Orthopedic Basic Review | Dr Hutaif Basic Science Revie -...
14 Apr 2026
46 min read
55 Views

Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Basic Review | Dr Hutaif Basic Sci...
00:00
Start Quiz
Question 1High Yield
A patient sustained a transverse humeral shaft fracture 6 months ago and presently complains of pain and instability at the area of injury. A plain radiograph is shown in Figure A and on exam there is gross motion at the fracture site. What is the most appropriate definitive treatment?

Explanation
Figure A shows an atrophic nonunion of a humeral shaft fracture.
Humeral shaft nonunion is defined as failure of healing after 6 months. The nonunion can be hypertrophic, oligotrophic, or atrophic. The risk of atrophic nonunion increases with bone loss, open fractures, and infection among other factors.
As Jupiter has described, the application of a compression plate to stabilize the fracture fragments with autogenous cancellous bone graft has been successful as long as there is a well vascularized envelope of muscle.
Humeral shaft nonunion is defined as failure of healing after 6 months. The nonunion can be hypertrophic, oligotrophic, or atrophic. The risk of atrophic nonunion increases with bone loss, open fractures, and infection among other factors.
As Jupiter has described, the application of a compression plate to stabilize the fracture fragments with autogenous cancellous bone graft has been successful as long as there is a well vascularized envelope of muscle.
Question 2High Yield
Increasing tibial polyethylene conformity can have what effect on fixed bearing total knee arthroplasty?
Explanation
DISCUSSION: Increasing conformity between the tibial polyethylene bearing and the femoral component has desirable and undesirable consequences. Increased conformity increases the contact area and thereby reduces contact stress within the polyethylene. This can lead to less risk of polyethylene wear, fracture, and delamination. However, increasing conformity also limits the ability of the femur to roll back during flexion, and may transfer increased shear stress to the fixation surfaces of the implants.
REFERENCES: D’Lima DD, Chen PC, Colwell CW Jr: Polyethylene contact stresses, articular congruity, and knee alignment. Clin Orthop Relat Res 2001;392:232-238.
Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
REFERENCES: D’Lima DD, Chen PC, Colwell CW Jr: Polyethylene contact stresses, articular congruity, and knee alignment. Clin Orthop Relat Res 2001;392:232-238.
Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
Question 3High Yield
What percentage of the human genome represents the actual genes:
Explanation
The percentage of the genome that represents the sequence of our genes is approximately 5%. The rest of the genome codes are for initiator and termination sequences, maintenance functions, and unknown functions.
Question 4High Yield
A 36-year-old man has a 2-day history of acute lower back pain with severe radicular symptoms in the left lower extremity. The patient has a positive straight leg test at 40 degrees on the left side and mild decreased sensation on the dorsum of the left foot. What is the most appropriate management at this time?
Explanation
In the absence of any severe progressive neurologic deficits or other red flags, the most appropriate management for an acute lumbar disk herniation is nonsurgical care. Conservative treatments such as limited bed rest, anti-inflammatory medications, and judicious use of pain medications are appropriate in this clinical situation. Up to 90% of patients will experience a resolution of symptoms without the need for surgical intervention within a 3-month window. In the acute setting, with no neurologic deficits, immediate MRI of the lumbar spine is neither beneficial nor warranted. Likewise,without signs of an acute deficit, emergent surgical intervention and caudal epidural steroid injections are not needed.
Question 5High Yield
A 35-year-old woman is bitten on her left index finger by a snake in her backyard. Management of snake bites includes all of the following except:
Explanation
There are different snake bite protocols depending on the species of snake. However, common steps in all snake bite protocols include keeping the patient emotionally and physically still, calling for help immediately, applying a moderately tight tourniquet proximally to prevent further spread of venom, and capture or identification of the snake. Local injection of the antivenin in the fingers or toes is contraindicated.
Question 6High Yield
Which of the following is most commonly associated with the use of bisphosphonates in the setting of
metastatic breast cancer?
metastatic breast cancer?
Explanation
Bisphosphonate therapy in breast cancer patients is indicated for the correction of hypercalcemia and the prevention of cancer treatment-induced bone loss. Bisphosphonates reduce metastatic bone pain in at least 50% of patients and can reduce the frequency of skeletal-related events by 30% to 40%. Osteonecrosis of the jaw could occur in up to 2.5% of breast cancer patients during longterm bisphosphonate therapy.
Question 7High Yield
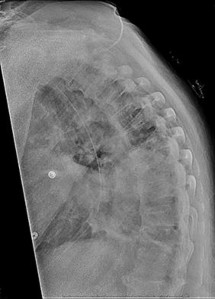
Figure 81 is a lateral thoracic spine radiograph of a 76-year-old man with a history of ankylosing spondylitis who falls and strikes his back. He has moderate thoracic discomfort. An initial examination does not reveal neurologic deficits. He is discharged home that day, but returns 3 days later with profound weakness in his legs. Which imaging study should have been obtained at his initial presentation?
Explanation
Patients with ankylosing spondylitis are at high risk for occult vertebral fractures that are not readily detectable on radiographs. The treating surgeon must have a high suspicion for fractures in these patients and pursue further imaging of the spine with CT and (often) MRI. Even among patients who are neurologically intact, fracture displacement and neurologic deterioration can occur if fractures are not recognized early and appropriately stabilized. Fractures in patients with ankylosing spondylitis are extremely unstable and are associated with high risk for delayed neurological deterioration. Although plain film imaging of the entire spine should be considered, occult fractures can easily be missed. Imaging of the sacroiliac joints can be helpful to establish the diagnosis of ankylosing spondylitis but would not identify an occult fracture of the vertebra in this patient.
RECOMMENDED READINGS
[Finkelstein JA, Chapman JR, Mirza S. Occult vertebral fractures in ankylosing spondylitis. Spinal Cord. 1999 Jun;37(6):444-7. PubMed PMID: 10432265. ](http://www.ncbi.nlm.nih.gov/pubmed/10432265)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10432265) [Harrop JS, Sharan A, Anderson G, Hillibrand AS, Albert TJ, Flanders A, Vaccaro AR. Failure of standard imaging to detect a cervical fracture in a patient with ankylosing spondylitis. Spine (Phila Pa 1976). 2005 Jul 15;30(14):E417-9. PubMed PMID: 16025019. ](http://www.ncbi.nlm.nih.gov/pubmed/16025019)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16025019)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16025019)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16025019)
Westerveld LA, Verlaan JJ, Oner FC. Spinal fractures in patients with ankylosing spinal disorders: a systematic review of the literature on treatment, neurological status and
[complications. Eur Spine J. 2009 Feb;18(2):145-56. doi: 10.1007/s00586-008-0764-0. Epub 2008 Sep 13. Review. PubMed PMID: 18791749. ](http://www.ncbi.nlm.nih.gov/pubmed/18791749)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18791749)
RECOMMENDED READINGS
[Finkelstein JA, Chapman JR, Mirza S. Occult vertebral fractures in ankylosing spondylitis. Spinal Cord. 1999 Jun;37(6):444-7. PubMed PMID: 10432265. ](http://www.ncbi.nlm.nih.gov/pubmed/10432265)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10432265) [Harrop JS, Sharan A, Anderson G, Hillibrand AS, Albert TJ, Flanders A, Vaccaro AR. Failure of standard imaging to detect a cervical fracture in a patient with ankylosing spondylitis. Spine (Phila Pa 1976). 2005 Jul 15;30(14):E417-9. PubMed PMID: 16025019. ](http://www.ncbi.nlm.nih.gov/pubmed/16025019)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/16025019)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16025019)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16025019)
Westerveld LA, Verlaan JJ, Oner FC. Spinal fractures in patients with ankylosing spinal disorders: a systematic review of the literature on treatment, neurological status and
[complications. Eur Spine J. 2009 Feb;18(2):145-56. doi: 10.1007/s00586-008-0764-0. Epub 2008 Sep 13. Review. PubMed PMID: 18791749. ](http://www.ncbi.nlm.nih.gov/pubmed/18791749)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18791749)
Question 8High Yield
A 42-year-old male sustains a closed, isolated ulna shaft fracture with 2mm displacement and 3 degrees valgus angulation. He is treated conservatively with early range of motion but presents at one year with a painful atrophic nonunion. What treatment is indicated at this time?
Explanation
Appropriate treatment of an atrophic nonunion of the ulna includes open reduction and internal fixation with autogenous bone grafting. The atrophic nature of the nonunion reveals that biology, and not necessarily stability, is the major issue of the nonunion. The referenced article by Ring et al reviews a case series of these patients and found that even in the face of significant preoperative bone resorption, good clinical outcomes and union rate is possible with open plating and grafting. The article by Street reviews intramedullary nailing/pinning of the forearm, and found a 7% nonunion rate with this technique.
Question 9High Yield
Four days ago, a 13-year-old boy stubbed his toe on a chair while running barefoot through his home.
He received no treatment at the time. He is now seen at the orthopaedic clinic with the radiograph and clinical photograph shown in Figures 27a and 27b. What is the next step in management?
He received no treatment at the time. He is now seen at the orthopaedic clinic with the radiograph and clinical photograph shown in Figures 27a and 27b. What is the next step in management?
Explanation
The boy has a Seymour’s fracture of the toe. The germinal matrix of the nail bed is trapped in the fracture site; thus this should be considered an open fracture. Ideally, it should be treated with open reduction and internal fixation and use of antibiotics at the time of injury. Because this is a delayed presentation, it is even more important to do a formal open reduction and a good irrigation and debridement, followed by the use of postoperative antibiotics. Because the fracture has been displaced for several days, overall management will be easier if the fracture reduction is maintained with pin fixation.
REFERENCE: Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL. American Academy of Orthopaedic Surgeons, 2008, p 737.
REFERENCE: Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL. American Academy of Orthopaedic Surgeons, 2008, p 737.
Question 10High Yield
A 24-year-old man presents for treatment of a painful fifth toe deformity. He had the deformity for 10 years and notes that it is getting progressively worse. On examination, a claw toe deformity is present. There is 90° of fixed hyperextension of the metatarsophalangeal joint, 70° of flexion at the interphalangeal joint, and a painful corn on the distal tip of the phalanx. The patient would like surgical correction. Which procedure is most likely to give him relief of pain and correction of deformity:
Explanation
C orrection of a fixed claw fifth toe deformity is not an easy procedure. The customary procedures used for correction of other lesser toe deformities are not always successful. In this patient, PIP arthroplasty or arthrodesis alone will not correct this deformity. The deformity requires a subtotal or complete proximal phalangectomy. Although this procedure corrects the deformity, patients must know that they will inevitably have a floppy fifth toe.
Question 11High Yield
The most common soft tissue sarcoma of the foot and ankle is:
Explanation
Malignant melanoma is the most common soft tissue malignancy of the foot; however, synovial sarcoma is the most common soft tissue sarcoma. There may be a long duration of presence of the mass, with or without growth of the lesion. When one evaluates a patient with a small or large soft tissue mass on the foot, synovial sarcoma should be considered in the differential diagnosis.
Question 12High Yield
A 70-year-old man who underwent an uncomplicated large rotator cuff repair 6 months ago is now seeking a second opinion regarding persistent pain and weakness in his shoulder. Examination reveals that his incision is well healed and unreactive. The surgical report suggests that the tendons were secured back to bone with sutures through the greater tuberosity. Figure 28 shows a radiograph that was obtained 1 week ago. What is the most likely diagnosis?
Explanation
Symptoms can persist following a rotator cuff repair for a variety of reasons. In the early postoperative period, infection is the primary concern. Stiffness and loss of motion can occur because of postoperative scarring. Complex regional pain syndrome can occur but is rare, and the diagnosis is not made with a plain radiograph. This radiograph shows a superiorly migrated humeral head that articulates with the acromion, indicating that the repair has failed. While large to massive tears may fail more commonly than once thought, the clinical outcome may be satisfactory in many patients.
REFERENCES: Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213.
Jost B, Pfirrmann CW, Gerber C, Switzerland Z: Clinical outcome after structural failure of rotator cuff repairs. J Bone Joint Surg Am 2000;82:304-314.
REFERENCES: Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213.
Jost B, Pfirrmann CW, Gerber C, Switzerland Z: Clinical outcome after structural failure of rotator cuff repairs. J Bone Joint Surg Am 2000;82:304-314.
Question 13High Yield
Figure 89



Explanation
- Cubital tunnel syndrome_
Question 14High Yield
Figures 46a through 46e show the radiographs of a 22-year-old man who injured his wrist in a motorcycle accident. He has no other injuries. What is the best course of action?
Explanation
The patient has a fracture-dislocation of the radiocarpal joint. Attached to the large radial styloid fragment are the extrinsic wrist ligaments to the carpus. This injury should be treated with open reduction and internal fixation of the styloid fracture. Radiolunate fusion or extrinsic ligament repair is suggested when the extrinsic ligaments are ruptured, resulting in ulnar translocation of the carpus.
REFERENCES: Dumontier C, Meyer ZU, Reckendorf G, et al: Radiocarpal dislocations: Classification and proposal for treatment: A review of twenty-seven cases. J Bone Joint Surg Am 2001;83:212.
Bilos ZJ, Pankovich AM, Yelda S: Fracture-dislocation of the radiocarpal joint: A clinical study of five cases. J Bone Joint Surg Am 1977;59:198-203.
REFERENCES: Dumontier C, Meyer ZU, Reckendorf G, et al: Radiocarpal dislocations: Classification and proposal for treatment: A review of twenty-seven cases. J Bone Joint Surg Am 2001;83:212.
Bilos ZJ, Pankovich AM, Yelda S: Fracture-dislocation of the radiocarpal joint: A clinical study of five cases. J Bone Joint Surg Am 1977;59:198-203.
Question 15High Yield
A 55-year-old patient is seeking a surgical consultation for a painful flatfoot deformity that has failed to respond to nonsteroidal anti-inflammatory drugs, shoe and activity modifications, and orthoses. The patient is of medium build, a nonsmoker, and has no history of diabetes mellitus. Radiographs are shown in Figures 43a through 43c. Based on these findings, treatment should consist of
Explanation
The patient has a degenerative collapse of the midfoot through the tarsometatarsal joints with significant forefoot abduction; therefore, a midfoot arthrodesis is required to address the arthritic joints and deformity at the tarsometatarsal articulation. All of the other procedures correct hindfoot deformities and therefore would not be appropriate treatment.
REFERENCES: Brage M: Degenerative joint disease of the midfoot. Foot Ankle Clin 1999;4:355-367.
Mann RA, Prieskorn D, Sobel M: Mid-tarsal and tarsometatarsal arthrodesis for primary degenerative osteoarthrosis or osteoarthrosis after trauma. J Bone Joint Surg Am
1996;78:1376-1385.
REFERENCES: Brage M: Degenerative joint disease of the midfoot. Foot Ankle Clin 1999;4:355-367.
Mann RA, Prieskorn D, Sobel M: Mid-tarsal and tarsometatarsal arthrodesis for primary degenerative osteoarthrosis or osteoarthrosis after trauma. J Bone Joint Surg Am
1996;78:1376-1385.
Question 16High Yield
A 65-year-old female sustained the injury seen in Figure A after a slip and fall getting out of the shower. She is an avid golfer and walks the course on most days. Her past medical history includes borderline hypertension and migraine headaches. Which treatment option has shown to have the lowest re-operation rate and best clinical outcomes scores in this patient population?

Explanation
Figure A shows a displaced right femoral neck fracture in an active, healthy elderly patient. Treatment of her hip fracture with total hip arthroplasty (THA) has shown to have the lowest re-operation rates and best functional outcome scores when compared to internal fixation devices and hemiarthroplasty.
Large studies have shown the incidence of femoral head AVN to be approximately 30-45% with displaced femoral neck fractures (Garden III-IV). For this reason, treatment of these injuries in elderly patients have supported arthroplasty over ORIF. Treatment of patients with THA vs. hemiarthroplasty have also been investigated. Studies have shown that THA has lower reoperation rates and improved functional outcome scores in younger, active elderly patients compared to hemiarthroplasty.
Avery et al. prospectively followed a cohort of 81 patients treated with THA vs. hemiarthroplasty in high functioning elderly patients with displaced femoral neck fractures. They showed a lower mortality rate (p = 0.013) and trend towards superior function in patients treated with THA. Advantages with THA vs hemiarthroplasty must be traded off against a slightly higher risk of dislocations.
Hedbeck et al. performed a randomized controlled trial involving 120 elderly patients with acutely displaced femoral neck fractures that were treated with either bipolar hemiarthroplasty or THA. They showed Harris hip scores and EQ-5D scores in favour of THA. They suggested treatment with THA in elderly, lucid patients with displaced femoral neck fractures.
Figure A is a AP pelvic radiograph. The most obvious finding is a displaced femoral neck fracture.
Incorrect Answers:
Answers 1,2,3: Arthroplasty of any type has been shown to have the least amount of complications and greatest functional outcome scores compared to internal fixation devices. Indications for treatment of femoral neck fractures with internal fixation include: (1) stable or unstable fractures in young or physiologically young patients (2) stable fragility fractures (Garden I and II) in low demand elderly patients.
Answer 4: Hemiarthroplasty is most appropriate for displaced femoral neck fractures (Garden III or IV) in low-functional demand elderly patients.
Large studies have shown the incidence of femoral head AVN to be approximately 30-45% with displaced femoral neck fractures (Garden III-IV). For this reason, treatment of these injuries in elderly patients have supported arthroplasty over ORIF. Treatment of patients with THA vs. hemiarthroplasty have also been investigated. Studies have shown that THA has lower reoperation rates and improved functional outcome scores in younger, active elderly patients compared to hemiarthroplasty.
Avery et al. prospectively followed a cohort of 81 patients treated with THA vs. hemiarthroplasty in high functioning elderly patients with displaced femoral neck fractures. They showed a lower mortality rate (p = 0.013) and trend towards superior function in patients treated with THA. Advantages with THA vs hemiarthroplasty must be traded off against a slightly higher risk of dislocations.
Hedbeck et al. performed a randomized controlled trial involving 120 elderly patients with acutely displaced femoral neck fractures that were treated with either bipolar hemiarthroplasty or THA. They showed Harris hip scores and EQ-5D scores in favour of THA. They suggested treatment with THA in elderly, lucid patients with displaced femoral neck fractures.
Figure A is a AP pelvic radiograph. The most obvious finding is a displaced femoral neck fracture.
Incorrect Answers:
Answers 1,2,3: Arthroplasty of any type has been shown to have the least amount of complications and greatest functional outcome scores compared to internal fixation devices. Indications for treatment of femoral neck fractures with internal fixation include: (1) stable or unstable fractures in young or physiologically young patients (2) stable fragility fractures (Garden I and II) in low demand elderly patients.
Answer 4: Hemiarthroplasty is most appropriate for displaced femoral neck fractures (Garden III or IV) in low-functional demand elderly patients.
Question 17High Yield
A nondisplaced fracture of the proximal medial femoral neck proximal to the lesser trochanter is noted at the time of insertion of a cementless tapered wedge-type femoral component in a total hip arthroplasty. Appropriate perioperative management should include which of the following?

Explanation
DISCUSSION: The fracture should be explored in its entirety. If it remains in the intertrochanteric region, a single cerclage cable passed above the lesser trochanter and tightened around the femoral component is appropriate. A more distal or displaced fracture should be repaired with cerclage cables and consideration for revision of the femoral component with a long-stemmed or cemented implant should be given.
REFERENCES: Sharkey PF, Hozack WJ, Booth RE, et al: Intraoperative femoral fractures in cementless total hip arthroplasty. Orthop Rev 1992;21:337-342.
Sharkey PF, Wolf LR, Hume EL, et al: Insertional femoral fracture: A biomechanical study of femoral component stability. Semin Arthroplasty 1990;1:91-94.
Figure 39a Figure 39b Figure 39c
DISCUSSION: The fracture should be explored in its entirety. If it remains in the intertrochanteric region, a single cerclage cable passed above the lesser trochanter and tightened around the femoral component is appropriate. A more distal or displaced fracture should be repaired with cerclage cables and consideration for revision of the femoral component with a long-stemmed or cemented implant should be given.
REFERENCES: Sharkey PF, Hozack WJ, Booth RE, et al: Intraoperative femoral fractures in cementless total hip arthroplasty. Orthop Rev 1992;21:337-342.
Sharkey PF, Wolf LR, Hume EL, et al: Insertional femoral fracture: A biomechanical study of femoral component stability. Semin Arthroplasty 1990;1:91-94.
Figure 39a Figure 39b Figure 39c
Question 18High Yield
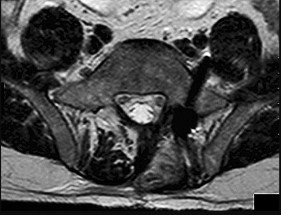
A 36-year-old woman has neck pain in the upper cervical region and occipital discomfort after being involved in a motor vehicle accident. Examination reveals no forehead or scalp lacerations. The neurologic examination is normal. A CT scan shows no evidence of bony injury. Figures 39a and 39b show a lateral radiograph and an MRI scan. Management should consist of
Explanation
The lateral radiograph shows 8 mm of atlantoaxial translation. In the absence of a bony injury, this represents rupture of the transverse atlantal ligament. The MRI scan reveals soft-tissue swelling posterior to the odontoid and a high intensity zone in the atlanto-dens interval consistent with acute injury. These injuries require arthrodesis because nonsurgical measures will not provide stability. Techniques for C1-2 fusion include Gallie, Brooks, or triple wiring. Transarticular screw fixation across the C1-2 articulation provides the most rigid means of fixation and the highest arthrodesis rates but is technically demanding. Anterior C2-3 arthrodesis will not address the level of instability. The normal atlanto-dens interval is 3 mm in an adult and 4 mm in a child.
REFERENCES: Kurz LT: Transverse atlantal ligament insufficiency, in Clark CR (ed):
The Cervical Spine. Philadelphia, PA, Lippincott-Raven, 1998, pp 401-407.
Fielding JW, Cochran GB, Lansing JF III, et al: Tears of the transverse ligament of the atlas:
A clinical and biomechanical study. J Bone Joint Surg Am 1974;56:1683-1691.
REFERENCES: Kurz LT: Transverse atlantal ligament insufficiency, in Clark CR (ed):
The Cervical Spine. Philadelphia, PA, Lippincott-Raven, 1998, pp 401-407.
Fielding JW, Cochran GB, Lansing JF III, et al: Tears of the transverse ligament of the atlas:
A clinical and biomechanical study. J Bone Joint Surg Am 1974;56:1683-1691.
Question 19High Yield
Figure 1 shows the radiograph obtained from a 54-year-old woman with rheumatoid arthritis who has thumb pain and dysfunction. Nonsurgical treatment, including splinting, oral NSAIDs, activity modification, and steroid injections, has failed. What is the most appropriate surgical intervention?
---
---

Explanation
Various options exist to treat thumb CMC arthritis: trapezial resection alone, trapezial resection with ligament suspensionplasty or tendon interposition, trapezial resection with both ligament suspensionplasty and tendon interposition, CMC fusion, and CMC replacement. MCP hyperextension can develop in long-standing CMC arthritis, contributing to CMC instability as well as thumb pain and weakness. In patients with concomitant MCP hyperextension that exceeds 30°,
correction of the deformity of the MCP joint must also be addressed and can be done with MCP capsulodesis, extensor pollicis brevis tendon transfer, or MCP fusion. Fusion of both the thumb CMC and MP joints is not recommended as this would result in marked stiffness and dysfunction.
correction of the deformity of the MCP joint must also be addressed and can be done with MCP capsulodesis, extensor pollicis brevis tendon transfer, or MCP fusion. Fusion of both the thumb CMC and MP joints is not recommended as this would result in marked stiffness and dysfunction.
Question 20High Yield
Which of the following measures has not been shown to decrease rates of injury in healthy children participating in recreational sports:
Explanation
Knee braces have been shown not to reduce injury rates for children for children with sound knees. All other measures have been shown to reduce injury rates.
Question 21High Yield
A 38-year-old man reports right upper extremity pain that radiates from his neck to his anterior arm,dorsoradial forearm, and into the index finger. Examination reveals weakness of the biceps muscle group and loss of his brachioradialis reflex on that side. At which level is he most likely to have a right-sided cervical disk protrusion on an MRI scan?
Explanation
The patient has a typical right C6 radiculopathy based on his history and physical examination. A posterolateral disk protrusion at the C5-C6 level is mostly likely to cause a C6 radiculopathy because the C6 nerve roots exit just above the C6 pedicle and therefore would be compressed by a right-sided C5-C6 disk protrusion. In contrast to the lumbar spine, far lateral disk protrusions are not typically described in the cervical spine.
---
---
Question 22High Yield
The most common cause of damage to femoral vessels is:
Explanation
Damage to the femoral vessels is most commonly due to aberrant retractor placement. Care should be taken to ensure that the retractor tip is placed directly on bone, and that the iliopsoas is not interposed between the retractor tip and bone. Extruded cement, acetabular cup migration, and capsule dissection have also been implicated in damage to the femoral vessels
Question 23High Yield
A 19-year old Division 1 offensive lineman sustains an ankle injury during a game. He has pain with weight-bearing and is unable to return to the game. Figures 1 through 5 are his radiographs taken the next day. What is the best next step?
---
---
---
---
---
---
---
---
---
---





Explanation
The radiographs reveal medial clear space widening and an oblique proximal fibula fracture (best seen on the lateral view overlapping the tibia). This is consistent with an unstable syndesmotic injury. Operative repair of the syndesmosis with reduction and fixation is warranted. Immobilization is the best option for a stable syndesmotic injury. Physical therapy and MRI are not warranted given the findings on the _radiographs._
Question 24High Yield
-What is the best way to determine whether a radial head implant is too thick intraoperatively?
Explanation
No detailed explanation provided for this question.
Question 25High Yield
Slide 1 Slide 2 Slide 3
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 1). The childâs skeletal radiograph survey is also presented (Slide 2 and Slide 3).
The chance of hand involvement in this child is:
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 1). The childâs skeletal radiograph survey is also presented (Slide 2 and Slide 3).
The chance of hand involvement in this child is:
Explanation
The hand is involved in 30% to 80% of cases.
Question 26High Yield
Based on the clinical photograph, radiographs, and biopsy specimen shown in Figures 68a through 68d, what is the most likely diagnosis?



Explanation
**
The patient has gout. Unfortunately, gout may mimic several conditions affecting the small joints of the hand, including infection. The histologic specimen shows negatively birefringent intracellular rods consistent with gout. The histology rules out giant cell tumor and calcium pyrophosphate deposition disease.
The patient has gout. Unfortunately, gout may mimic several conditions affecting the small joints of the hand, including infection. The histologic specimen shows negatively birefringent intracellular rods consistent with gout. The histology rules out giant cell tumor and calcium pyrophosphate deposition disease.
Question 27High Yield
A 40-year-old man has a painful mass on his anterior ankle joint with limited range of motion. A radiograph, MRI scan, a gross specimen, and a hematoxylin/eosin biopsy specimen are shown in Figures 5a through 5d. What is the most likely diagnosis?
Explanation
Synovial chondromatosis results from chondroid metaplasia within the synovium. Male to female ratio is 2:1, with a peak incidence in early adult life. Radiographs can show speckled calcification. Multiple cartilaginous bodies are found loose in the joint and embedded in the synovium. These nodules are composed of cartilage with calcification. Treatment includes synovectomy and removal of loose bodies.
REFERENCES: Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Hocking R, Negrine J: Primary synovial chondromatosis of the subtalar joint affecting two brothers. Foot Ankle Int 2003;24:865-867.
REFERENCES: Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Hocking R, Negrine J: Primary synovial chondromatosis of the subtalar joint affecting two brothers. Foot Ankle Int 2003;24:865-867.
Question 28High Yield
Genetic mutations that may result in the cervical abnormalities noted in the figures generally affect the





Explanation
The figures are characteristic of a child with Klippel-Feil syndrome (congenital cervical spine abnormalities) in association with congenital scoliosis in the upper thoracic spine and a right-sided Sprengel deformity (congenital elevation of the scapula). Sprengel deformity occurs in as many as 30% of children with Klippel-Feil syndrome. Other congenital conditions that are commonly associated with Klippel-Feil, and that should be screened for, include deafness in 30%, genitourinary abnormalities in 25% to 35%, and cardiovascular abnormalities in 4% to 29% of children with Klippel-Feil syndrome.
In Sprengel deformity, there is usually a tether called the omovertebral connection between the abnormally elevated scapula and the spinous processes in the upper thoracic region. This tether is most commonly bony but also may be cartilaginous or fibrous. Although there also may be abnormalities in the ribs, clavicle, or humerus, they are morphologic abnormalities only, not tethers.
Patients with Klippel-Feil syndrome should be discouraged from participating in contact or collision sports if they have a massive fusion of the cervical spine, any involvement of C2, or limited cervical motion. Fusions at 1 or 2 interspaces below C3 and normal cervical motion do not preclude participation in activities. A Sprengel deformity may limit abduction of the shoulder and normal racquet or throwing mechanics, but, in the absence of pain, is not a contraindication to attempted participation.
Klippel-Feil syndrome affects a heterogenous cohort of patients and different inheritance patterns have been seen, including autosomal-dominant and autosomal-recessive types, with varying levels of penetrance. The first human Klippel-Feil syndrome locus was identified on chromosome 8 and is called SGM1. Other candidates for mutations in Klippel-Feil include PAX genes and Notch pathway genes. In general, the involved genes help regulate the formation and segmentation of the vertebrae.
Between days 20 and 30 following conception, the paraxial mesoderm subdivides into segments called somites. As they mature, somites develop into 3 layers called the sclerotome, myotome, and dermatome. The sclerotome undergoes a process of resegmentation during which the caudal section from 1 somite joins with the rostral section of the immediately caudal somite to form the vertebral bodies. It is during the processes of segmentation and resegmentation that the abnormalities leading to Klippel-Feil syndrome occur. Gastrulation refers to the phase early in embryonic development when the single-layered blastula is reorganized into a trilaminar structure with 3 germ layers: the ectoderm, mesoderm, and endoderm. Neurulation refers to the process by which the notochord induces formation of the neural tube from the neural plate, forming the brain and spinal cord.
Figure 55a
Figure 55b
Figure 55c
In Sprengel deformity, there is usually a tether called the omovertebral connection between the abnormally elevated scapula and the spinous processes in the upper thoracic region. This tether is most commonly bony but also may be cartilaginous or fibrous. Although there also may be abnormalities in the ribs, clavicle, or humerus, they are morphologic abnormalities only, not tethers.
Patients with Klippel-Feil syndrome should be discouraged from participating in contact or collision sports if they have a massive fusion of the cervical spine, any involvement of C2, or limited cervical motion. Fusions at 1 or 2 interspaces below C3 and normal cervical motion do not preclude participation in activities. A Sprengel deformity may limit abduction of the shoulder and normal racquet or throwing mechanics, but, in the absence of pain, is not a contraindication to attempted participation.
Klippel-Feil syndrome affects a heterogenous cohort of patients and different inheritance patterns have been seen, including autosomal-dominant and autosomal-recessive types, with varying levels of penetrance. The first human Klippel-Feil syndrome locus was identified on chromosome 8 and is called SGM1. Other candidates for mutations in Klippel-Feil include PAX genes and Notch pathway genes. In general, the involved genes help regulate the formation and segmentation of the vertebrae.
Between days 20 and 30 following conception, the paraxial mesoderm subdivides into segments called somites. As they mature, somites develop into 3 layers called the sclerotome, myotome, and dermatome. The sclerotome undergoes a process of resegmentation during which the caudal section from 1 somite joins with the rostral section of the immediately caudal somite to form the vertebral bodies. It is during the processes of segmentation and resegmentation that the abnormalities leading to Klippel-Feil syndrome occur. Gastrulation refers to the phase early in embryonic development when the single-layered blastula is reorganized into a trilaminar structure with 3 germ layers: the ectoderm, mesoderm, and endoderm. Neurulation refers to the process by which the notochord induces formation of the neural tube from the neural plate, forming the brain and spinal cord.
Figure 55a
Figure 55b
Figure 55c
Question 29High Yield
Removal of both hallucal sesamoids should be reserved as a salvage procedure because of the high incidence of which of the following postoperative complications?
Explanation
Removal of both sesamoids is associated with a high incidence of postoperative hallux valgus and cock-up deformity of the great toe because of weakening of the flexor hallucis brevis tendon. The sesamoids lie within these tendons and require meticulous repair following excision.
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 17-25.
Richardson EG: Hallucal sesamoid pain: Causes and surgical treatment. J Am Acad Orthop Surg 1999;7:270-278.
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 17-25.
Richardson EG: Hallucal sesamoid pain: Causes and surgical treatment. J Am Acad Orthop Surg 1999;7:270-278.
Question 30High Yield
Figure 77 shows the clinical photograph of a 21-year-old male ice hockey player who sustained a blow to the jaw from another player’s hockey stick. Examination reveals an unstable jaw, mild bleeding with exposed bone, and malocclusion. What is the most serious acute complication of this injury?
Explanation
DISCUSSION: The most serious, acute complication of severe maxillofacial trauma is airway obstruction that can result in early death. It is most likely to be associated with multiple mandibular fractures or combined maxillary, mandibular, and nasal fractures as reported by Seyfer and Hansen and Rohrich and Shewmaker.
The mandible suspends the tongue anteriorly. When the mandible is fractured and the patient is supine, the tongue falls posteriorly and obstructs the airway. Soft-tissue swelling around the injured oronasal structures can also result in a loss of airway patency. Endotracheal or nasotracheal intubation is often impossible and a surgical airway may often have to be created to prevent death by asphyxiation. Other injuries that may require immediate attention include head or cervical spine injury and hemorrhage. A cerebrovascular accident is also less common but is associated with injury to the common carotid artery or its branches. Periodontal disease is generally a long-term complication from dental injuries. Hearing loss is not a common complication of dental and facial trauma.
REFERENCES: Seyfer AE, Hansen JE: Facial trauma, in Moore EF, Feliciano DV, Maddox KL (eds): Trauma, ed 5. New York, NY, McGraw-Hill, 2004, pp 423-444.
Rohrich RJ, Shewmake KB: Evolving concepts of craniomaxillofacial fracture management. Clin Plast
Surg 1992;19:1-10.
DISCUSSION: The most serious, acute complication of severe maxillofacial trauma is airway obstruction that can result in early death. It is most likely to be associated with multiple mandibular fractures or combined maxillary, mandibular, and nasal fractures as reported by Seyfer and Hansen and Rohrich and Shewmaker.
The mandible suspends the tongue anteriorly. When the mandible is fractured and the patient is supine, the tongue falls posteriorly and obstructs the airway. Soft-tissue swelling around the injured oronasal structures can also result in a loss of airway patency. Endotracheal or nasotracheal intubation is often impossible and a surgical airway may often have to be created to prevent death by asphyxiation. Other injuries that may require immediate attention include head or cervical spine injury and hemorrhage. A cerebrovascular accident is also less common but is associated with injury to the common carotid artery or its branches. Periodontal disease is generally a long-term complication from dental injuries. Hearing loss is not a common complication of dental and facial trauma.
REFERENCES: Seyfer AE, Hansen JE: Facial trauma, in Moore EF, Feliciano DV, Maddox KL (eds): Trauma, ed 5. New York, NY, McGraw-Hill, 2004, pp 423-444.
Rohrich RJ, Shewmake KB: Evolving concepts of craniomaxillofacial fracture management. Clin Plast
Surg 1992;19:1-10.
Question 31High Yield
A 30-month-old boy underwent open reduction of his right hip to address developmental hip dysplasia. The reduction was performed through an anterior approach, and a shortening femoral osteotomy was not performed. Four months after surgery, hip radiographs reveal absence of ossification of the femoral epiphysis and fragmentation of the ossific nucleus. What is the likely cause of this complication?
Explanation
The incidence of pediatric hip dysplasia is approximately 1 per 100 live births, with hip dislocation present in 1 in 1000 births. Two surgical approaches primarily are used for surgical reduction in the dislocated pediatric hip: the modified medial approach as described by Weinstein and the
anterior Smith-Peterson approach. The Weinstein modification of the Ludloff approach exploits the interval between the pectineus muscle and the femoral neurovascular bundles rather than the interval between the pectineus and the adductor longus and brevis. The modified “bikini” anterior Smith-Peterson approach passes between the sartorius and tensor fascia lata superficially and between the rectus and gluteus medius during deep dissection.
When using the medial approach, the neurovascular bundle is particularly at risk, including the medial circumflex femoral vessels that supply blood to the femoral head ossific nucleus. Damage to this structure increases risk for osteonecrosis of the femoral head. Unlike the anterior approach, the medial approach does not allow for the performance of a capsulorrhaphy, poses higher risk for postprocedure redislocation, and is less useful in children of walking age. Identification of the ligamentum teres during deep dissection assists in localization of the true bony acetabulum.
The anatomic structure primarily at risk during the anterior approach is the lateral femoral cutaneous nerve. Excessive traction or transection of this structure will result in numbness in the proximal lateral thigh. This surgical approach allows for identifying and addressing all potential impediments to reduction: the redundant capsule, hypertrophic labrum, hypertrophic ligamentum teres, pulvinar, iliopsoas tendon, and transverse acetabular ligament. In older children who undergo open reduction with periacetabular osteotomy without a concomitant proximal femoral shortening osteotomy, reduction may be accompanied by increased pressure on the femoral head which, in turn, may result in secondary osteonecrosis of the femoral head.
RECOMMENDED READINGS
1. Karol LA. Developmental dysplasia of the hip. In: Song KM, ed. _Orthopaedic Knowledge Update: Pediatrics 4_. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2011:159-167.
2. [Vitale MG, Skaggs DL. Developmental dysplasia of the hip from six months to four years of age. J Am Acad Orthop Surg. 2001 Nov-Dec;9(6):401-11. Review. PubMed PMID: 11730331. ](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11730331)
3. Weinstein SL, Ponseti IV. Congenital dislocation of the hip. J Bone Joint Surg Am. 1979 Jan;61(1):119-
[24/. PubMed PMID: 759421. ](http://www.ncbi.nlm.nih.gov/pubmed/759421)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/759421)
4. Olszewski DC, Karol LA. The medial Ludloff open reduction in developmental dysplasia of the hip before the age of walking. Operative Techniques in Orthopaedics. 2013;23:109-114.
anterior Smith-Peterson approach. The Weinstein modification of the Ludloff approach exploits the interval between the pectineus muscle and the femoral neurovascular bundles rather than the interval between the pectineus and the adductor longus and brevis. The modified “bikini” anterior Smith-Peterson approach passes between the sartorius and tensor fascia lata superficially and between the rectus and gluteus medius during deep dissection.
When using the medial approach, the neurovascular bundle is particularly at risk, including the medial circumflex femoral vessels that supply blood to the femoral head ossific nucleus. Damage to this structure increases risk for osteonecrosis of the femoral head. Unlike the anterior approach, the medial approach does not allow for the performance of a capsulorrhaphy, poses higher risk for postprocedure redislocation, and is less useful in children of walking age. Identification of the ligamentum teres during deep dissection assists in localization of the true bony acetabulum.
The anatomic structure primarily at risk during the anterior approach is the lateral femoral cutaneous nerve. Excessive traction or transection of this structure will result in numbness in the proximal lateral thigh. This surgical approach allows for identifying and addressing all potential impediments to reduction: the redundant capsule, hypertrophic labrum, hypertrophic ligamentum teres, pulvinar, iliopsoas tendon, and transverse acetabular ligament. In older children who undergo open reduction with periacetabular osteotomy without a concomitant proximal femoral shortening osteotomy, reduction may be accompanied by increased pressure on the femoral head which, in turn, may result in secondary osteonecrosis of the femoral head.
RECOMMENDED READINGS
1. Karol LA. Developmental dysplasia of the hip. In: Song KM, ed. _Orthopaedic Knowledge Update: Pediatrics 4_. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2011:159-167.
2. [Vitale MG, Skaggs DL. Developmental dysplasia of the hip from six months to four years of age. J Am Acad Orthop Surg. 2001 Nov-Dec;9(6):401-11. Review. PubMed PMID: 11730331. ](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11730331)
3. Weinstein SL, Ponseti IV. Congenital dislocation of the hip. J Bone Joint Surg Am. 1979 Jan;61(1):119-
[24/. PubMed PMID: 759421. ](http://www.ncbi.nlm.nih.gov/pubmed/759421)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/759421)
4. Olszewski DC, Karol LA. The medial Ludloff open reduction in developmental dysplasia of the hip before the age of walking. Operative Techniques in Orthopaedics. 2013;23:109-114.
Question 32High Yield
Which of the following nerves is most susceptible to iatrogenic injury during bunion surgery?

Explanation
The dorsomedial cutaneous nerve, which is the terminal branch of the superficial peroneal nerve, is most susceptible to iatrogenic injury, primarily due to the location of surgical incisions. The dorsolateral cutaneous nerve is typically a branch of the
deep peroneal nerve; the medial plantar hallucal nerve is a branch of the medial plantar nerve. The terminal branch of the saphenous nerve provides sensation to the dorsomedial hindfoot.
---
deep peroneal nerve; the medial plantar hallucal nerve is a branch of the medial plantar nerve. The terminal branch of the saphenous nerve provides sensation to the dorsomedial hindfoot.
---
Question 33High Yield
Which of the following tumors rarely metastasizes:
Explanation
Dermatofibrosarcoma protuberans presents as a variably colored, slow-growing nodule involving the subcutaneous tissue. This tumor has a low incidence of metastasis; however, the recurrence rate is high even with wide local excision.
Question 34High Yield
When using antibiotic-laden polymethylmethacrylate (PMMA) beads, the elution characteristics produce which profile?
Explanation
The elution of antibiotics from polymethylmethacrylate beads is characterized by a rapid release during the initial 24 hours, followed by a period during which the release rate quickly decreases and then reaches a steadily declining rate release. Elution can produce very low levels of release by week 5.
RECOMMENDED READINGS
20. [Hake ME, Young H, Hak DJ, Stahel PF, Hammerberg EM, Mauffrey C. Local antibiotic therapy strategies in orthopaedic trauma: Practical tips and tricks and review of the literature. Injury. 2015 Aug;46(8):1447-56. doi: 10.1016/j.injury.2015.05.008. Epub 2015 May 14. Review. PubMed PMID: 26007616. ](http://www.ncbi.nlm.nih.gov/pubmed/26007616)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26007616)
21. [Anagnostakos K, Wilmes P, Schmitt E, Kelm J. Elution of gentamicin and vancomycin from polymethylmethacrylate beads and hip spacers in vivo. Acta Orthop. 2009 Apr;80(2):193-7. doi: 10.3109/17453670902884700. PubMed PMID: 19404802. ](http://www.ncbi.nlm.nih.gov/pubmed/19404802)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19404802)
22. [Penner MJ, Duncan CP, Masri BA. The in vitro elution characteristics of antibiotic-loaded CMW and Palacos-R bone cements. J Arthroplasty. 1999 Feb;14(2):209-14. ](http://www.ncbi.nlm.nih.gov/pubmed/10065729)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10065729)
RESPONSES FOR QUESTIONS 89 THROUGH 96
1. Humeral head resurfacing/shoulder hemiarthroplasty
2. Anatomic total shoulder arthroplasty (TSA)
3. Reverse total shoulder arthroplasty (rTSA)
4. Rotator cuff repair
5. Open reduction and internal fixation (ORIF)
Which intervention listed above is most appropriate to address each scenario described below? When chronic conditions are described, nonsurgical interventions such as physical therapy, anti-inflammatory medications, and corticosteroid injections have been exhausted.
RECOMMENDED READINGS
20. [Hake ME, Young H, Hak DJ, Stahel PF, Hammerberg EM, Mauffrey C. Local antibiotic therapy strategies in orthopaedic trauma: Practical tips and tricks and review of the literature. Injury. 2015 Aug;46(8):1447-56. doi: 10.1016/j.injury.2015.05.008. Epub 2015 May 14. Review. PubMed PMID: 26007616. ](http://www.ncbi.nlm.nih.gov/pubmed/26007616)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26007616)
21. [Anagnostakos K, Wilmes P, Schmitt E, Kelm J. Elution of gentamicin and vancomycin from polymethylmethacrylate beads and hip spacers in vivo. Acta Orthop. 2009 Apr;80(2):193-7. doi: 10.3109/17453670902884700. PubMed PMID: 19404802. ](http://www.ncbi.nlm.nih.gov/pubmed/19404802)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19404802)
22. [Penner MJ, Duncan CP, Masri BA. The in vitro elution characteristics of antibiotic-loaded CMW and Palacos-R bone cements. J Arthroplasty. 1999 Feb;14(2):209-14. ](http://www.ncbi.nlm.nih.gov/pubmed/10065729)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10065729)
RESPONSES FOR QUESTIONS 89 THROUGH 96
1. Humeral head resurfacing/shoulder hemiarthroplasty
2. Anatomic total shoulder arthroplasty (TSA)
3. Reverse total shoulder arthroplasty (rTSA)
4. Rotator cuff repair
5. Open reduction and internal fixation (ORIF)
Which intervention listed above is most appropriate to address each scenario described below? When chronic conditions are described, nonsurgical interventions such as physical therapy, anti-inflammatory medications, and corticosteroid injections have been exhausted.
Question 35High Yield
Figures 32a and 32b are the CT and MR image of a man who undergoes fusion for his degenerative spondylolisthesis. He wakes up with a foot drop. Which structure has most likely been injured?

Explanation
After exiting the L5-S1 neuroforamen, the L5 nerve root lies anterior to the sacral ala. There, if S1 pedicle screws are inadvertently directed laterally toward the ala rather than medially toward the sacral promontory, the L5 nerve root is endangered.
The iliac vein and artery lie more ventral than the L5 nerve root, which is draped closely to the sacral ala. The S1 nerve root exits inferior to the S1 sacral ala and is seen medial to the S1 pedicle on the MR axial image provided. On the CT scan the pedicle screw is aiming medial to lateral and is penetrating several millimeters outside the bone. Although an injury to the peroneal division of the sciatic nerve could result in a foot drop, this is not the most likely cause in this scenario and it lies more peripherally.
RECOMMENDED READINGS
7. [Mirkovic S, Abitbol JJ, Steinman J, Edwards CC, Schaffler M, Massie J, Garfin SR. Anatomic consideration for sacral screw placement. Spine (Phila Pa 1976). 1991 Jun;16(6 Suppl):S289-94. PubMed PMID: 1862427. ](http://www.ncbi.nlm.nih.gov/pubmed/1862427)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1862427)
8. [Santos ER, Rosner MK, Perra JH, Polly DW Jr. Spinopelvic fixation in deformity: a review. Neurosurg Clin N Am. 2007 Apr;18(2):373-84. Review. PubMed PMID: 17556140. ](http://www.ncbi.nlm.nih.gov/pubmed/17556140)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17556140)
The iliac vein and artery lie more ventral than the L5 nerve root, which is draped closely to the sacral ala. The S1 nerve root exits inferior to the S1 sacral ala and is seen medial to the S1 pedicle on the MR axial image provided. On the CT scan the pedicle screw is aiming medial to lateral and is penetrating several millimeters outside the bone. Although an injury to the peroneal division of the sciatic nerve could result in a foot drop, this is not the most likely cause in this scenario and it lies more peripherally.
RECOMMENDED READINGS
7. [Mirkovic S, Abitbol JJ, Steinman J, Edwards CC, Schaffler M, Massie J, Garfin SR. Anatomic consideration for sacral screw placement. Spine (Phila Pa 1976). 1991 Jun;16(6 Suppl):S289-94. PubMed PMID: 1862427. ](http://www.ncbi.nlm.nih.gov/pubmed/1862427)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1862427)
8. [Santos ER, Rosner MK, Perra JH, Polly DW Jr. Spinopelvic fixation in deformity: a review. Neurosurg Clin N Am. 2007 Apr;18(2):373-84. Review. PubMed PMID: 17556140. ](http://www.ncbi.nlm.nih.gov/pubmed/17556140)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17556140)
Question 36High Yield
Scoliosis in cleidocranial dysplasia is frequently associated with which of the following conditions:
Explanation
Scoliosis with cleidocranial dysplasia (C C D) is frequently associated with syringomyelia.
C ervical instability is rare in C C D. Spondylolisthesis is rare in C C D. Spinal stenosis is rare in C C D.
Spinal decompensation is rare in C C D.
C ervical instability is rare in C C D. Spondylolisthesis is rare in C C D. Spinal stenosis is rare in C C D.
Spinal decompensation is rare in C C D.
Question 37High Yield
A 42-year-old woman sustained an open grade 3B tibial shaft fracture with a severe degloving injury involving the anterior and lateral compartments 1 year ago.
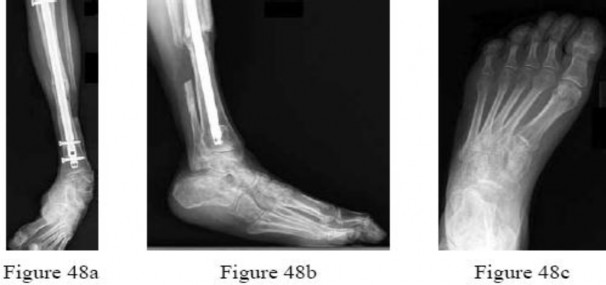
She underwent multiple débridements,definitive fracture treatment, and flap coverage. She now reports that she has difficulty ambulating.Examination includes a 20° equinovarus contracture, 2+ dorsiflexion, 2+ eversion, 5+ inversion, and 5+ plantar flexion strength. She has a supple forefoot and intact sensation throughout. Figures 48a through 48c are current weight-bearing radiographs. Attempted surgical correction should include Achilles lengthening, calcaneal osteotomy, and
---
She underwent multiple débridements,definitive fracture treatment, and flap coverage. She now reports that she has difficulty ambulating.Examination includes a 20° equinovarus contracture, 2+ dorsiflexion, 2+ eversion, 5+ inversion, and 5+ plantar flexion strength. She has a supple forefoot and intact sensation throughout. Figures 48a through 48c are current weight-bearing radiographs. Attempted surgical correction should include Achilles lengthening, calcaneal osteotomy, and
---
Explanation
The patient has developed an equinovarus contracture from overpull of the posterior tibial tendon, presumably due to the degloving injury and lack of protective splinting. In this instance, the patient is best treated with an Achilles lengthening, lateralizing calcaneal osteotomy, and posterior tibial tendon transfer. Flexor hallucis longus to peroneal transfer will not restore dorsiflexion. Ankle arthrodesis would allow deformity correction through the ankle joint but does not address the remainder of the foot,such that the patient would likely have trouble clearing the floor during the swing phase of gait. A first metatarsal osteotomy is indicated in the instance of a forefoot-driven cavus foot deformity. A split anterior tibial tendon transfer is indicated for correction of ankle and hindfoot varus contractures, and requires an intact and functional anterior tibial tendon, making it contraindicated in this instance.
Question 38High Yield
In classic hemophilia, a natural factor-VIII level of less than what percentage will lead to severe bleeding and complications:
Explanation
A surprisingly small amount of circulating factor-VIII (approximately 5%) is necessary to protect a patient from severe bleeding complications.
Question 39High Yield
Which of the following statements best characterizes the natural history of metatarsus adductus in a newborn:
Explanation
Virtually all patients with metatarsus adductus will improve with time in the absence of active treatment.
C asts are not needed for the majority of cases because spontaneous improvement is by far the most common outcome. Reverse last shoes are not needed in the majority of patients with metatarsus adductus.
Most patients will not need surgery.
Equinus of the hindfoot is not part of the pathology in metatarsus adductus.
C asts are not needed for the majority of cases because spontaneous improvement is by far the most common outcome. Reverse last shoes are not needed in the majority of patients with metatarsus adductus.
Most patients will not need surgery.
Equinus of the hindfoot is not part of the pathology in metatarsus adductus.
Question 40High Yield
The main advantage of multicenter studies in analyzing total hip arthroplasty is:
Explanation
The main advantage of multicenter studies - although they are time-consuming, expensive, and often frustrating - is obtaining large numbers of patients in a relatively short time. This is important when examining statistical differences between varying results
Question 41High Yield
A 17-year-old patient presents with pain in the second toe. Pain becomes worse with exercise and has been present for 6 months. On examination, swelling is present around the metatarsophalangeal joint, and pain is present over the joint and upon squeezing the forefoot. Radiographic evaluation demonstrates a lucency in the second metatarsal head. The most likely cause of this condition is:
Explanation
This patient has the typical features of Freibergâs osteochondrosis of the second metatarsal head. There is swelling present, which is not noted in association with a neuroma, even though the clinical findings may be similar. Synovitis is common but not associated with radiographic changes.
Question 42High Yield
Figures 9a and 9b are the radiographs of a 32-year-old woman who has right foot pain after falling down a few steps. For the best long-term outcome, initial treatment should include which of the following?
---
---


Explanation
The radiographs show a displaced Lisfranc injury. The outcome of treatment is dependent on achieving an anatomic reduction and stabilization, which is only possible with primary ORIF. Some studies indicate primary fusion may provide superior short-term results compared with ORIF. Closed treatment (reduction with casting or splinting) will not achieve or maintain the reduction, whereas delayed treatment by secondary fusion after arthritis occurs yields inferior outcomes to primary ORIF.
---
---
Question 43High Yield
Figure 16 shows the lateral radiograph of a patient who is scheduled to undergo an anterior cruciate ligament (ACL) reconstruction. If the graft is tensioned at 20° of flexion and the femoral tunnel is created by passing a reamer over the guide wire marked “A,” the resulting ligament reconstruction will excessively**
Explanation
If the femoral tunnel is created using guide wire A, it will be too far anterior in the intercondylar notch. The distance between a central tibial insertion for the ACL and an anterior femoral tunnel will progressively increase as the knee is flexed. Therefore, if the graft is tensioned near extension, the ligament will excessively tighten as the knee flexes past 90°. This will result in restricted knee flexion or failure of the graft as full flexion is gained. There will be little effect on the ligament as it extends from 20° to 0° of flexion. If the graft is tensioned in significant flexion (greater than 60°), it will be excessively loose as the knee fully extends.
REFERENCES: Daniel DM, Fritschy D: Anterior cruciate ligament injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 1994, pp 1313-1360.
Larson RL, Tailon M: Anterior cruciate ligament insufficiency: Principles of treatment. J Am Acad Orthop Surg 1994;2:26-35.
REFERENCES: Daniel DM, Fritschy D: Anterior cruciate ligament injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 1994, pp 1313-1360.
Larson RL, Tailon M: Anterior cruciate ligament insufficiency: Principles of treatment. J Am Acad Orthop Surg 1994;2:26-35.
Question 44High Yield
A 63-year-old right-hand dominant woman has a history of gradually progressive atraumatic right shoulder pain. She describes a constant nagging pain that radiates to her deltoid insertion and difficulty with overhead activities. Her examination and imaging studies confirm a rotator cuff tear. What is the mostly likely initiating anatomic location of her tear?
Explanation
Fundamental to understanding the pathogenesis of rotator cuff tears is an appreciation of the likely initiation site of the disease process. Although authors initially postulated that rotator cuff tears originated in the anterior margin of the supraspinatus tendon near the biceps tendon, recent research has challenged this notion. Kim and associates analyzed 360 full-thickness or partial-thickness rotator cuff tears using ultrasonograms. They separated stratified tears based on their anteroposterior size and whether they were partial- or full-thickness tears. The mean width and length of tear size was 16.3 mm and 17 mm, respectively. Histograms showed that the most common tear location for all tears regardless of size was approximately 15 mm posterior to the biceps tendon. This corresponds to the center of the rotator crescent initially described by Burkhart and associates. This location is described as being more susceptible to degeneration secondary to its diminished vascular supply and mechanical properties. The rotator cable is an arch-shaped thick bundle of fibers that is thought to shield the crescent from stress.
Question 45High Yield
Which of the following molecules play an important role in cartilage hypertrophy during growth plate development and ossification in fracture healing:
Explanation
Important concepts to remember regarding signaling proteins include:
Indian hedgehog (IHH) and core binding factor alpha 1 (Cbfa1) influence embryoniCbone formation and fracture healing. Vascular endothelial growth factor (VEGF) plays a role in cartilage hypertrophy at the growth plate and during fracture healing.
Transforming growth factor-beta (TGF-B) and platelet derived growth factor (PDGF) are found in early fracture hematoma, and these factors modulate cell proliferation and differentiation.
Bone morphogenetiCprotein and interleukin 1 and 6 are expressed during cartilage formation. Correct Answer: Vascular endothelial growth factor (VEGF)
Indian hedgehog (IHH) and core binding factor alpha 1 (Cbfa1) influence embryoniCbone formation and fracture healing. Vascular endothelial growth factor (VEGF) plays a role in cartilage hypertrophy at the growth plate and during fracture healing.
Transforming growth factor-beta (TGF-B) and platelet derived growth factor (PDGF) are found in early fracture hematoma, and these factors modulate cell proliferation and differentiation.
Bone morphogenetiCprotein and interleukin 1 and 6 are expressed during cartilage formation. Correct Answer: Vascular endothelial growth factor (VEGF)
Question 46High Yield
A 25-year-old man injured his dominant shoulder after falling on his outstretched arm 4 months ago. Examination reveals that he cannot lift his arm above 90 degrees, and he has pronounced medial scapular winging. Management should consist of
Explanation
Serratus anterior palsy or long thoracic nerve palsy is usually caused by traction injury to the nerve, blunt injury, or iatrogenic injury. The palsy results in winging of the scapula and medial rotation of the inferior pole of the scapula. A patient with this injury will usually recover in 12 to 18 months. Initial treatment should include observation and shoulder strengthening exercises. Nerve exploration with repair has not proven beneficial in changing the outcome. Many orthopaedic surgeons favor using a split pectoralis major transfer for symptomatic patients. Electrodiagnostic studies are helpful in confirming the diagnosis.
REFERENCES: Post M: Pectoralis major transfer for winging of the scapula. J Shoulder Elbow Surg 1995;4:1-9.
Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
REFERENCES: Post M: Pectoralis major transfer for winging of the scapula. J Shoulder Elbow Surg 1995;4:1-9.
Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 47High Yield
The operative report of a recent patient incorrectly documents the timing of peri-operative antibiotic administration. How should the
**medical record be legally altered?**
**medical record be legally altered?**
Explanation
**
It is illegal to alter the medical record under any circumstance. If a documentation error has occurred, you may addend the medical record by identifying the error and noting the correction.
The review article by Bal discusses medical practice and highlights the four legal elements that must be proven in litigation: (1) a professional duty owed to the patient; (2) breach of such duty; (3) injury caused by the breach; and (4) resulting damages.
It is illegal to alter the medical record under any circumstance. If a documentation error has occurred, you may addend the medical record by identifying the error and noting the correction.
The review article by Bal discusses medical practice and highlights the four legal elements that must be proven in litigation: (1) a professional duty owed to the patient; (2) breach of such duty; (3) injury caused by the breach; and (4) resulting damages.
Question 48High Yield
A 30-year-old woman sustains a transverse amputation of the distal phalanx of the index finger, leaving exposed bone. What is the most appropriate management of the soft-tissue defect?
Explanation
V-Y advancement flaps are ideal for fingertip amputations that are transverse or dorsal oblique in nature. Healing by secondary intention is contraindicated with exposed bone. Shortening of exposed bone to allow primary skin closure is a possible alternative, as long as significant shortening of the index finger is avoided. A Moberg flap is useful only for distal amputations of the thumb. The first dorsal metacarpal artery-island pedicled flap uses tissue from the dorsum of the proximal index finger, and is typically used to resurface defects of
the thumb.
REFERENCES: Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Atasoy E, Ioakimidis E, Kasdan ML, et al: Reconstruction of the amputated fingertip with a triangular volar flap: A new surgical procedure. J Bone Joint Surg Am 1970;52:921-926.
the thumb.
REFERENCES: Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Atasoy E, Ioakimidis E, Kasdan ML, et al: Reconstruction of the amputated fingertip with a triangular volar flap: A new surgical procedure. J Bone Joint Surg Am 1970;52:921-926.
Question 49High Yield
Which of the following describes the inheritance pattern of Gaucher's disease:
Explanation
Structural defects are usually transmitted by an autosomal-dominant pattern. In contrast, with metabolic or enzyme deficiencies, the condition is usually transmitted in an autosomal-recessive pattern.
Remember the major autosomal-recessive conditions: Sickle cell disease
Osteogenesis imperfecta (Types II, III)
Hypophosphatasia Homocystinuria Gaucher's disease
Remember the major autosomal-recessive conditions: Sickle cell disease
Osteogenesis imperfecta (Types II, III)
Hypophosphatasia Homocystinuria Gaucher's disease
Question 50High Yield
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. Treatment should include
---
---
---
---
---
---
---
---
---
---





Explanation
The MR images show a tear through a discoid lateral meniscus. A discoid meniscus is caused by a failure of apoptosis during development in utero and is considered a congenital abnormality. Discoid menisci are prone to tearing and can be caused by minimal trauma. There is no known genetic cause for this condition. Radiographic findings that may be present in the setting of a discoid meniscus include lateral joint space widening, squaring of the lateral femoral condyle, and cupping of the lateral tibial plateau. Contralateral discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment _of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair._
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon