal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
---
---
---
---
---
---
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Figures 3 through 8 are the axial and sagittal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
---
---
---
---
---
---








Explanation
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the
femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Question 24High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
The surgical approach for definitive reduction and stabilization of this pattern is
---
---
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
The surgical approach for definitive reduction and stabilization of this pattern is
---
---


Explanation
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally
stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally
stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Question 25High Yield
**CLINICAL SITUATION**
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
This knee injury is best described as a
---
---
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
This knee injury is best described as a
---
---



Explanation
Medial plateau fracture dislocations are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the anteroposterior radiograph include an intact lateral column (lateral articular surface still in continuity with tibial shaft), centrolateral articular impaction, shortening, and condylar widening. The medial femoral condyle stays with the fractured medial tibial plateau segment.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair, but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair, but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 26High Yield
**CLINICAL SITUATION**
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Initial surgical management should consist of
---
---
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Initial surgical management should consist of
---
---



Explanation
Medial plateau fracture dislocations are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the anteroposterior radiograph include an intact lateral column (lateral articular surface still in continuity with tibial shaft), centrolateral articular impaction, shortening, and condylar widening. The medial femoral condyle stays with the fractured medial tibial plateau segment.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair,
but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair,
but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 27High Yield
**CLINICAL SITUATION**
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Figures 4 through 8 are the axial and coronal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
---
---
---
---
---
---
---
---
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Figures 4 through 8 are the axial and coronal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
---
---
---
---
---
---
---
---



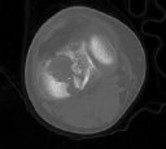
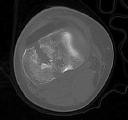



Explanation
Medial plateau fracture dislocations are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the anteroposterior radiograph include an intact lateral column (lateral articular surface still in continuity with tibial shaft), centrolateral articular impaction, shortening, and condylar widening. The medial femoral condyle stays with the fractured medial tibial plateau segment.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair, but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair, but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 28High Yield
**CLINICAL SITUATION**
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
The surgical approach for definitive reduction and stabilization of this pattern is
---
---
---
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
The surgical approach for definitive reduction and stabilization of this pattern is
---
---
---



Explanation
Medial plateau fracture dislocations are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the anteroposterior radiograph include an intact lateral column (lateral articular surface still in continuity with tibial shaft), centrolateral articular impaction, shortening, and condylar widening. The medial femoral condyle stays with the fractured medial tibial plateau segment.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair,
but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair,
but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 29High Yield
**CLINICAL SITUATION**
Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities.
What is the best next step in the patient’s evaluation?
---
Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities.
What is the best next step in the patient’s evaluation?
---




Explanation
The patient had an open fracture that was initially treated with what appears to be appropriate irrigation and debridement and intramedullary nail placement. The post-operative infection and need for rotational flap is worrisome,
but she has not had any issues since the flap. She has abundant callus formation but the fracture line is still visible and unchanged on 2 sets of radiographs. The patient has persistent pain. The best initial evaluation is to ensure that there is no underlying infection with laboratory studies, including a complete blood count (CBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Nuclear medicine studies have questionable utility, but may be helpful if the inflammatory markers from laboratory studies come back elevated. A CT scan is not warranted because the sequential radiographs show persistent fracture lines and no changes. The patient has a hypertrophic nonunion. Originally, she had appropriate treatment and has shown the ability to make callus, thus her biologic capacity appears to be intact and bone grafting is not needed. The hypertrophic nature of her fracture nonunion indicates that she needs more stability. The best treatment for a hypertrophic nonunion of the tibia is exchange nailing. Based on successive radiographs and the lack of healing, observation is probably just delaying the inevitable. Plating with retention of the nail can be useful in recalcitrant long bone non-union, especially in the femur.
but she has not had any issues since the flap. She has abundant callus formation but the fracture line is still visible and unchanged on 2 sets of radiographs. The patient has persistent pain. The best initial evaluation is to ensure that there is no underlying infection with laboratory studies, including a complete blood count (CBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Nuclear medicine studies have questionable utility, but may be helpful if the inflammatory markers from laboratory studies come back elevated. A CT scan is not warranted because the sequential radiographs show persistent fracture lines and no changes. The patient has a hypertrophic nonunion. Originally, she had appropriate treatment and has shown the ability to make callus, thus her biologic capacity appears to be intact and bone grafting is not needed. The hypertrophic nature of her fracture nonunion indicates that she needs more stability. The best treatment for a hypertrophic nonunion of the tibia is exchange nailing. Based on successive radiographs and the lack of healing, observation is probably just delaying the inevitable. Plating with retention of the nail can be useful in recalcitrant long bone non-union, especially in the femur.
Question 30High Yield
**CLINICAL SITUATION**
Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities.
Based on the radiographs shown in Figures 1 and 2, her tibia is a
---
---
Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities.
Based on the radiographs shown in Figures 1 and 2, her tibia is a
---
---
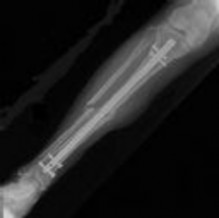
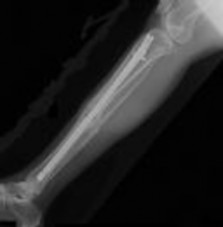
Explanation
The patient had an open fracture that was initially treated with what appears to be appropriate irrigation and debridement and intramedullary nail placement. The post-operative infection and need for rotational flap is worrisome, but she has not had any issues since the flap. She has abundant callus formation but the fracture line is still visible and unchanged on 2 sets of radiographs. The patient has persistent pain. The best initial evaluation is to ensure that there is no underlying infection with laboratory studies, including a complete blood count (CBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Nuclear medicine studies have questionable utility, but may be helpful if the inflammatory markers from laboratory studies come back elevated. A CT scan is not warranted because the sequential radiographs show persistent fracture lines and no changes. The patient has a hypertrophic nonunion. Originally, she had appropriate treatment and has shown the ability to make callus, thus her biologic capacity appears to be intact and bone grafting is not needed. The hypertrophic nature of her fracture nonunion indicates that she needs more stability. The best treatment for a hypertrophic nonunion of the tibia is exchange nailing. Based on successive radiographs and the lack of healing, observation is probably just delaying the inevitable. Plating with retention of the nail can be useful in recalcitrant long bone nonunions, especially in the femur.
Question 31High Yield
Suprapatellar intramedullary nailing for tibia fractures when compared to
infrapatellar nailing is associated with
infrapatellar nailing is associated with
Explanation
Suprapatellar nailing has been very useful in the management of proximal tibia fractures, allowing a better reduction. Both arthroscopy and MRI have been utilized after suprapatellar nailing to evaluate for changes in the patellofemoral joints, and no significant changes can be attributed to this technique. In a comparative study between suprapatellar nailing and standard (infrapatellar) nailing, both techniques showed excellent range of motion and no significant differences between the methods. In a separate study, it was noted that patients who underwent suprapatellar nailing did not complain of anterior knee pain that is often seen with standard nailing.
Question 32High Yield
**CLINICAL SITUATION**
Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities.
Assuming her workup is negative for any other causes, what is the best treatment option?
---
Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities.
Assuming her workup is negative for any other causes, what is the best treatment option?
---


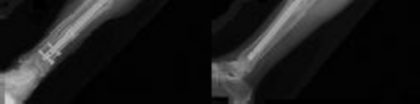
Explanation
The patient had an open fracture that was initially treated with what appears to be appropriate irrigation and debridement and intramedullary nail placement. The post-operative infection and need for rotational flap is worrisome, but she has not had any issues since the flap. She has abundant callus formation but the fracture line is still visible and unchanged on 2 sets of radiographs. The patient has persistent pain. The best initial evaluation is to ensure that there is no underlying infection with laboratory studies, including a complete blood count (CBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Nuclear medicine studies have questionable utility, but may be helpful if the inflammatory markers from laboratory studies come back elevated. A CT scan is not warranted because the sequential radiographs show persistent fracture lines and no changes. The patient has a hypertrophic nonunion. Originally, she had appropriate treatment and has shown the ability to make callus, thus her biologic capacity appears to be intact and bone grafting is not needed. The hypertrophic nature of her fracture nonunion indicates that she needs more stability. The best treatment for a hypertrophic nonunion of the tibia is exchange nailing. Based on successive radiographs and the lack of healing, observation is probably just delaying the inevitable. Plating with retention of the nail can be useful in recalcitrant long bone non-unions, especially in the femur.
Question 33High Yield
Figure 1 shows a patient with an open tibia fracture who presents to the emergency department after a propeller injury in brackish water (river water and sea water). What is the most appropriate antibiotic coverage for this patient?
---
---

Explanation
The clinical photo shows significant soft tissue wounds with associated tibia fracture. With the amount of soft tissue damage and periosteal stripping this would be classified as a Gustilo Type IIIB injury. The brackish water environment where this particular injury occurred influences the antibiotic choice secondary to the particular organisms found in this setting. Brackish water is made up of both fresh and salt water with common organisms that include Vibrio species, Aeromonas hydrophila, Pseudomonas species, Erysipelothrix rhusiopathiae, and Mycobacterium marinum. The combination of both Doxycycline (tetracycline) and Ceftazidime (third-generation cephalosporin) cover these particular pathogens. Standard antibiotic coverage for Gustilo Type I and II injures is 1st generation cephalosporin (cefazolin), with Type III being 1st generation cephalosporin and aminoglycoside (cefazolin and gentamicin) or a fluoroquinolone. In Type III injuries, Penicillin is commonly added in barnyard injuries for extended coverage of
soil-borne pathogens (clostridial species). Vancomycin is not indicated for coverage in marine environments, rather it is more commonly used for populations with a high prevalence of nosocomial infections. Sulfamethoxazole-trimethoprim is not used for open fracture coverage.
soil-borne pathogens (clostridial species). Vancomycin is not indicated for coverage in marine environments, rather it is more commonly used for populations with a high prevalence of nosocomial infections. Sulfamethoxazole-trimethoprim is not used for open fracture coverage.
Question 34High Yield
A 56-year-old woman sustains a type IIIB open tibial shaft fracture. She undergoes irrigation and debridement and intramedullary nailing with flap coverage 24 hours later. Cultures are taken pre-debridement and post-debridement. She develops a surgical site infection at 6 weeks, which requires removing the hardware and placing
show
Commented [1]:
an external fixator. Deep cultures are most likely to pathogens found in
show
Commented [1]:
an external fixator. Deep cultures are most likely to pathogens found in
Explanation
One study found only 8% of organisms grown on pre-debridement cultures eventually caused infection; 7% of cases with negative pre-debridement cultures became infected. Of cases that did become infected, pre-debridement cultures grew the infecting organism only 22% of the time. Post-debridement cultures were more accurate in predicting infection. However, of cases that became infected, the infecting organism was present on post-debridement cultures only 42% of the time. It is concluded that pre-debridement and post-debridement bacterial cultures from open fracture wounds are of essentially no value. It is recommended that they not be done.
In another study, before any interventions were performed, initial aerobic and anaerobic cultures of the wounds of 117 consecutive open extremity fractures grades I through III were obtained. The results of these cultures were correlated with the development of a wound infection. If an infection occurred, the organism grown from the infected wound was compared with any organism grown from the primary wound cultures. Of the initial cultures, 76% (89/117) did not demonstrate any growth, while the other 24% (28/117) only grew skin flora. There were only 7 (6%) wound infections, and 71% (5/7) initially did not grow any organisms. Of the isolates that grew from the initial cultures, none were the organisms that eventually led to
47
wound infections. The use of primary wound cultures in open extremity injuries has no value in the management of patients suffering from infections after long bone open extremity fractures.
In another study, before any interventions were performed, initial aerobic and anaerobic cultures of the wounds of 117 consecutive open extremity fractures grades I through III were obtained. The results of these cultures were correlated with the development of a wound infection. If an infection occurred, the organism grown from the infected wound was compared with any organism grown from the primary wound cultures. Of the initial cultures, 76% (89/117) did not demonstrate any growth, while the other 24% (28/117) only grew skin flora. There were only 7 (6%) wound infections, and 71% (5/7) initially did not grow any organisms. Of the isolates that grew from the initial cultures, none were the organisms that eventually led to
47
wound infections. The use of primary wound cultures in open extremity injuries has no value in the management of patients suffering from infections after long bone open extremity fractures.
Question 35High Yield
A 58-year-old man has a painful, warm, erythematous and fluctuant area over his left olecranon. An aspiration would be most likely to reveal
Explanation
[Discussion: Staphylococcus aureus is the most common causative organism in septic bursitis, making up 80% or more of cases of culture-proven septic bursitis (](https://www.uptodate.com/contents/septic-bursitis)https://www.uptodate.com/contents/septic-bursitis[). Staphylococcus aureus was the most frequent pathogen (217 out of 256 or 85%), followed by Streptococcus pyogenes (16), other streptococci (15), Enterococcus faecalis (4) and coagulase-negative staphylococci (2). Staphylococcus aureus is the most common causative organism in septic bursitis, making up 80% or more of cases of culture-proven septic bursitis (](https://www.uptodate.com/contents/septic-bursitis)https://www.uptodate.com/contents/septic-bursitis). Staphylococcus aureus was the most frequent pathogen (217 out of 256 or 85%), followed by Streptococcus pyogenes (16), other streptococci (15), Enterococcus faecalis (4) and coagulase-negative staphylococci (2).
Question 36High Yield
A 65-year-old woman with type II diabetes mellitus (most recent Hgb A1C was 8.2) has had 3 days of left knee pain. Physical examination of the left knee reveals erythema, warmth and a large effusion. Range of motion is painful and limited to 30 degrees of flexion. She is found to be hypotensive and not responding to volume resuscitation. She requires phenylephrine to maintain Mean Arterial Pressure (MAP) of 70. ESR and CRP are elevated and Lactate is 3.1 mmol/L. What is the next best intervention for this patient’s treatment?
Explanation
The patient is demonstrating signs of septic shock. Administration of antibiotics should not be delayed. Aspirating the knee joint and obtaining blood cultures can be rapidly accomplished to obtain accurate specimens. This should be followed immediately by administration of broad spectrum IV antibiotics. Patients with septic shock can be identified with a clinical construct of sepsis with persisting hypotension requiring vasopressors to maintain mean arterial pressure (MAP) ≥ 65 mmHg and having a serum lactate level > 2mmol/L (18 mg/dL) despite adequate volume resuscitation. With these criteria, hospital mortality is in excess of 40%.
Question 37High Yield
A 58-year-old man with a 50-year history of osteomyelitis of the left tibia has a painful ulceration of the anterior lower limb. Figure 1 is the clinical photograph of the wound, which had purulent discharge and an unpleasant odor. Figures 2 and 3 are radiographs of the left tibia. A biopsy reveals malignant degeneration. What are the most likely findings?
---
---
---
---



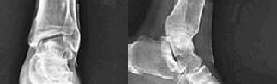
Explanation
Squamous cell carcinoma is the most common type of malignant tumor deriving from chronic osteomyelitis. The most frequently affected site is the tibia, followed by the femur. When the neoplasm invades the bone, there is either osteolytic erosion or a pathological fracture. Diagnosis is confirmed by biopsy at all suspicious wound sites. The malignant transformation most often results in squamous cell carcinoma and much more rarely in fibrosarcoma, osteosarcoma, reticulosarcoma, malignant fibrous histiocytoma or angiosarcoma. Many experts accept amputation as the best treatment option for carcinomatous transformation of chronic bone infections.
Question 38High Yield
A 56-year-old man with poorly controlled diabetes mellitus has rapidly developing and advancing erythema, warmth and swelling with bullae formation on the left lower extremity. These findings appear to be advancing proximally several millimeters per hour. Culture results are most likely to reveal
Explanation
Necrotizing fasciitis (NF) results in the death of the body's soft tissue. It is a severe disease of sudden onset that spreads rapidly. Symptoms include red or purple skin in the affected area, with severe pain, fever, and vomiting. The most commonly affected areas are the limbs and perineum. Early diagnosis is difficult as the disease often looks like a simple superficial skin infection in the early stages. While a number of laboratory and imaging modalities can raise the suspicion for necrotizing fasciitis, the gold standard for diagnosis is a surgical exploration in the setting of high suspicion. When in doubt, a small "keyhole" incision can be made into the affected tissue. If a finger easily separates the tissue along the fascial plane,
the diagnosis is confirmed and an extensive debridement should be performed. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score can be utilized to risk stratify people who have signs of cellulitis and determine the likelihood of necrotizing fasciitis being present. It uses six serologic measures, including C-reactive protein, total white blood cell count, hemoglobin, sodium, creatinine and glucose.
Polymicrobial synergistic infection was the most common cause of necrotizing fasciitis (48 patients; 53.9%) with streptococci and enterobacteriaceae being the most common isolates. Group-A streptococcus was the most common cause of monomicrobial necrotizing fasciitis. The most common associated comorbidity was diabetes mellitus (63 patients; 70.8%).
the diagnosis is confirmed and an extensive debridement should be performed. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score can be utilized to risk stratify people who have signs of cellulitis and determine the likelihood of necrotizing fasciitis being present. It uses six serologic measures, including C-reactive protein, total white blood cell count, hemoglobin, sodium, creatinine and glucose.
Polymicrobial synergistic infection was the most common cause of necrotizing fasciitis (48 patients; 53.9%) with streptococci and enterobacteriaceae being the most common isolates. Group-A streptococcus was the most common cause of monomicrobial necrotizing fasciitis. The most common associated comorbidity was diabetes mellitus (63 patients; 70.8%).
Question 39High Yield
Six weeks after open reduction internal fixation of a closed tibial pilon fracture, a patient has a draining wound with surrounding erythema and swelling. Radiographs show lucency around screws. What is the most appropriate treatment sequence?
Explanation
Management of acutely infected wounds is primarily surgical. Osteomyelitis frequently involves Orthopaedic hardware, which would ideally be removed or replaced given biofilm involvement. Multiple operative cultures of fluid collections, soft tissues and bone should routinely be obtained. Culture yield is highest if cultures are obtained before empiric antibiotic treatment is started. Tissue samples are greatly preferred to swabs, which are notoriously inaccurate.
Question 40High Yield
**CLINICAL SITUATION**
Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
She undergoes a closed reduction in the emergency department. Figures 2 through 5 are post-reduction CT images. What is the ideal surgical approach to address this fracture?
---
---
---
---
---
Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
She undergoes a closed reduction in the emergency department. Figures 2 through 5 are post-reduction CT images. What is the ideal surgical approach to address this fracture?
---
---
---
---
---

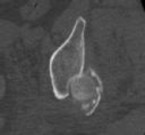
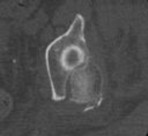
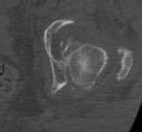

Explanation
The patient sustained a posterior wall fracture dislocation. For acetabular fractures, the position of the limb in space at the time of impact (in terms of the amount of flexion/extension, internal/external rotation, and adduction/abduction) will dictate the fracture pattern. For posterior wall fracture patterns, the limb is in some degree of flexion, adduction, and internal rotation. Other combinations are possible to contribute to an acetabular fracture but not likely to contribute to a posterior wall pattern.
This posterior wall fracture pattern can be addressed from a standard Kocher-Langenbeck approach for both fixation and arthroplasty. There is no significant cranial or anterior extension of the fracture that would necessitate a modified posterior approach or greater trochanteric osteotomy. The other listed approaches would not be appropriate.
Indications for total hip arthroplasty are continuing to evolve and many patient-specific and fracture specific variables are involved. Several studies have investigated this issue and the common variables that influence the success of primary fixation are related to the age of the patient, greater than 50 years as well as associated bone quality and how these are affected with the fracture. The presence of marginal impaction suggests significant insult to the cartilage. In the presence of pre-existing cartilage wear, the likelihood of success with primary fixation is decreased. The presence of significant comminution of the fracture (greater than 3 fragments) also suggests decreased success with primary fixation. The other factors listed can contribute to perioperative morbidity but not as clearly when compared to the three listed in
. In the clinical setting of a patient older than 50 years old with a comminuted fracture, marginal impaction, and femoral head damage, there should be serious consideration for combined fracture fixation and acute total hip arthroplasty. Delayed arthroplasty can be an option in some patients, but clinical outcomes have not been as favorable as acute combined treatment.
Although urethral tears, rib fractures, and subdural hematoma are commonly involved with high-energy accidents and are routinely investigated through advanced trauma life support (ATLS) protocols, the ipsilateral knee has not received such focus. In a recent multi-center study, 15% of patients were found to have ipsilateral knee symptoms within a period of 1 year from the date of injury. The patterns of knee injury included 56 fractures (29%), 49 ligamentous lesions (25%), and 88 miscellaneous (46%) causes, including bone bruises, wounds, and swelling.
Multi-ligamentous knee injuries can be occult and a detailed examination of the knee should be standard in these patients upon secondary and tertiary surveys.
This posterior wall fracture pattern can be addressed from a standard Kocher-Langenbeck approach for both fixation and arthroplasty. There is no significant cranial or anterior extension of the fracture that would necessitate a modified posterior approach or greater trochanteric osteotomy. The other listed approaches would not be appropriate.
Indications for total hip arthroplasty are continuing to evolve and many patient-specific and fracture specific variables are involved. Several studies have investigated this issue and the common variables that influence the success of primary fixation are related to the age of the patient, greater than 50 years as well as associated bone quality and how these are affected with the fracture. The presence of marginal impaction suggests significant insult to the cartilage. In the presence of pre-existing cartilage wear, the likelihood of success with primary fixation is decreased. The presence of significant comminution of the fracture (greater than 3 fragments) also suggests decreased success with primary fixation. The other factors listed can contribute to perioperative morbidity but not as clearly when compared to the three listed in
. In the clinical setting of a patient older than 50 years old with a comminuted fracture, marginal impaction, and femoral head damage, there should be serious consideration for combined fracture fixation and acute total hip arthroplasty. Delayed arthroplasty can be an option in some patients, but clinical outcomes have not been as favorable as acute combined treatment.
Although urethral tears, rib fractures, and subdural hematoma are commonly involved with high-energy accidents and are routinely investigated through advanced trauma life support (ATLS) protocols, the ipsilateral knee has not received such focus. In a recent multi-center study, 15% of patients were found to have ipsilateral knee symptoms within a period of 1 year from the date of injury. The patterns of knee injury included 56 fractures (29%), 49 ligamentous lesions (25%), and 88 miscellaneous (46%) causes, including bone bruises, wounds, and swelling.
Multi-ligamentous knee injuries can be occult and a detailed examination of the knee should be standard in these patients upon secondary and tertiary surveys.
Question 41High Yield
**CLINICAL SITUATION**
Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
Which factors will lead a surgeon to pursue fracture fixation and acute total hip arthroplasty instead of fixation alone?
---
Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
Which factors will lead a surgeon to pursue fracture fixation and acute total hip arthroplasty instead of fixation alone?
---

Explanation
The patient sustained a posterior wall fracture dislocation. For acetabular fractures, the position of the limb in space at the time of impact (in terms of the amount of flexion/extension, internal/external rotation, and adduction/abduction) will dictate the fracture pattern. For posterior wall fracture patterns, the limb is in some degree of flexion, adduction, and internal rotation. Other combinations are possible to contribute to an acetabular fracture but not likely to contribute to a posterior wall pattern.
This posterior wall fracture pattern can be addressed from a standard Kocher-Langenbeck approach for both fixation and arthroplasty. There is no significant cranial or anterior extension of the fracture that would necessitate a modified
posterior approach or greater trochanteric osteotomy. The other listed approaches would not be appropriate.
Indications for total hip arthroplasty are continuing to evolve and many patient-specific and fracture specific variables are involved. Several studies have investigated this issue and the common variables that influence the success of primary fixation are related to the age of the patient, greater than 50 years as well as associated bone quality and how these are affected with the fracture. The presence of marginal impaction suggests significant insult to the cartilage. In the presence of pre-existing cartilage wear, the likelihood of success with primary fixation is decreased. The presence of significant comminution of the fracture (greater than 3 fragments) also suggests decreased success with primary fixation. The other factors listed can contribute to perioperative morbidity but not as clearly when compared to the three listed in
. In the clinical setting of a patient older than 50 years old with a comminuted fracture, marginal impaction, and femoral head damage, there should be serious consideration for combined fracture fixation and acute total hip arthroplasty. Delayed arthroplasty can be an option in some patients, but clinical outcomes have not been as favorable as acute combined treatment.
Although urethral tears, rib fractures, and subdural hematoma are commonly involved with high-energy accidents and are routinely investigated through advanced trauma life support (ATLS) protocols, the ipsilateral knee has not received such focus. In a recent multi-center study, 15% of patients were found to have ipsilateral knee symptoms within a period of 1 year from the date of injury. The patterns of knee injury included 56 fractures (29%), 49 ligamentous lesions (25%), and 88 miscellaneous (46%) causes, including bone bruises, wounds, and swelling. Multi-ligamentous knee injuries can be occult and a detailed examination of the knee should be standard in these patients upon secondary and tertiary surveys.
This posterior wall fracture pattern can be addressed from a standard Kocher-Langenbeck approach for both fixation and arthroplasty. There is no significant cranial or anterior extension of the fracture that would necessitate a modified
posterior approach or greater trochanteric osteotomy. The other listed approaches would not be appropriate.
Indications for total hip arthroplasty are continuing to evolve and many patient-specific and fracture specific variables are involved. Several studies have investigated this issue and the common variables that influence the success of primary fixation are related to the age of the patient, greater than 50 years as well as associated bone quality and how these are affected with the fracture. The presence of marginal impaction suggests significant insult to the cartilage. In the presence of pre-existing cartilage wear, the likelihood of success with primary fixation is decreased. The presence of significant comminution of the fracture (greater than 3 fragments) also suggests decreased success with primary fixation. The other factors listed can contribute to perioperative morbidity but not as clearly when compared to the three listed in
. In the clinical setting of a patient older than 50 years old with a comminuted fracture, marginal impaction, and femoral head damage, there should be serious consideration for combined fracture fixation and acute total hip arthroplasty. Delayed arthroplasty can be an option in some patients, but clinical outcomes have not been as favorable as acute combined treatment.
Although urethral tears, rib fractures, and subdural hematoma are commonly involved with high-energy accidents and are routinely investigated through advanced trauma life support (ATLS) protocols, the ipsilateral knee has not received such focus. In a recent multi-center study, 15% of patients were found to have ipsilateral knee symptoms within a period of 1 year from the date of injury. The patterns of knee injury included 56 fractures (29%), 49 ligamentous lesions (25%), and 88 miscellaneous (46%) causes, including bone bruises, wounds, and swelling. Multi-ligamentous knee injuries can be occult and a detailed examination of the knee should be standard in these patients upon secondary and tertiary surveys.
Question 42High Yield
**CLINICAL SITUATION**
Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
In this patient, what other potential injury can be associated with this fracture pattern and is commonly overlooked?
---
Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
In this patient, what other potential injury can be associated with this fracture pattern and is commonly overlooked?
---

Explanation
The patient sustained a posterior wall fracture dislocation. For acetabular fractures, the position of the limb in space at the time of impact (in terms of the amount of flexion/extension, internal/external rotation, and adduction/abduction) will dictate the fracture pattern. For posterior wall fracture patterns, the limb is in some degree of flexion, adduction, and internal rotation. Other combinations are possible to contribute to an acetabular fracture but not likely to contribute to a posterior wall pattern.
This posterior wall fracture pattern can be addressed from a standard Kocher-Langenbeck approach for both fixation and arthroplasty. There is no significant cranial or anterior extension of the fracture that would necessitate a modified posterior approach or greater trochanteric osteotomy. The other listed approaches would not be appropriate.
Indications for total hip arthroplasty are continuing to evolve and many patient-specific and fracture specific variables are involved. Several studies have investigated this issue and the common variables that influence the success of primary fixation are related to the age of the patient, greater than 50 years as well as associated bone quality and how these are affected with the fracture. The presence of marginal impaction suggests significant insult to the cartilage. In the presence of pre-existing cartilage wear, the likelihood of success with primary fixation is decreased. The presence of significant comminution of the fracture (greater than 3 fragments) also suggests decreased success with primary fixation. The other factors listed can contribute to perioperative morbidity but not as clearly when compared to the three listed in
. In the clinical setting of a patient older than 50 years old with a comminuted fracture, marginal impaction, and femoral head damage,
there should be serious consideration for combined fracture fixation and acute total hip arthroplasty. Delayed arthroplasty can be an option in some patients, but clinical outcomes have not been as favorable as acute combined treatment.
Although urethral tears, rib fractures, and subdural hematoma are commonly involved with high-energy accidents and are routinely investigated through advanced trauma life support (ATLS) protocols, the ipsilateral knee has not received such focus. In a recent multi-center study, 15% of patients were found to have ipsilateral knee symptoms within a period of 1 year from the date of injury. The patterns of knee injury included 56 fractures (29%), 49 ligamentous lesions (25%), and 88 miscellaneous (46%) causes, including bone bruises, wounds, and swelling. Multi-ligamentous knee injuries can be occult and a detailed examination of the knee should be standard in these patients upon secondary and tertiary surveys.
This posterior wall fracture pattern can be addressed from a standard Kocher-Langenbeck approach for both fixation and arthroplasty. There is no significant cranial or anterior extension of the fracture that would necessitate a modified posterior approach or greater trochanteric osteotomy. The other listed approaches would not be appropriate.
Indications for total hip arthroplasty are continuing to evolve and many patient-specific and fracture specific variables are involved. Several studies have investigated this issue and the common variables that influence the success of primary fixation are related to the age of the patient, greater than 50 years as well as associated bone quality and how these are affected with the fracture. The presence of marginal impaction suggests significant insult to the cartilage. In the presence of pre-existing cartilage wear, the likelihood of success with primary fixation is decreased. The presence of significant comminution of the fracture (greater than 3 fragments) also suggests decreased success with primary fixation. The other factors listed can contribute to perioperative morbidity but not as clearly when compared to the three listed in
. In the clinical setting of a patient older than 50 years old with a comminuted fracture, marginal impaction, and femoral head damage,
there should be serious consideration for combined fracture fixation and acute total hip arthroplasty. Delayed arthroplasty can be an option in some patients, but clinical outcomes have not been as favorable as acute combined treatment.
Although urethral tears, rib fractures, and subdural hematoma are commonly involved with high-energy accidents and are routinely investigated through advanced trauma life support (ATLS) protocols, the ipsilateral knee has not received such focus. In a recent multi-center study, 15% of patients were found to have ipsilateral knee symptoms within a period of 1 year from the date of injury. The patterns of knee injury included 56 fractures (29%), 49 ligamentous lesions (25%), and 88 miscellaneous (46%) causes, including bone bruises, wounds, and swelling. Multi-ligamentous knee injuries can be occult and a detailed examination of the knee should be standard in these patients upon secondary and tertiary surveys.
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon