Thumb MCP Joint Collateral Ligament Reconstruction: An Intraoperative Masterclass

Key Takeaway
Join us in the OR for a masterclass on chronic thumb MCP joint collateral ligament reconstruction. We'll meticulously detail surgical anatomy, patient positioning, and step-by-step execution for UCL and RCL tears using tendon grafts. Learn critical pearls, avoid pitfalls, and understand comprehensive postoperative management to restore stability and function to the thumb.
Welcome, colleagues and fellows, to the operating theater and this comprehensive masterclass. Today, we are addressing a profoundly challenging yet highly rewarding procedure: the reconstruction of chronic instability of the thumb metacarpophalangeal (MCP) joint. This is a crucial skill set for any hand surgeon or orthopedic specialist, as untreated or inadequately managed instability inevitably leads to significant pain, profound weakness, and eventually, debilitating osteoarthritis. Our definitive goal is to restore the thumb's stable post function, an absolute biomechanical prerequisite for effective pinch, grip, and overall hand dexterity.
Comprehensive Introduction and Patho-Epidemiology
Chronic instability of the thumb MCP joint is a pathology that frequently presents to the orthopedic clinic, often after a significant delay from the initial traumatic event. The thumb relies heavily on its ligamentous restraints for stability, given its unique kinematic demands. When these restraints fail, the entire biomechanical chain of the hand is compromised.
The Burden of Chronic Thumb MCP Instability
The thumb contributes to approximately fifty percent of overall hand function. It acts as a dynamic, stable post against which the fingers can exert force during precision pinch and power grip. When the collateral ligaments of the MCP joint are incompetent, this stable post collapses under load. Patients typically present with a history of dropping objects, an inability to open jars, or sharp pain when turning a key in a lock. The functional deficit is not merely an inconvenience; it represents a profound limitation in activities of daily living and occupational tasks.
Furthermore, the chronicity of the condition implies that the window for primary repair has long closed. Acute tears, if identified early, can often be addressed with direct anatomic repair. However, once the pathology transitions to a chronic state—typically defined as presenting more than four to six weeks post-injury—the ligament ends become attenuated, retracted, and scarred. Direct repair is no longer biomechanically viable, and formal reconstruction utilizing autograft or allograft tissue becomes the mandatory surgical strategy.
The socioeconomic burden of this condition is notable. It frequently affects young, active individuals and manual laborers who sustain sporting or occupational injuries. The prolonged conservative management of unrecognized tears, followed by the requisite surgical reconstruction and extensive rehabilitation, results in significant time away from work and sport. Therefore, mastering this reconstructive technique is essential for restoring patients to their pre-injury baseline efficiently and durably.
Pathogenesis and the Mechanism of Injury
Understanding the exact mechanism of injury is paramount for anticipating the intraoperative pathology. Ulnar collateral ligament (UCL) tears, famously termed "Skier's thumb" or "Gamekeeper's thumb," are most frequently caused by a forceful hyperabduction and hyperextension moment applied to the MCP joint. This typically occurs during a fall on an outstretched hand with the thumb abducted, or when a ski pole forcefully deviates the thumb radially. The proximal phalanx deviates outward, placing catastrophic tensile stress on the UCL. The ligament usually avulses distally from its insertion on the volar-ulnar base of the proximal phalanx, though midsubstance tears and proximal avulsions from the metacarpal head do occur.
The Stener lesion is a critical pathognomonic concept in UCL injuries. Described by Bertil Stener in 1962, this occurs when the distally avulsed UCL stump retracts proximally and flips superficial to the adductor aponeurosis. The aponeurosis essentially acts as an anatomical barrier, interposing itself between the torn ligament and its bony insertion site. This interposition completely precludes any possibility of spontaneous healing, rendering conservative management futile and mandating surgical intervention. A palpable, tender soft tissue mass on the ulnar aspect of the MCP joint—the retracted ligament stump—is highly suggestive of this lesion.
Conversely, Radial Collateral Ligament (RCL) tears typically result from forceful ulnar deviation and extension of the MCP joint. Interestingly, a true Stener-type lesion is exceedingly rare on the radial side. This is due to the local anatomy: the abductor aponeurosis is considerably wider and more expansive than the adductor aponeurosis, generally allowing the torn RCL ends to remain deep to the aponeurosis. While this theoretical proximity might suggest a higher capacity for non-operative healing, chronic RCL laxity still frequently develops due to inadequate initial immobilization or progressive attenuation of the healing tissue under the shear forces of daily use.
Natural History of the Untreated Lesion
The natural history of untreated or missed complete collateral ligament tears is a relentless progression toward joint destruction. Without proper intervention, the chronic laxity subjects the articular surfaces to abnormal shear forces and asymmetrical loading. The dynamic stabilizers of the thumb, primarily the extrinsic and intrinsic musculature, cannot compensate for the loss of static ligamentous restraint.
As the joint repeatedly subluxates during pinch and grasp, the articular cartilage experiences accelerated, incongruous wear. This mechanical degradation initiates a cascade of biochemical inflammatory responses within the synovial fluid, culminating in progressive osteoarthritis. The patient will experience a transition from purely instability-related symptoms to deep, aching joint pain, stiffness, and crepitus.
Furthermore, chronic instability often leads to secondary capsular attenuation. A lateral radiograph in a chronically unstable thumb may reveal volar subluxation of the proximal phalanx relative to the metacarpal head. This indicates that the dorsal capsule has stretched out in addition to the collateral ligament failure. Once significant osteoarthritis or fixed subluxation occurs, isolated soft-tissue reconstruction is no longer viable, and the patient is relegated to a salvage procedure, typically an MCP joint arthrodesis.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the skin, the surgeon must possess a three-dimensional, encyclopedic understanding of the thumb MCP joint anatomy. Precision in identifying and respecting these structures is the difference between a functional reconstruction and an iatrogenic disaster.
Osteology and Articular Geometry
The thumb MCP joint is a unique articulation, exhibiting biomechanical characteristics of both a condyloid and a ginglymus (hinge) joint. Unlike the spherical metacarpal heads of the fingers, the thumb metacarpal head is distinctly asymmetric and flattened. It possesses two distinct condyles separated by a shallow intercondylar notch. Crucially, the radial condyle is typically taller and projects further volarly in the dorsovolar dimension than the ulnar condyle. This asymmetry dictates the complex kinematics of the joint, allowing for a slight degree of pronation during flexion, which is essential for pulp-to-pulp pinch.
The base of the proximal phalanx is correspondingly biconcave to articulate with these condyles. The joint's inherent osseous stability is relatively poor, relying heavily on the surrounding soft tissue envelope. The metacarpal head also exhibits a "cam effect." Because the collateral ligaments originate dorsal to the axis of rotation, they become progressively tighter as the joint moves from extension into flexion. This cam effect is a fundamental principle that must be replicated during graft tensioning.
Understanding this osteology is critical for precise bone tunnel placement. Tunnels must be placed at the exact anatomical origins and insertions of the native ligaments to recreate normal kinematics. Misplacement of a tunnel by even a few millimeters can result in a graft that is excessively tight in flexion (limiting motion) or too lax in extension (failing to provide stability).
The Collateral Ligament Complex
The static stability of the MCP joint is governed by a robust capsuloligamentous complex, primarily consisting of the proper and accessory collateral ligaments. The Proper Collateral Ligament (PCL) originates from a distinct fossa on the dorsal-proximal aspect of the metacarpal condyle. It courses obliquely in a volar and distal direction to insert on the volar third of the base of the proximal phalanx. Due to the aforementioned cam effect of the metacarpal head, the PCL is lax in extension and maximally taut in 30 to 40 degrees of MCP joint flexion.
Immediately volar and contiguous with the PCL is the Accessory Collateral Ligament (ACL). The ACL originates from the metacarpal head just volar to the PCL origin and extends obliquely across the joint to insert not on the phalanx, but onto the volar plate and the sesamoid bones. In contrast to the PCL, the ACL is maximally taut in full extension and becomes lax as the joint flexes.
This differential tensioning is the basis for our clinical examination. When testing for instability, applying stress in 30 degrees of flexion isolates the PCL. Applying stress in full extension tests the integrity of the ACL and the volar plate. A clinical pearl to remember is that for a joint to exhibit gross instability in extension, both the proper and accessory collateral ligaments must be completely ruptured.
Critical Neurovascular and Musculotendinous Structures
The surgical approach to the thumb MCP joint is fraught with neurovascular landmines. The most critical structures are the terminal sensory branches of the superficial radial nerve. The dorsoulnar digital nerve and the dorsoradial digital nerve invariably cross the operative field in the subcutaneous plane, immediately superficial to the adductor and abductor aponeuroses, respectively.

These nerves are highly susceptible to traction injury or direct laceration during the initial exposure. Injury to these branches results in a painful neuroma, which can be far more debilitating for the patient than the original ligamentous instability. Meticulous blunt dissection, identification, and gentle retraction with vessel loops are absolute requirements.
Deeper to the subcutaneous tissue lie the aponeuroses. On the ulnar side, the adductor aponeurosis—an extension of the adductor pollicis tendon—sweeps dorsally to contribute to the extensor mechanism. It is the proximal edge of this aponeurosis that creates the Stener lesion. On the radial side, the abductor aponeurosis, derived from the abductor pollicis brevis, serves a similar function but is anatomically broader. Recognizing these fascial layers is essential, as the native collateral ligaments and the subsequent reconstruction lie entirely deep to them.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of surgical success. Not every patient with a chronic ligament tear requires reconstruction, and in some, reconstruction is actively contraindicated. A rigorous evaluation is necessary to determine the appropriate surgical pathway.
Patient Selection for Reconstruction
The primary indication for surgical reconstruction of the thumb MCP collateral ligaments is the failure of conservative management in the setting of symptomatic, chronic instability. Patients must exhibit persistent pain and functional impairment, specifically weakness of pinch and grip that interferes with their daily vocational or avocational activities.
A thorough trial of conservative management, typically consisting of customized hand-based thermoplastic splinting, nonsteroidal anti-inflammatory drugs (NSAIDs), and activity modification, should be attempted for patients with low functional demands or mild symptoms. However, in active individuals with a clear, complete rupture and gross instability on examination, prolonged conservative care is often futile and merely delays definitive treatment.
Prophylactic reconstruction is considered a "soft" indication. Theoretically, stabilizing an asymptomatic but grossly unstable joint prevents the inevitable progression to asymmetric articular wear and osteoarthritis. However, surgeons must carefully weigh this against the risks of surgery and the prolonged postoperative rehabilitation required. Extensive preoperative counseling is necessary to align patient expectations with the realities of the recovery process.
Absolute and Relative Contraindications
Proceeding with a soft-tissue ligament reconstruction in the presence of specific contraindications will unequivocally lead to catastrophic failure, persistent pain, and the rapid need for revision surgery.
| Contraindication Type | Condition | Rationale | Management Alternative |
|---|---|---|---|
| Absolute | Significant Osteoarthritis | Stabilizing an arthritic joint increases contact pressures, exacerbating pain and stiffness. | MCP Joint Arthrodesis |
| Absolute | Fixed Joint Subluxation | Requires extensive soft tissue release to reduce, creating global instability that a single graft cannot restrain. | MCP Joint Arthrodesis |
| Absolute | Active Joint Infection | High risk of graft necrosis, hardware infection, and systemic spread. | I&D, Antibiotics, delayed Arthrodesis |
| Relative | Mild Chondromalacia | Borderline joint wear may progress despite stabilization. | Patient-specific; consider Arthrodesis |
| Relative | Patient Non-compliance | Inability to adhere to strict postoperative splinting and rehab protocols will lead to graft stretching or rupture. | Permanent Splinting |
The presence of significant osteoarthritis, demonstrated by joint space narrowing, osteophyte formation, or subchondral sclerosis on radiographs, coupled with clinical crepitus, is an absolute contraindication. In these scenarios, an MCP joint arthrodesis is the gold standard, providing a predictably pain-free, stable, and durable thumb.
Diagnostic Evaluation and Imaging
The diagnosis of chronic instability is primarily clinical, relying heavily on a meticulous physical examination. Stability testing is the cornerstone. The surgeon must stabilize the metacarpal and apply a valgus stress (for the UCL) or varus stress (for the RCL) to the proximal phalanx. This must be performed in both full extension and 30 degrees of flexion.
The most critical clinical finding is the absence of a firm, discrete endpoint during stress testing. A "mushy" or absent endpoint strongly suggests a complete ligamentous rupture. Quantitatively, we rely on the criteria popularized by Heyman et al.: greater than 30 to 35 degrees of absolute laxity in extension, or greater than 15 degrees of side-to-side difference compared to the uninjured contralateral thumb in 30 degrees of flexion, is diagnostic of a complete tear.
Radiographic evaluation is mandatory. Standard posteroanterior (PA), lateral, and oblique views of both thumbs must be obtained to rule out subtle avulsion fractures, assess for volar subluxation, and critically evaluate the joint for any signs of osteoarthritis. While advanced imaging such as MRI or ultrasound can visualize the ligamentous disruption and confirm a Stener lesion, they are rarely necessary in chronic cases where the clinical examination already dictates the need for reconstruction.
Pre-Operative Planning, Templating, and Patient Positioning
Success in the operating room is dictated by the preparation that occurs beforehand. Meticulous preoperative planning ensures that the surgeon has the necessary equipment, the optimal graft source, and a clear roadmap for the procedure.
Graft Selection and Harvesting Considerations
For chronic instability, the native ligament is non-functional, and a tendon graft is required to reconstruct the anatomical restraints. The Palmaris Longus (PL) tendon is the undisputed gold standard and the preferred donor graft. It is anatomically convenient (harvested from the ipsilateral forearm), possesses excellent biomechanical tensile strength, and its caliber is ideal for passing through the relatively small osseous tunnels in the thumb metacarpal and phalanx.
Preoperative clinical assessment of the PL is mandatory, as it is congenitally absent in approximately 10% to 15% of the population. The surgeon must ask the patient to oppose the thumb to the small finger and actively flex the wrist against resistance; a present PL will prominently bowstring at the volar wrist.
If the PL is absent, the surgeon must have a backup plan. Suitable autograft alternatives include a slip of the Extensor Indicis Proprius (EIP), the plantaris tendon (requiring a separate leg prep), or a strip of the Flexor Carpi Radialis (FCR). Allograft tissue, such as a gracilis or semitendinosus allograft, is an option but carries a theoretical risk of delayed incorporation, higher cost, and minimal risk of disease transmission.
Operating Room Setup and Patient Positioning
The patient is positioned supine on the operating room table. The affected upper extremity is placed on a radiolucent hand table. The arm should be angled slightly less than perpendicular to the torso; this prevents traction on the brachial plexus and allows the surgeon and assistant to sit comfortably around the hand.
A pneumatic tourniquet is applied to the proximal arm over generous padding. A bloodless surgical field is absolutely critical for identifying the delicate sensory nerves and defining the aponeurotic layers. The tourniquet is typically set to 250 mmHg, or 100 mmHg above the patient's systolic blood pressure.
Fluoroscopy is an indispensable tool for this procedure. The C-arm must be positioned and draped prior to the incision. It should come in from the foot or head of the table, allowing for seamless intraoperative imaging without requiring the patient or the hand table to be moved. Real-time fluoroscopy is utilized to verify the starting points for the osseous tunnels, confirm the trajectory of the drill, and ensure the final placement of fixation hardware.
Anesthesia and Pre-Incision Examination
The procedure is typically performed under regional anesthesia, specifically an axillary or supraclavicular brachial plexus block, often supplemented with intravenous sedation or light general anesthesia. Regional anesthesia provides excellent intraoperative muscle relaxation and profound postoperative pain control.
Once the patient is anesthetized and the muscles are fully relaxed, an Examination Under Anesthesia (EUA) is performed. This is a critical step. Without the guarding and muscle spasm present in the clinic, the true extent of the instability is often unmasked. The surgeon should document the degree of laxity in both flexion and extension and compare it to the contralateral side if it is accessible. This final assessment confirms the surgical plan just moments before the incision.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution requires a blend of delicate soft-tissue handling and precise osseous engineering. The goal is to recreate the native anatomy as accurately as possible to restore normal kinematics.
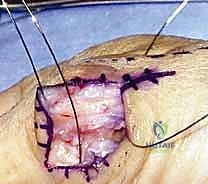
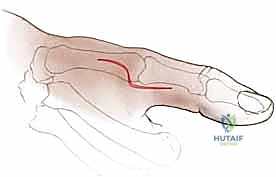
Incision Design and Superficial Dissection
Several incision options are available, but the "Lazy-S" or a modified chevron incision provides optimal exposure while minimizing the risk of scar contracture over the flexion crease of the joint. For a UCL reconstruction, the incision is centered over the ulnar aspect of the MCP joint. The proximal limb starts dorsally over the metacarpal neck, curves volarly to cross the joint line obliquely, and then extends distally along the midaxial line of the proximal phalanx.

The skin is incised with a #15 blade. The superficial dissection must proceed with extreme caution using blunt dissecting scissors. The superficial fascia is carefully spread to identify the dorsoulnar sensory nerve branches.

These nerves are meticulously mobilized, isolated with vessel loops, and gently retracted dorsally or volarly, depending on their anatomical course. Retraction must be gentle to avoid a traction neuropraxia.

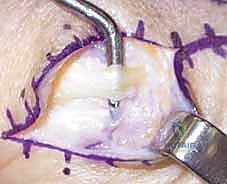
Arthrotomy and Joint Preparation
Once the nerves are protected, the adductor aponeurosis is identified. It appears as a transverse band of fascial tissue blending into the extensor mechanism.

The aponeurosis is incised longitudinally, leaving a sufficient cuff of tissue volarly for later repair. Deep to the aponeurosis, the remnants of the native UCL and the joint capsule are encountered.

In chronic cases, the ligament is often a mass of disorganized scar tissue. The joint capsule is opened longitudinally. The articular surfaces of the metacarpal head and proximal phalanx are inspected to confirm the absence of advanced arthrosis. The remnants of the native ligament are sharply excised to expose the bare bone at the anatomical origin and insertion sites. The joint is thoroughly irrigated and debrided of any fibrotic scar tissue that might impede reduction.
Osseous Tunnel Preparation
The creation of the osseous tunnels is the most technically demanding portion of the procedure. The reconstruction relies on anatomical placement.
First, the metacarpal origin is addressed. The center of the native UCL origin is identified on the dorsal-proximal aspect of the ulnar condyle.

A 0.045-inch Kirschner wire (K-wire) is driven transversely across the metacarpal neck from ulnar to radial. The trajectory must be parallel to the joint surface in the coronal plane. Fluoroscopy is utilized to confirm the K-wire position. Once confirmed, the K-wire is over-drilled with a cannulated drill bit, typically 3.0mm to 4.0mm in diameter, depending on the caliber of the harvested graft.

Next, the phalangeal tunnel is created. The anatomical insertion is on the volar-ulnar aspect of the proximal phalanx base. A K-wire is introduced at this point and directed dorsally and radially, exiting the radial cortex of the phalanx. Again, fluoroscopy confirms the position before over-drilling.

Care must be taken to maintain an adequate bone bridge to prevent iatrogenic fracture during drilling or later graft tensioning.

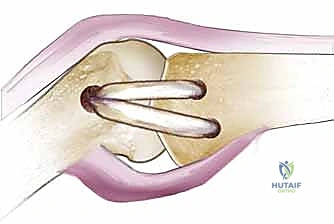
Graft Passage, Tensioning, and Fixation
The harvested palmaris longus graft is prepared on the back table. A running locking suture (e.g., 2-0 FiberWire) is placed in both ends of the graft to facilitate passage.

Various routing techniques exist, but the figure-of-eight configuration or a simple docking technique are most common. Using a suture passing wire, the graft is pulled through the metacarpal tunnel from ulnar to radial, and then routed back over the dorsal aspect of the metacarpal neck.
Clinical & Radiographic Imaging Archive