Reconstruction for Missed Monteggia Lesion

Introduction and Epidemiology
Monteggia fracture-dislocations represent a rare and complex spectrum of traumatic upper extremity injuries, classically defined by a fracture or plastic deformation of the ulnar diaphysis or metaphysis coupled with proximal radioulnar joint (PRUJ) dissociation and radiocapitellar joint (RCJ) dislocation. These injuries most frequently occur in the pediatric population, typically affecting children between 4 and 10 years of age.
Despite the well-documented nature of this injury pattern, the diagnosis of an acute Monteggia fracture-dislocation is notoriously elusive. It is frequently missed upon initial presentation by skilled emergency physicians, pediatricians, radiologists, and even orthopedic surgeons. Misdiagnosis often occurs because the radial head dislocation is overlooked in the presence of a seemingly innocuous or isolated ulnar fracture, or because the ulnar injury presents merely as plastic deformation rather than a frank cortical disruption. Consequently, late presentation of a previously undetected traumatic dislocation of the radial head is a well-recognized clinical entity.
In children presenting with a seemingly isolated dislocation of the radial head, rigorous scrutiny of orthogonal forearm radiographs almost invariably demonstrates plastic deformation or a fracture malunion of the ulna. The confluence of these radiographic findings establishes the diagnosis of a chronic Monteggia fracture-dislocation (or chronic Monteggia lesion), distinguishing it from congenital radial head dislocation. Patients with chronic Monteggia lesions present at highly variable time points. In some instances, the radial head dislocation is discovered several weeks after initiating conservative treatment for a misdiagnosed isolated ulnar fracture. In other scenarios, the diagnosis remains obfuscated for months or years, ultimately manifesting as progressive elbow pain, substantial loss of motion, cubitus valgus malalignment, or tardy neuropathy.
The management of a chronic Monteggia lesion is exponentially more complex than the acute recognition and anatomical reduction of the primary injury. Nevertheless, due to the progressive nature of pain, restriction of motion, and functional disability, surgical reconstruction is indicated for the majority of symptomatic patients with preserved joint morphology.

Surgical Anatomy and Biomechanics
A profound understanding of the osseous, ligamentous, and neurovascular anatomy of the elbow and forearm is paramount for the successful reconstruction of a chronic Monteggia lesion.
Osteology and Ligamentous Stabilizers
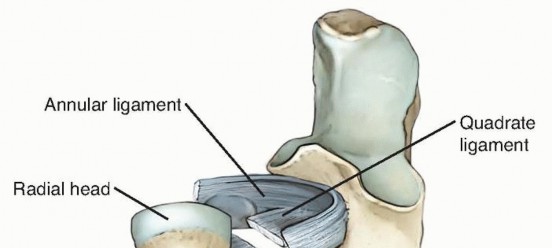
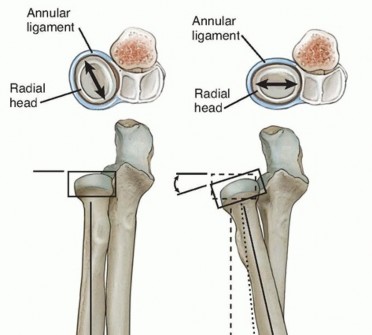
The proximal radioulnar joint is stabilized primarily by the annular ligament, which acts as the principal restraint to radial head translation during forearm rotation. The annular ligament originates and inserts on the anterior and posterior margins of the lesser sigmoid notch of the ulna, respectively, encircling the radial head.
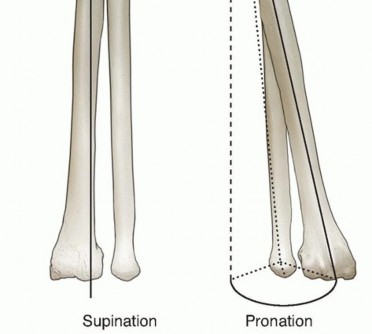
In supination, the annular ligament and the quadrate ligament become taut, thereby maximizing the stability of the PRUJ. The radial head itself is elliptical rather than perfectly spherical; consequently, during forearm supination, the long axis of the radial head positions itself perpendicularly to the lesser sigmoid notch. This anatomical cam effect causes the annular ligament and the anterior segment of the quadrate ligament to tighten, providing terminal stability.
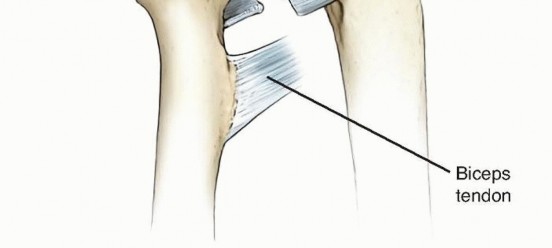
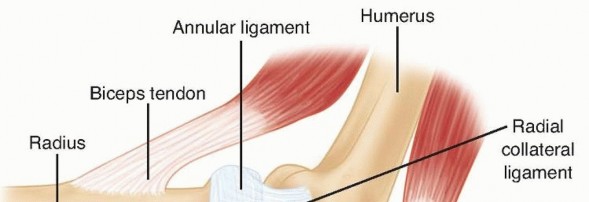
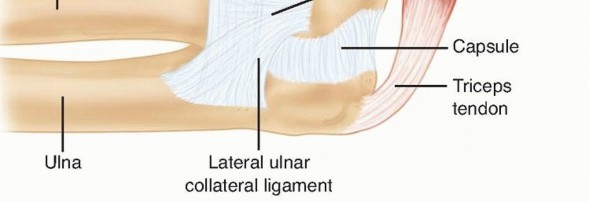
The lateral ligamentous complex of the elbow is a Y-shaped structure consisting of the radial collateral ligament (RCL), the lateral ulnar collateral ligament (LUCL), and the annular ligament. The LUCL provides critical restraint against posterolateral rotatory instability (PLRI), while the annular ligament maintains the radiocapitellar articulation.

Neurovascular Considerations
The radial nerve and its terminal branches are intimately associated with the anterior and lateral aspects of the elbow joint. The radial nerve emerges proximal to the elbow in the interval between the brachioradialis and the brachialis muscles. At the level of the radiocapitellar joint, it bifurcates into the superficial sensory branch and the posterior interosseous nerve (PIN).
The PIN courses distally and dives beneath the arcade of Frohse, passing through the two heads of the supinator muscle. The extreme proximity of the PIN to the radial head and neck renders it highly susceptible to iatrogenic injury during surgical exposure, capsular release, and annular ligament reconstruction in chronic Monteggia lesions. Furthermore, in the setting of chronic anterior radial head dislocation, the PIN may become intimately adhered to the displaced anterior capsule or the radial head itself.



Pathogenesis and Natural History
The Bado Classification
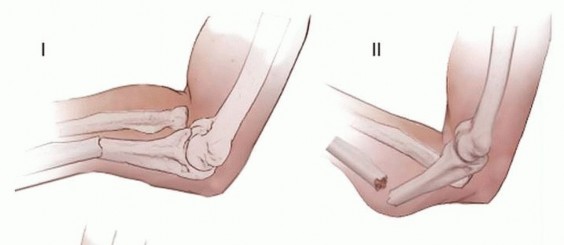
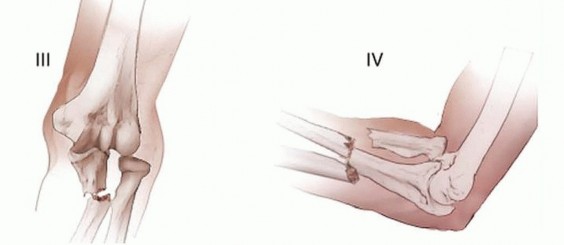
The Bado classification categorizes Monteggia fracture-dislocations based on the direction of the radial head dislocation and the apex of the ulnar fracture deformity:
* Type I: Anterior dislocation of the radial head with an apex-anterior fracture of the ulnar diaphysis. This is the most common pattern in the pediatric population (accounting for over 70% of cases).
* Type II: Posterior or posterolateral dislocation of the radial head associated with an apex-posterior ulnar diaphyseal or metaphyseal fracture. While this is the most common pattern in adults, it represents approximately 5% of pediatric Monteggia lesions.
* Type III: Lateral dislocation of the radial head associated with an apex-lateral (varus) fracture of the proximal ulna. This is the second most common Monteggia lesion in children, representing nearly 30% of pediatric injuries.
* Type IV: Anterior dislocation of the radial head combined with fractures of both the radial shaft and the ulna. This pattern is exceedingly rare in children.
Mechanism of Chronicity
Because the pediatric ulna heals rapidly, a missed acute injury can consolidate into a chronic Monteggia lesion within a mere 3 to 4 weeks. Most chronic lesions in children are characterized by anterior dislocation of the radial head and apex-anterior ulnar fracture malunion or plastic deformation. Suboptimal initial treatment—such as closed reduction and casting of a complete ulnar fracture without ensuring PRUJ stability—can also result in late subluxation or dislocation. Strict orthopedic principles dictate that only true plastic deformation and greenstick ulnar fractures should be managed nonoperatively. Complete transverse or short oblique fractures necessitate intramedullary fixation, while long oblique or comminuted fractures require open reduction and internal fixation (ORIF) with plate osteosynthesis to prevent late instability.
Natural History of the Untreated Lesion
Historically, literature suggested that the natural history of an untreated chronic Monteggia lesion was relatively benign, leading to recommendations of "skillful neglect" followed by radial head excision at skeletal maturity. Contemporary longitudinal data, however, definitively refutes this approach. The unreduced radial head leads to progressive biomechanical derangement. Patients predictably develop activity-related pain, radiocapitellar arthrosis, progressive loss of motion (particularly terminal elbow flexion and forearm pronation), and progressive cubitus valgus. Furthermore, the increasing valgus deformity and chronic anterior radial head displacement place insidious traction on the neurovascular structures, leading to documented cases of tardy ulnar, median, and posterior interosseous nerve palsies.
Clinical Evaluation and Diagnosis
Patient History
A meticulous history usually reveals a distinct traumatic event, typically a fall onto an outstretched hand with the elbow extended and the forearm hyper-pronated. This traumatic etiology is critical for differentiating a missed Monteggia lesion from a congenital radial head dislocation. If the child is under 4 years of age and the trauma was minor (e.g., axial traction), radial head subluxation (nursemaid’s elbow) must be considered; however, the persistence of symptoms beyond standard reduction maneuvers warrants advanced radiographic evaluation.
Physical Examination
Inspection often reveals an abnormal carrying angle. Normal pediatric carrying angles average 9.3 degrees in males and 11.5 degrees in females. Patients with chronic Monteggia lesions frequently exhibit progressive cubitus valgus, occasionally exceeding 30 degrees, which can be a significant functional and aesthetic concern. Palpation of the cubital fossa often reveals a distinct anterior fullness corresponding to the dislocated radial head. Crepitation during forearm rotation suggests early arthrotic changes.
Range of motion (ROM) must be meticulously documented. Normal elbow ROM spans from 4 degrees of hyperextension to 145 degrees of flexion. Chronic Bado Type I lesions typically cause a mechanical block to terminal flexion due to the anteriorly dislocated radial head abutting the distal humerus (average flexion limited to 110 degrees). Forearm rotation must be assessed by isolating the radiocarpal and midcarpal joints; the examiner must track the rotation of the radial styloid relative to the ulnar axis to avoid being misled by compensatory wrist rotation.
A comprehensive neurologic examination is mandatory. Tardy ulnar nerve palsy may manifest as diminished sensibility in the autonomous zone of the small finger, intrinsic muscle atrophy, clawing, or a positive Froment/Wartenberg sign. Tardy PIN palsy presents as weakness in metacarpophalangeal joint extension and thumb retropulsion, with preserved wrist extension (due to radial nerve innervation of the ECRL proximal to the PIN bifurcation) accompanied by radial deviation during wrist extension.
Imaging Studies
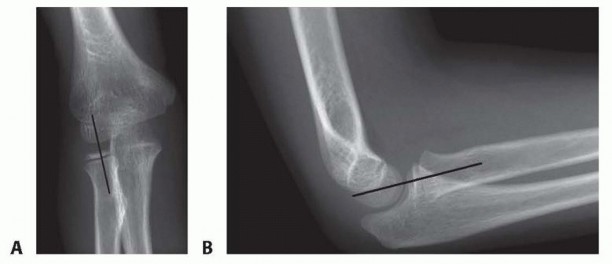
Standard anteroposterior (AP) and lateral radiographs of the elbow and forearm are the cornerstone of diagnosis. The most critical radiographic parameter is the radiocapitellar line, which must bisect the capitellum in all radiographic views. A disruption of this line is highly indicative of radial head dislocation. However, in chronic or subtle Bado Type I lesions, the radiocapitellar line may appear falsely normal on a true AP radiograph; thus, the lateral view is paramount.
The ulna must be scrutinized for plastic deformation, defined as a deviation from its normally straight dorsal border (the "ulnar bow sign"). In chronic cases, heterotopic ossification or calcification of the displaced annular ligament and anterior capsule may be visible and should not be mistaken for intra-articular loose bodies.

Differential Diagnosis
- Congenital radial head dislocation (characterized by bilateral involvement, a hypoplastic/flattened capitellum, and a convex, dome-shaped radial head deformity).
- Nursemaid's elbow (radial head subluxation).
- Isolated traumatic radial head dislocation.
- Traumatic elbow dislocation.
Indications and Contraindications
The primary indication for surgical reconstruction is a symptomatic chronic Monteggia lesion in a patient with preserved radiocapitellar joint morphology. The goal is to restore elbow kinematics, resolve pain, and prevent progressive valgus deformity and tardy neuropathy.
Contraindications:
Surgical reconstruction is contraindicated if there are irreversible morphologic changes to the joint. While some historical literature suggests age (e.g., >12 years) or time from injury (e.g., >3 years) as absolute contraindications, contemporary orthopedic consensus prioritizes joint morphology over chronological age. Advanced imaging (MRI or 3D CT) should be utilized in older patients or long-standing lesions to evaluate cartilage quality.
Absolute contraindications include:
* Significant radial head enlargement or dome-shaped deformity.
* Severe flattening or hypoplasia of the capitellum.
* Established radiocapitellar arthrosis.
In patients with these contraindications, observation is warranted. If symptoms become debilitating, radial head excision may be considered post-skeletal maturity, though this carries the inherent risks of proximal radial migration, wrist pain (Essex-Lopresti equivalent), and progressive cubitus valgus.
Preoperative Planning and Patient Positioning
Preoperative evaluation requires careful templating of the ulnar osteotomy. The surgeon must determine the apex of the ulnar malunion to plan the osteotomy site. The degree of angulation and lengthening required to anatomically reduce the radiocapitellar joint must be estimated.
General anesthesia is strictly preferred over regional blocks. A regional block obscures the immediate postoperative neurologic examination, which is critical for detecting iatrogenic PIN injury or the onset of compartment syndrome.
The patient is positioned supine with the operative extremity extended onto a radiolucent hand table. A sterile pneumatic tourniquet is applied high on the brachium to allow for an extensile posterior approach. The entire upper limb, up to the axilla, is prepped and draped to allow full manipulation of the extremity.
Detailed Surgical Approach and Technique
The modern surgical reconstruction of a chronic Monteggia lesion encompasses three critical components: (1) an ulnar lengthening and angulation osteotomy, (2) open reduction of the radiocapitellar joint, and (3) repair or reconstruction of the annular ligament.
Extensile Posterolateral Approach
An extensile posterolateral approach is utilized to access both the ulnar diaphysis and the radiocapitellar joint while allowing direct visualization and protection of the PIN.
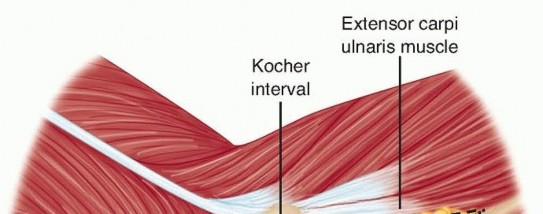
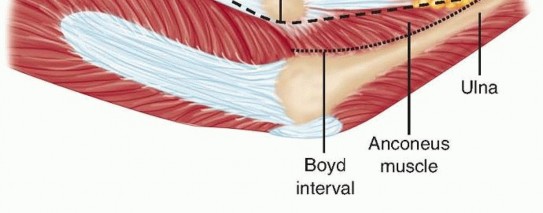

- Incision and Deep Dissection: A curvilinear incision is made over the lateral aspect of the elbow, extending distally along the subcutaneous border of the ulna. The Kocher interval (between the anconeus and the extensor carpi ulnaris) or the Boyd interval may be utilized.
- Nerve Protection: The radial nerve is identified in the interval between the brachioradialis and brachialis. It is traced distally to its bifurcation. The PIN is meticulously dissected and mobilized away from the anterior elbow capsule. In chronic lesions, the PIN is often adherent to the capsule or the dislocated radial head; failure to directly visualize the nerve risks catastrophic transection during capsular release.
- Joint Exposure: The radiocapitellar joint is exposed. The dislocated radial head and the interposed, collapsed, or fibrotic annular ligament are identified. The joint is cleared of fibrotic tissue to allow for subsequent reduction.


Ulnar Osteotomy and Fixation
The ulnar osteotomy is the biomechanical linchpin of the operation. Without correcting the ulnar length and alignment, the radial head cannot be stably maintained in the capitellar fossa.
- Osteotomy Execution: Using an oscillating saw with copious saline irrigation (to prevent thermal necrosis), a transverse or oblique osteotomy is performed at the apex of the ulnar malunion.
- Correction: The ulna is distracted and angulated. For a typical Bado Type I lesion, the ulna must be lengthened and angulated posteriorly (apex dorsal) to create the necessary tension on the interosseous membrane to pull the radial head posteriorly and distally into the joint. Overcorrection of the ulnar deformity is frequently required to achieve a stable radiocapitellar reduction.
- Fixation: Once the radial head is visually and fluoroscopically reduced, the ulnar osteotomy is stabilized using a contoured dynamic compression plate or locking plate. In younger children, double-stacked one-third tubular plates may be utilized. A minimum of four to six cortices of fixation must be achieved on both sides of the osteotomy. If a structural gap exists after distraction, autograft (from the local callus) or allograft bone is packed into the defect to prevent nonunion.


Annular Ligament Reconstruction
While the ulnar osteotomy provides the macro-stability, reconstruction of the annular ligament provides micro-stability and prevents anterior subluxation during active supination.
Several techniques exist:
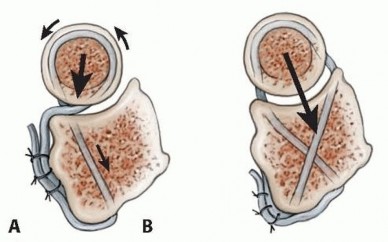
* Bell-Tawse Technique: Originally described utilizing a turn-down slip of the central triceps tendon/fascia, which is passed around the radial neck and sutured to the ulna, providing a posteriorly directed vector force.
* Seel and Peterson Technique: Involves creating crossing drill holes at the anterior and posterior rims of the lesser sigmoid notch, allowing for a more anatomical recreation of the ligament's origin and insertion.
* Lateral Triceps Slip or Palmaris Longus Autograft: Alternative graft choices depending on surgeon preference and tissue availability.
Prophylactic Fasciotomies and Closure
Due to the extensive surgical dissection, ulnar lengthening, and the risk of postoperative swelling, limited prophylactic fasciotomies of the volar and dorsal forearm compartments are strongly advocated to mitigate the risk of compartment syndrome.
Final orthogonal fluoroscopy confirms the stable reduction of the radiocapitellar and proximal radioulnar joints. Transarticular radiocapitellar pinning with a smooth Kirschner wire is rarely indicated if the ulnar osteotomy is biomechanically sound; however, in revision cases or highly unstable joints, a stout, smooth K-wire may be utilized to hold the joint for 3 to 4 weeks.
The periosteum over the ulna is meticulously repaired to expedite osteogenesis. The extensor-supinator origin is reattached to the lateral epicondyle. The wound is typically closed in layers over a closed-suction drain (e.g., Jackson-Pratt) to prevent hematoma formation.
Postoperative Rehabilitation Protocols
Immediately postoperatively, the patient is placed in a well-padded, bivalved long-arm cast. The elbow is typically immobilized in 80 to 90 degrees of flexion, with the forearm positioned in 60 to 90 degrees of supination. This position maximizes the bony congruity of the PRUJ and tightens the reconstructed annular ligament.
The patient must be admitted for 24 to 48 hours for rigorous pain control and serial neurovascular checks to monitor for compartment syndrome.
The cast is maintained for 4 to 6 weeks to allow for initial bony consolidation of the ulnar osteotomy and soft tissue healing of the ligament reconstruction. Following cast removal, the patient is transitioned to a custom, removable long-arm splint for an additional 3 to 4 weeks. Splint removal for supervised, active, and active-assisted range of motion exercises is initiated. Formal physical therapy is critical. Elbow flexion and extension typically recover more rapidly than forearm rotation. Maximal functional recovery is generally anticipated at 6 to 12 months postoperatively.
Outcomes and Complications
Clinical Outcomes
Data regarding the surgical reconstruction of chronic Monteggia lesions is largely derived from retrospective, single-center case series. Nakamura et al. reported long-term outcomes (average 84 months) in 22 children undergoing combined ulnar osteotomy and annular ligament reconstruction. The radial head remained anatomically stable in approximately 80% of patients, while asymptomatic subluxation occurred in 20%.
Functional outcomes, measured via the Mayo Elbow Performance Index (MEPI), reliably improve postoperatively. Average elbow flexion typically improves from approximately 120 degrees to near-normal (138 degrees). Postoperative forearm pronation usually exceeds 65 degrees, though patients should be counseled that some permanent loss of terminal forearm rotation (particularly pronation) is expected. Superior outcomes are reliably correlated with younger patient age (<12 years) and shorter duration from injury to surgery (<3 years).
Complications
The complication profile for this complex reconstruction is substantial:
* Compartment Syndrome: The combination of extensive dissection and bone lengthening creates a high-risk environment. Pain out of proportion, increasing narcotic demand, and pain with passive stretch require immediate evaluation. Prophylactic fasciotomies are highly recommended.
* Posterior Interosseous Nerve Palsy: Can occur via direct transection or traction. If the nerve was visually protected during surgery, a postoperative deficit is usually a neuropraxia. Expectant management with serial clinical exams (tracking the advancing Tinel sign) is indicated. Lack of clinical recovery by 6 months warrants surgical exploration.
* Ulnar Nerve Palsy: May occur secondary to extensive acute lengthening of the ulna, occasionally necessitating prophylactic or delayed in-situ decompression or transposition.
* Recurrent Radial Head Subluxation/Dislocation: Occurs in up to 20% of cases. Usually stems from an under-corrected ulnar osteotomy or failure of the ligamentous reconstruction.
* Radial Neck Notching: Can occur if the annular ligament reconstruction graft is tensioned too tightly, leading to mechanical wear on the radial neck.
* Ulnar Nonunion: Mitigated by utilizing a stable plate construct, ensuring an incomplete hinged osteotomy if possible, repairing the periosteum, and utilizing local/allograft bone grafting.
References
- Bado JL. The Monteggia lesion. Clin Orthop Relat Res 1967;50: 71-86.
- Bell Tawse AJ. The treatment of malunited anterior Monteggia fractures in children. J Bone Joint Surg Br 1965;47:718-723.
- Chen WS. Late neuropathy in chronic dislocation of the radial head. Report of two cases. Acta Orthop Scand 1992;63:343-344.
- Dormans JP, Rang M. The problem of Monteggia fracture-dislocations in children. Orthop Clin North Am 1990;21:251-256.
- Exner GU. Missed chronic anterior Monteggia lesion. Closed reduction by gradual lengthening and angulation of the ulna. J Bone Joint Surg Br 2001;83:547-550.
-
Academic Resource & Medical Review
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
Disclaimer: The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.


