Operative Management of Muscular Dystrophy: A Comprehensive Orthopaedic Guide
Key Takeaway
Muscular dystrophies encompass a heterogeneous group of hereditary myopathies characterized by progressive skeletal muscle degeneration. Orthopaedic intervention is paramount for prolonging functional ambulation and managing contractures. This guide details the pathophysiology, clinical evaluation, and operative management of Duchenne muscular dystrophy, including percutaneous contracture releases and posterior tibial tendon transfers, providing orthopaedic surgeons with evidence-based protocols to optimize patient outcomes and quality of life.
MUSCULAR DYSTROPHY: PATHOPHYSIOLOGY AND CLASSIFICATION
The muscular dystrophies represent a heterogeneous group of hereditary disorders affecting skeletal muscle, characterized by progressive myofiber degeneration, fibrofatty replacement, and profound associated weakness. The genetic transmission and phenotypic expression vary significantly across the spectrum of these myopathies.
The X-linked dystrophies are the most prevalent and clinically significant, encompassing Duchenne muscular dystrophy (DMD), Becker muscular dystrophy (BMD), and Emery-Dreifuss muscular dystrophy. Autosomal recessive variants, notably limb-girdle muscular dystrophy and congenital muscular dystrophy, represent the next most common cohort. Conversely, facioscapulohumeral muscular dystrophy (FSHD) is inherited as an autosomal dominant trait and presents with a distinct pattern of regional weakness.
Duchenne Muscular Dystrophy (DMD)
Duchenne muscular dystrophy is a sex-linked recessive inherited trait, predominantly affecting males, though it may manifest in females with Turner syndrome (45,X0) or skewed X-chromosome inactivation. Female carriers are typically asymptomatic but may exhibit mild manifestations. The incidence is approximately 1 in 3,500 live male births. While 70% of cases have a documented family history, approximately 30% arise from spontaneous de novo mutations.
The fundamental etiology of DMD is a mutation in the Xp21 region of the X chromosome. This locus encodes dystrophin, a massive 400-kd structural protein. Dystrophin is a critical component of the dystrophin-glycoprotein complex (DGC), which anchors the intracellular cytoskeleton (F-actin) to the extracellular matrix, thereby stabilizing the sarcolemma during muscle contraction.
In DMD, the total absence of functional dystrophin leads to sarcolemmal fragility, calcium influx, protease activation, and relentless transcellular muscle degeneration.
CLINICAL PRESENTATION AND DIAGNOSIS
Children with DMD typically achieve early motor milestones within normal timeframes; however, independent ambulation is frequently delayed. The disease usually becomes clinically evident between 3 and 6 years of age. Early signs include a tendency toward toe-walking, frequent falls, and difficulty ascending stairs.
Physical Examination
The pattern of muscular weakness in DMD is highly predictable, progressing from proximal to distal.
- Lower Extremity and Pelvic Girdle: Examination reveals early weakness of the gluteus maximus and medius. This proximal weakness manifests as a widely based, lordotic stance and a waddling Trendelenburg gait.
- Gower Sign: The hallmark of proximal lower extremity weakness is the Gower sign. When attempting to rise from the floor, the child must use their upper extremities to "walk up" their own thighs to achieve an upright posture.
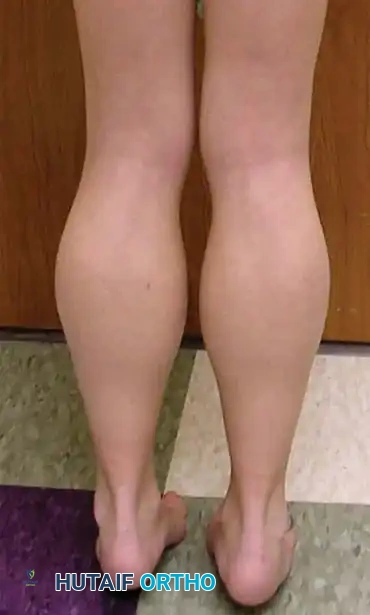
- Calf Pseudohypertrophy: The calf muscles (gastrocnemius and soleus) appear enlarged and firm. This is not true muscle hypertrophy but rather pseudohypertrophy caused by the extensive infiltration of degenerating muscle tissue by fat and fibrosis, giving the calves a characteristic "hard rubber" consistency on palpation.
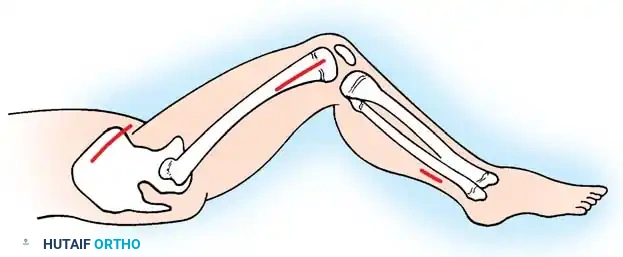
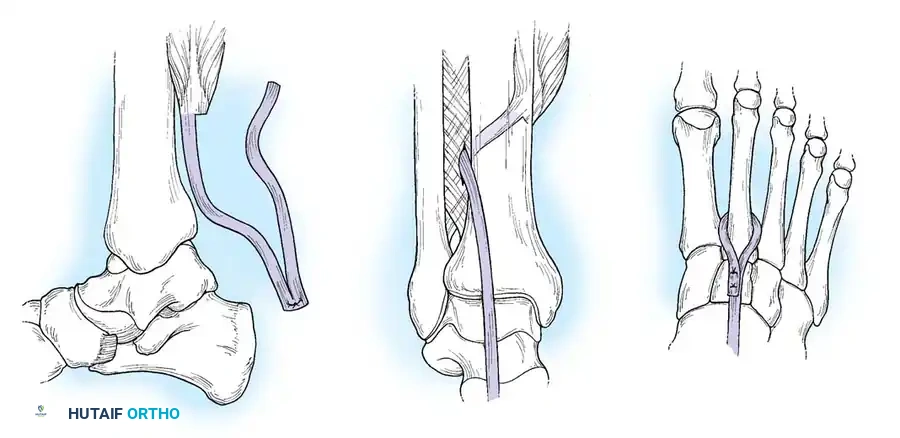
- Foot and Ankle Deformities: The extrinsic muscles of the foot and ankle retain strength longer than the proximal hip and knee musculature. Specifically, the tibialis posterior muscle retains its strength for the longest duration. The unopposed pull of the tibialis posterior, combined with progressive Achilles contracture, predictably drives the foot into a rigid equinovarus deformity.
- Upper Extremity and Shoulder Girdle: Weakness of the shoulder girdle is demonstrated by the Meryon sign. When the examiner attempts to lift the child by encircling their chest under the axillae, the child's arms passively abduct due to severe shoulder depressor and adductor weakness, causing the child to "slip through" the examiner's hands.
- Contractures: As the disease progresses, the Thomas test will reveal fixed hip flexion contractures, and the Ober test will demonstrate abduction contractures of the hip (iliotibial band tightness).
Diagnostic Modalities
The diagnosis is often clinically suspected by age 5. Laboratory analysis reveals dramatically elevated serum creatine kinase (CK) levels, typically 50 to 100 times the upper limit of normal, reflecting massive myonecrosis.
Definitive diagnosis is confirmed via DNA analysis of peripheral blood lymphocytes to identify the specific Xp21 mutation. If genetic testing is indeterminate, a muscle biopsy is indicated. Histological examination reveals extreme variation in muscle fiber size, centralized internal nuclei, split fibers, concurrent degenerating and regenerating fibers, and massive fibrofatty tissue deposition. Immunohistochemical staining for dystrophin will confirm its complete absence in DMD, differentiating it from BMD (where dystrophin is altered or reduced).
MEDICAL MANAGEMENT
The cornerstone of medical therapy involves corticosteroids (prednisone and deflazacort). Evidence demonstrates that steroid therapy preserves muscle strength, prolongs independent ambulation by up to 2 to 3 years, and significantly slows the progression of neuromuscular scoliosis.
⚠️ Clinical Warning: Corticosteroid Complications
While highly beneficial, chronic steroid use induces significant morbidity, including profound weight gain, myopathy, and severe osteopenia. This osteopenia drastically increases the risk of pathological fractures in the long bones and spine, and severely compromises bone purchase during posterior spinal instrumentation for scoliosis.
Investigational therapies, including exon-skipping drugs, gene therapy, and stem cell transfers, are rapidly evolving but remain adjuncts to standard orthopaedic and medical care.
ORTHOPAEDIC TREATMENT PRINCIPLES
The primary orthopaedic objective in DMD is the maintenance of functional ambulation for as long as physiologically possible. Prolonging ambulation delays the onset of severe joint contractures, preserves respiratory function, and delays the rapid progression of scoliosis that inevitably follows wheelchair confinement.

Between the ages of 8 and 14 years (median 10 years), patients typically develop a sensation of "locking" in their joints due to progressive contractures. Lower extremity contractures must be managed aggressively. It is exponentially easier to keep a patient walking than to rehabilitate them back to ambulation once they have ceased.
Surgical Philosophies
Three distinct approaches dictate the timing of surgical intervention:
- Ambulatory Approach (Current Standard): Surgery is performed while the patient is still independently ambulatory, typically just before a significant decline in walking ability. Rideau advocated for early aggressive surgery when contractures first appear, muscle strength plateaus (around age 5-6), and the child struggles to maintain an upright posture with feet together. The goal is to prevent the deterioration of the Gower maneuver time.
- Rehabilitative Approach: Surgery is delayed until the patient has lost the ability to walk, with the goal of resuming limited household ambulation using knee-ankle-foot orthoses (KAFOs).
- Palliative Approach: Intervention is reserved for non-ambulatory patients to correct severe contractures that interfere with wheelchair positioning, hygiene, or shoe wear.
💡 Biomechanical Pearl: The Role of Mild Equinus
Do not over-lengthen the Achilles tendon. A mild equinus contracture is biomechanically advantageous in DMD. It forces the ground reaction force vector anterior to the knee joint during the stance phase, creating an extension moment that prevents the knee from buckling in the presence of profound quadriceps weakness.
If surgery is indicated, hip, knee, and foot contractures should be released simultaneously under a single anesthetic to minimize downtime. Percutaneous techniques are preferred to minimize tissue trauma.
SURGICAL TECHNIQUES FOR LOWER EXTREMITY CONTRACTURES
Preoperative Positioning and Preparation
Proper positioning is critical for accessing multiple release sites simultaneously.
Technique 32-3: Percutaneous Release of Hip Flexion/Abduction and Achilles Contractures (Green)
This minimally invasive technique allows for rapid rehabilitation and immediate postoperative mobilization.
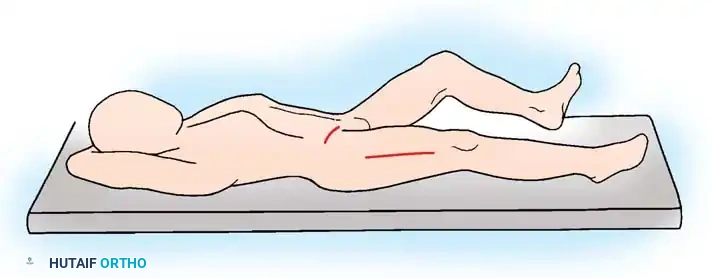
- Positioning: Place the child supine on the operating table. Prepare and drape both lower extremities circumferentially from the iliac crests to the toes.
- Tensioning the Tissues: First flex, then extend the hip to be released, holding the hip in adduction to place maximal tension on the contracted abductors and flexors. Keep the contralateral hip in maximal flexion to flatten the lumbar lordosis and stabilize the pelvis.
- Incision: Insert a No. 15 blade percutaneously just medial and distal to the anterior superior iliac spine (ASIS).
- Muscle Release:
- Release the sartorius muscle first.
- Release the tensor fasciae latae (TFL). Push the knife laterally and subcutaneously—remaining deep to the dermis—to transect the TFL completely.
- Return the blade to the original insertion point and advance it deeper to release the direct head of the rectus femoris.
- Surgical Pitfall: Strictly avoid medial dissection to protect the femoral neurovascular bundle, and be mindful of the lateral femoral cutaneous nerve near the ASIS.
- Distal Fascia Lata Release: Approximately 3 to 4 cm proximal to the superior pole of the patella, percutaneously release the iliotibial band/fascia lata laterally through a stab incision. Advance the blade medially toward the femur to completely release the lateral intermuscular septum.
- Achilles Tenotomy: Perform a percutaneous sliding or complete release of the Achilles tendon, depending on the severity of the equinus.
- Immobilization: Apply well-padded long leg casts with the knees in extension and the feet in a neutral plantigrade position. Ensure meticulous padding over the heels and fibular heads to prevent pressure necrosis.
The Rideau Technique (Open Approach)
Rideau et al. described a more extensive open procedure for severe, recalcitrant contractures. This involves open release of the hip flexors, lateral thigh structures, and formal excision of a segment of the iliotibial band and lateral intermuscular septum to prevent recurrence.
Technique 32-4: Transfer of the Posterior Tibial Tendon to the Dorsum of the Foot (Greene)
In patients with a rigid equinovarus deformity driven by the marked overpull of the tibialis posterior, simple Achilles lengthening is insufficient. Greene demonstrated that transferring the posterior tibial tendon (PTT) to the dorsum of the foot (middle cuneiform) yields superior long-term results, maintaining a plantigrade foot even after the patient becomes wheelchair-bound.
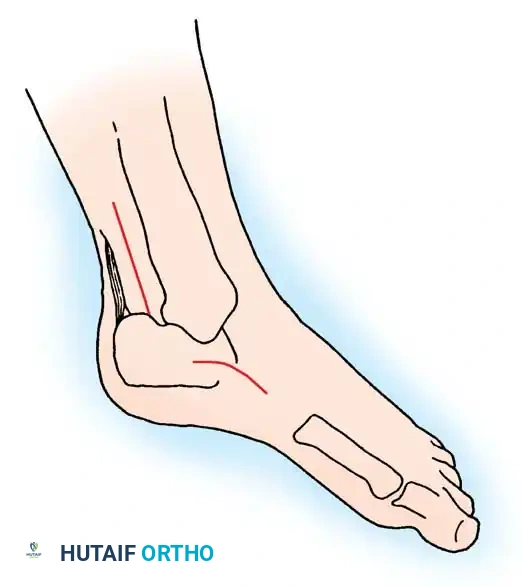
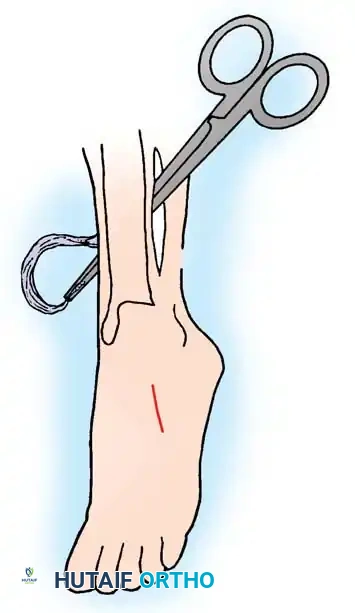
- Medial Incision (Tendon Harvest): Place the patient supine. Apply a thigh tourniquet. Make a 3 cm longitudinal incision on the medial aspect of the foot, starting at the neck of the talus and extending distally to the navicular tuberosity.
- Tendon Release: Open the PTT sheath from the distal extent of the flexor retinaculum to the navicular. Detach the tendon from its multiple bony insertions, preserving maximum length. Tag the distal end with a locking Krackow suture.
- Posteromedial Incision: Make a second vertical incision (6 to 8 cm) between the Achilles tendon and the posteromedial border of the distal tibia. (The Achilles tendon can be lengthened through this same window if required).
- Tendon Delivery: Incise the proximal PTT sheath and pull the detached distal tendon into this second wound.
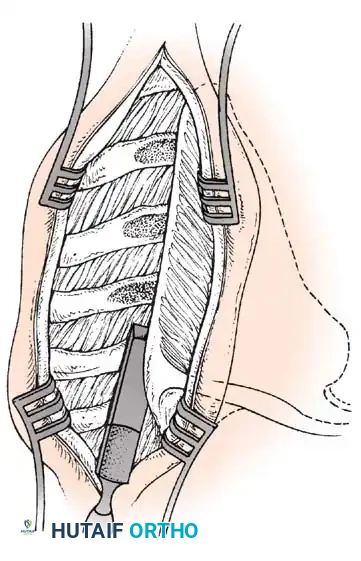
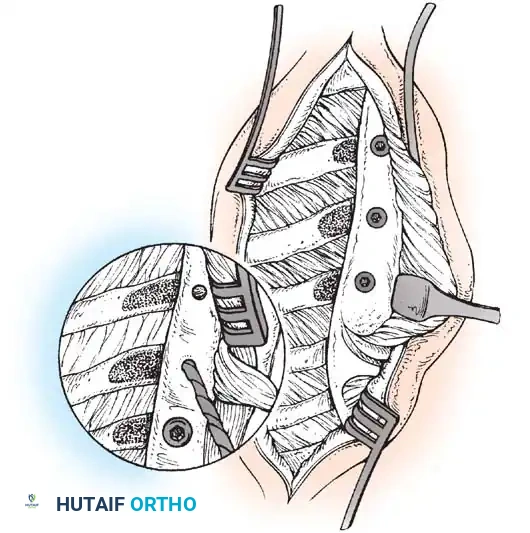
- Anterolateral Incision: Make a third incision (6 cm) lateral to the anterior tibial crest, extending down to the superior extensor retinaculum.
- Interosseous Membrane Window: Incise the anterior compartment fascia. Retract the tibialis anterior tendon laterally. Carefully expose the interosseous membrane adjacent to the tibia. Exise a 3 cm vertical window in the membrane. Enlarge this opening with proximal and distal horizontal cuts.
- Tendon Routing: Pass a large curved clamp from the anterior compartment, through the interosseous window, into the posteromedial wound.
- Surgical Pitfall: Keep the clamp intimately applied to the posterior tibial cortex to avoid catastrophic injury to the peroneal vessels.
- Grasp the tagged PTT and pull it through the interosseous window into the anterior compartment. Inspect the tendon through the posterior wound to ensure it is not twisted or ensnaring the flexor digitorum longus.
- Dorsal Foot Incision: Make a fourth incision (3 cm) over the dorsum of the foot, centered over the middle cuneiform.
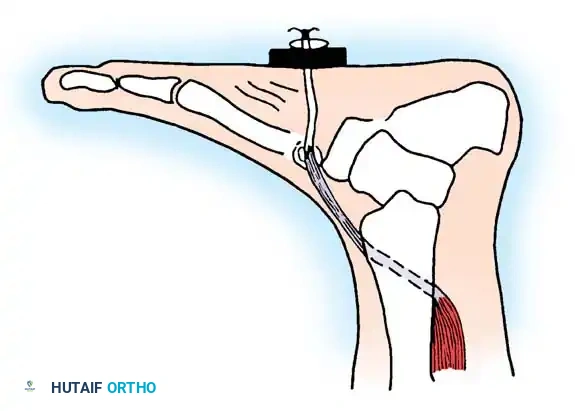
- Bony Preparation: Incise the periosteum of the middle cuneiform. Drill a 5 to 8 mm osseous tunnel directly through the center of the bone, from dorsal to plantar.
- Tendon Fixation: Pass a tendon passer subcutaneously from the anterior leg incision to the dorsal foot incision. Pull the PTT through this subcutaneous tunnel. Pass the suture limbs through the cuneiform drill hole, exiting the plantar aspect of the foot. Tension the tendon with the foot held in neutral dorsiflexion and tie the sutures over a padded button on the plantar surface.
- Closure: Deflate the tourniquet, achieve meticulous hemostasis, and close all wounds in layers. Apply a short leg cast.
Postoperative Rehabilitation Protocol
Prolonged immobilization is the enemy of the dystrophic muscle. Disuse atrophy occurs rapidly and is often irreversible.
* Immediate Mobilization: Patients must be mobilized immediately postoperatively. If tolerated, standing and taking a few steps are encouraged on postoperative day one.
* Orthoses: Casts are bivalved as soon as acute swelling subsides. Custom-molded bilateral polypropylene KAFOs or AFOs are fitted immediately.
* Discharge: Patients are discharged only when they can safely perform transfers and ambulate independently with a walker or crutches.
FACIOSCAPULOHUMERAL MUSCULAR DYSTROPHY (FSHD)
While DMD dominates the pediatric orthopaedic landscape, Facioscapulohumeral Muscular Dystrophy (FSHD) is a critical autosomal dominant myopathy that frequently presents to the adult reconstructive or shoulder surgeon.
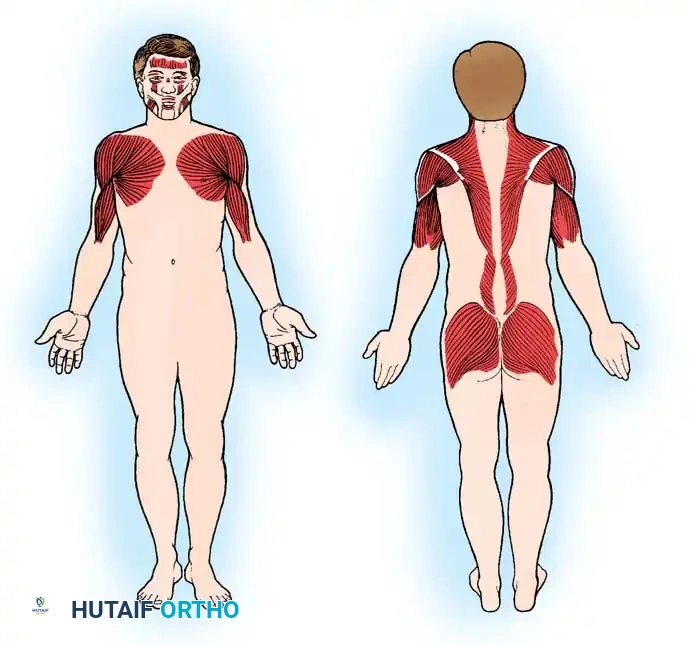
FSHD is characterized by a highly specific topographical progression of weakness, initially affecting the facial musculature, followed by the periscapular stabilizers, and eventually the humeral and anterior leg muscles.
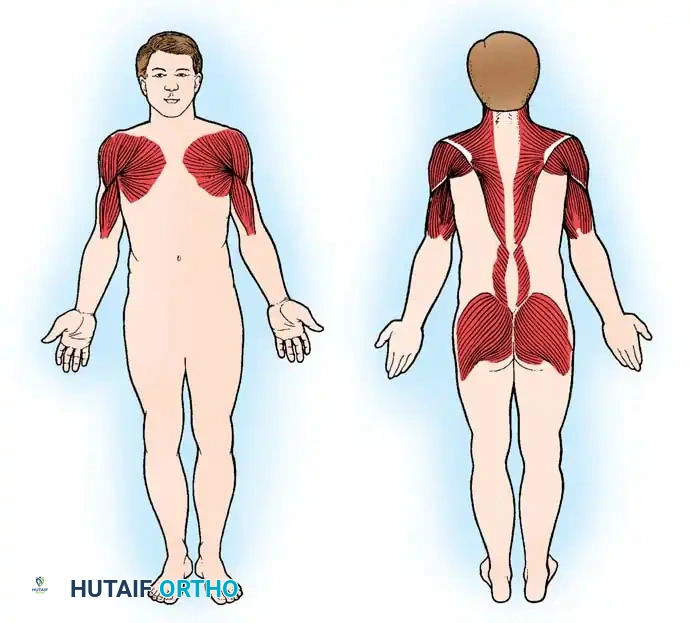
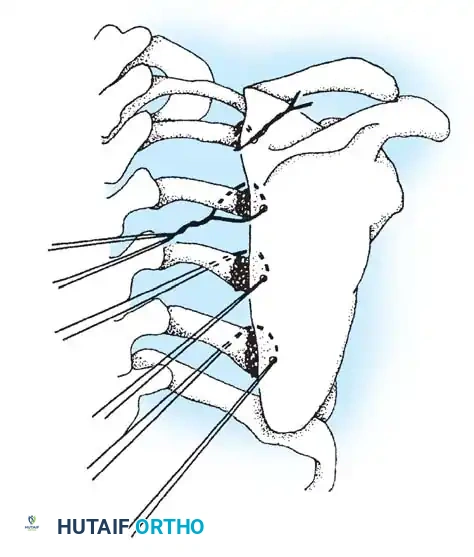
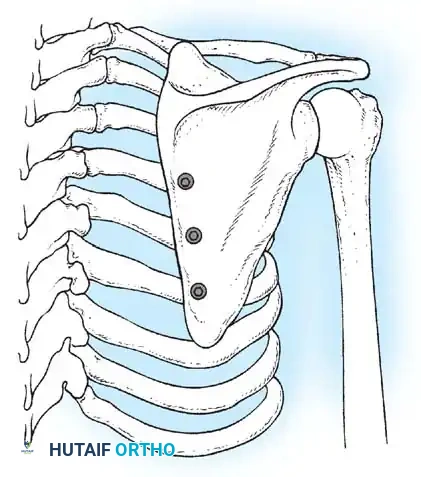
Scapulothoracic Arthrodesis in FSHD
The hallmark orthopaedic manifestation of FSHD is profound scapular winging due to selective weakness of the serratus anterior, rhomboids, and trapezius
Associated Surgical & Radiographic Imaging
📚 Medical References
You Might Also Like


