Menisci: Anatomy, Biomechanics, and Surgical Management
Key Takeaway
The menisci are vital fibrocartilaginous structures essential for load transmission, shock absorption, and joint stability in the knee. Understanding their complex ultrastructure, vascularity, and biomechanical hoop tension is critical for orthopedic surgeons. This comprehensive guide details meniscal anatomy, kinematics, and evidence-based surgical management, emphasizing meniscal preservation techniques to prevent early-onset osteoarthritis and optimize long-term patient outcomes.
Introduction to Meniscal Function and Anatomy
Meniscal integrity is paramount to the normal kinematic function and longevity of the knee joint. Historically viewed as vestigial remnants, the menisci are now universally recognized as critical structures that act as joint fillers, compensating for gross incongruities between the convex femoral condyles and the relatively flat tibial plateaus. They provide essential functions including load transmission, shock absorption, joint stability, proprioception, and articular cartilage lubrication.
The menisci are crescent-shaped, roughly triangular in cross-section, and cover one-half to two-thirds of the articular surface of their corresponding tibial plateaus. The peripheral edges are convex, thick, and firmly attached to the inner surface of the knee joint capsule (except at the popliteal hiatus laterally). They are loosely attached to the borders of the tibial plateaus by the coronary ligaments. The inner edges are concave, thin, and unattached, allowing for dynamic deformation during knee motion.
The Medial Meniscus
The medial meniscus is a C-shaped structure with a larger radius than its lateral counterpart. Its posterior horn is significantly wider than the anterior horn. The anterior horn attaches firmly to the tibia anterior to the intercondylar eminence and blends with the anterior cruciate ligament (ACL). The posterior horn is anchored immediately anterior to the posterior cruciate ligament (PCL) attachments. Its entire peripheral border is firmly affixed to the deep medial collateral ligament (MCL) and the medial capsule, rendering it less mobile and consequently more susceptible to shear forces and tearing during rotational stress.
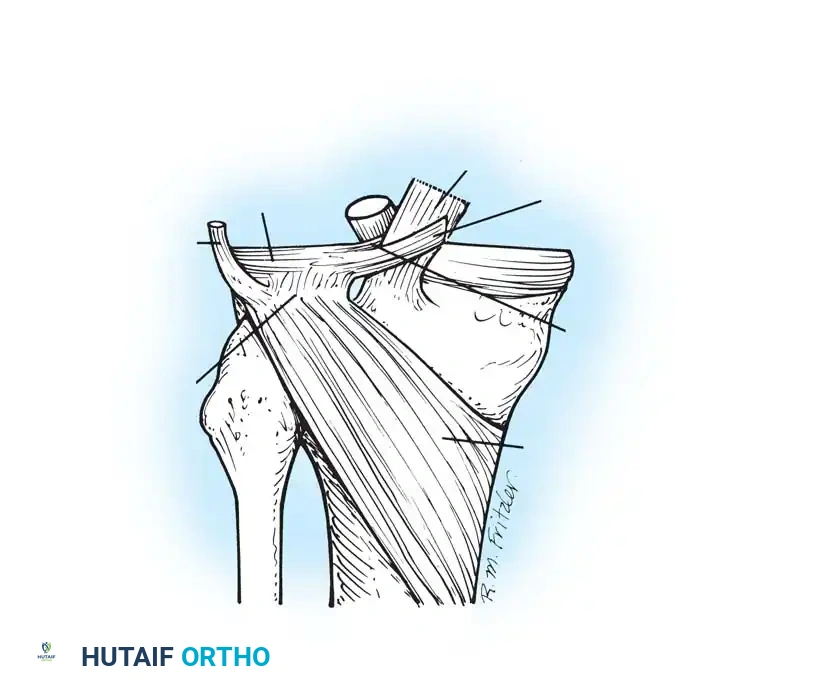
The Lateral Meniscus
The lateral meniscus is more circular, covering up to two-thirds of the lateral tibial plateau. It is smaller in diameter, thicker at its periphery, wider in its body, and significantly more mobile than the medial meniscus. The anterior horn attaches medially in front of the intercondylar eminence, while the posterior horn inserts into the posterior aspect of the intercondylar eminence.
Crucially, the lateral meniscus is separated from the lateral collateral ligament (LCL) by the popliteus tendon, which passes through the popliteal hiatus. The posterior horn receives anchorage to the femur via the meniscofemoral ligaments—the ligament of Humphry (anterior to the PCL) and the ligament of Wrisberg (posterior to the PCL). This complex attachment to the popliteus muscle and meniscofemoral ligaments allows the lateral meniscus to follow the lateral femoral condyle during rotation, protecting it from entrapment.
Ultrastructure and Collagen Architecture
The menisci are composed of dense, tightly woven extracellular matrix, primarily water (72%) and collagens (22%), with Type I collagen accounting for 90% of the collagenous framework. This specific arrangement provides extraordinary elasticity and the ability to withstand immense compressive loads.
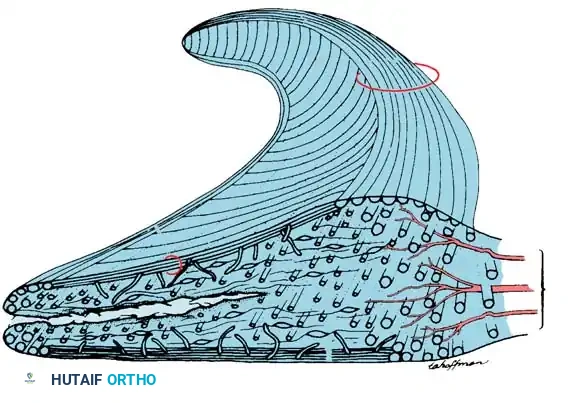
The collagen fibers are arranged in three distinct patterns:
* Circumferential Fibers: The major orientation of collagen fibers is circumferential. These fibers act similarly to metal hoops placed around a pressurized wooden barrel, resisting the outward radial forces generated by axial loading.
* Radial Fibers: These fibers act as "tie fibers," binding the circumferential fibers together to prevent longitudinal splitting.
* Perforating Fibers: These provide structural cohesion across different layers of the meniscus.
Clinical Pearl: The ultrastructural arrangement of collagen fibers dictates the characteristic patterns of meniscal tears. When a force is applied perpendicular to the fiber direction, meniscal strength decreases to less than 10%.
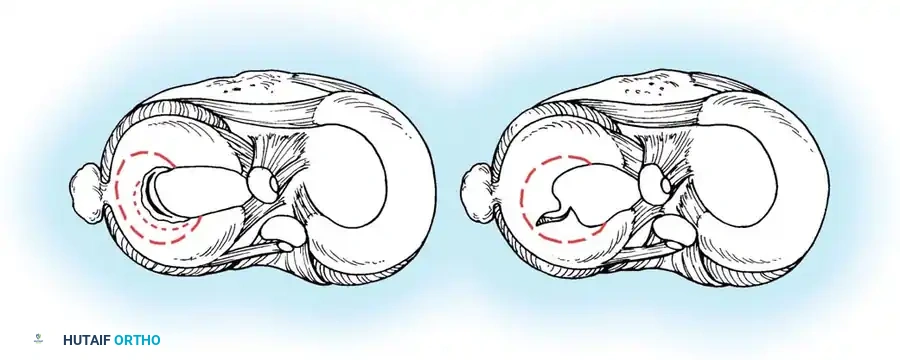
Cross-section demonstrating a horizontal cleavage split, often degenerative in nature, separating the superior and inferior meniscal leaves.
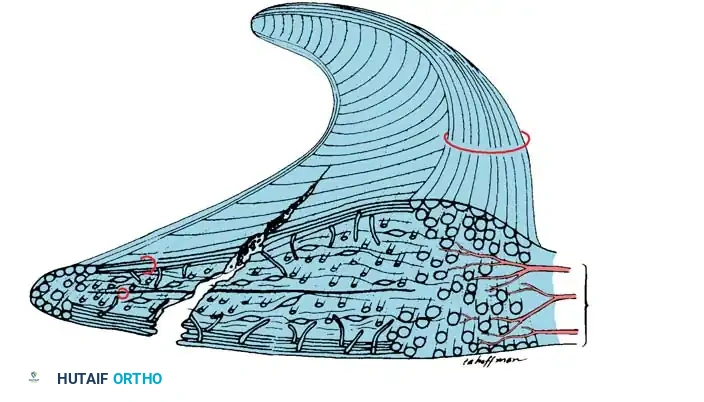
Cross-section showing the direction of a longitudinal tear, which typically occurs obliquely between the circumferential fibers.
Biomechanics and Kinematics
Load Transmission and Hoop Tension
The menisci are responsible for transmitting 40% to 60% of the superimposed weight in the standing position. The compression of the menisci by the tibia and femur generates outward forces that attempt to extrude the menisci from the joint. The circumferential tension (hoop tension) counteracts this radial force. These hoop forces are transmitted to the tibia through the strong anterior and posterior root attachments.
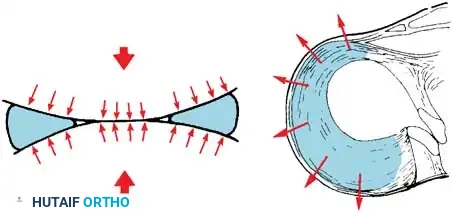
Intact hoop tension keeps the meniscus securely positioned between the articular surfaces during axial loading.
When a single radial cut or a complete root tear occurs, hoop tension is catastrophically lost. The meniscus extrudes, and its load-bearing capacity is effectively reduced to zero—biomechanically equivalent to a total meniscectomy.
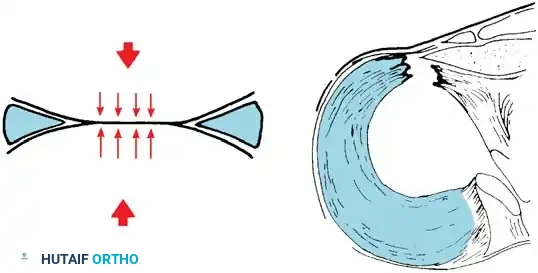
Loss of hoop tension due to a radial tear or root avulsion allows the meniscus to extrude, eliminating its protective load-sharing function.
Contact Area and Joint Stress
The larger contact area provided by the menisci reduces the average contact stress acting between the bones.
* Medial Meniscectomy: Decreases contact area by 50% to 70% and increases contact stress by 100%.
* Lateral Meniscectomy: Decreases contact area by 40% to 50% but dramatically increases contact stress by 200% to 300% due to the convex-on-convex articulation of the lateral compartment.
Surgical Warning: Increased contact stress resulting from decreased contact area produces rapid bone remodeling (Wolff's Law), flattening of the femoral condyle, joint space narrowing, and early-onset osteoarthritis. Preservation of the lateral meniscus is especially critical due to the exponential increase in contact stress following its removal.
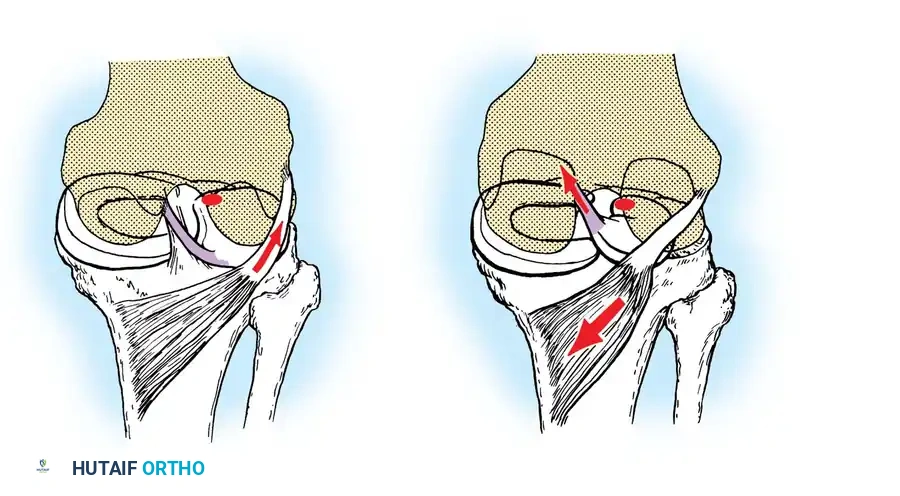
Kinematics and Stability
During flexion and extension, the menisci follow the tibial condyles. However, during rotation, they follow the femur. The medial meniscus, being firmly anchored, becomes distorted during rotation and is highly susceptible to injury. In contrast, the lateral meniscus is drawn backward by the popliteus muscle during internal tibial rotation and flexion, preventing it from being crushed between the condyles.
In the ACL-deficient knee, the medial meniscus becomes the primary secondary restraint to anterior tibial translation. Medial meniscectomy in an ACL-deficient knee increases anterior tibial translation by 58% at 90 degrees of flexion.
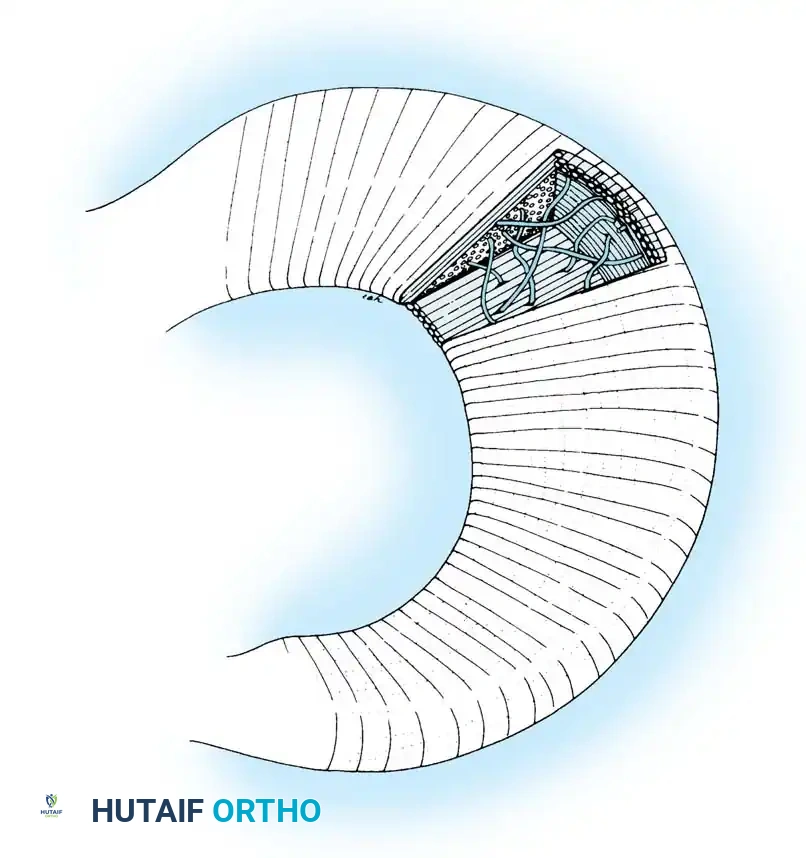
Vascularity and Healing Potential
The healing potential of a meniscal tear is directly proportional to its blood supply. Arnoczky and Warren's seminal microvascular studies demonstrated that the vascular supply originates predominantly from the lateral and medial geniculate vessels (inferior and superior).
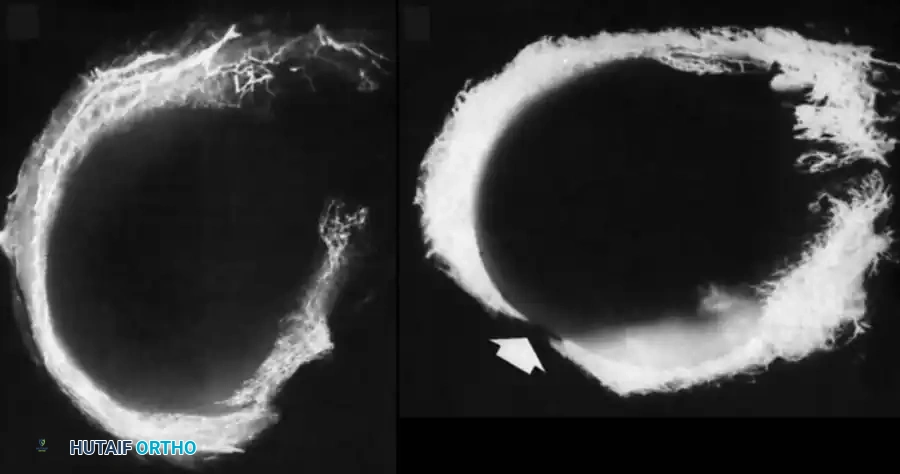
These vessels form a perimeniscal capillary plexus within the synovial and capsular tissue, supplying only the peripheral 10% to 30% of the medial meniscus and 10% to 25% of the lateral meniscus.
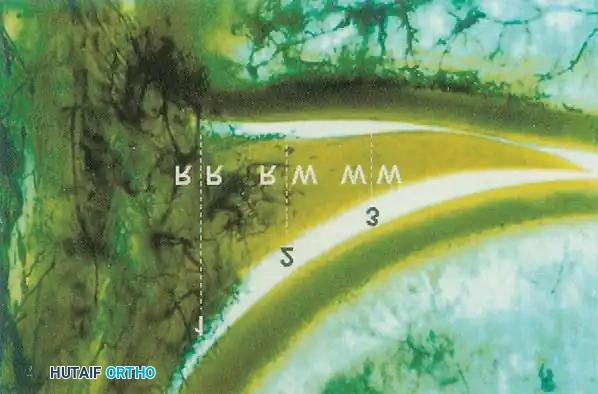
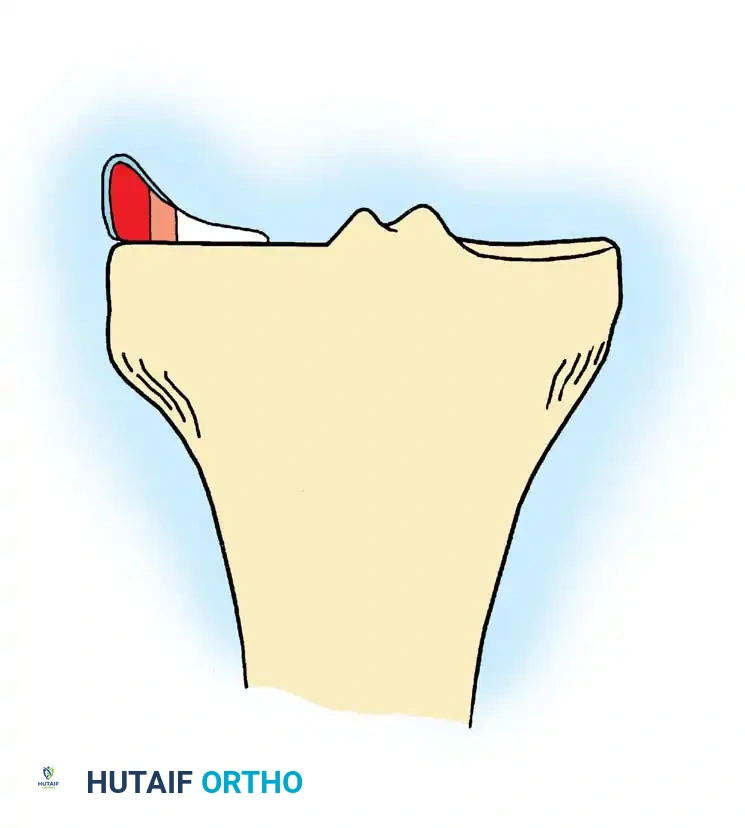
Based on this vascularity, the meniscus is divided into three zones:
1. Red-Red Zone: The fully vascularized peripheral 3 mm. Tears here have an excellent prognosis for healing following repair.
2. Red-White Zone: The watershed area (3-5 mm from the periphery). Healing is possible but requires biological augmentation (e.g., vascular access channels, fibrin clot, PRP).
3. White-White Zone: The avascular central portion. Tears here generally do not heal and are typically managed with partial meniscectomy.
Experimental studies show that lesions in the vascular zone fill with a cellular fibrovascular scar that matures into fibrocartilage over several months. Complete regeneration of excised meniscal tissue only occurs if the excision extends into the peripheral vascular synovial tissue, and even then, the regenerated tissue is biomechanically inferior to native meniscal cartilage.
Clinical Evaluation and Imaging
History and Physical Examination
Patients typically present with a history of a twisting injury with the foot planted, followed by delayed effusion (over 24 hours), joint line pain, and mechanical symptoms such as catching, locking, or giving way.
Physical examination must include:
* Joint Line Tenderness: Highly sensitive for meniscal pathology.
* McMurray Test: Flexion with rotation and varus/valgus stress to trap the torn fragment.
* Apley Grind Test: Prone compression and rotation.
* Thessaly Test: Dynamic weight-bearing rotation at 20 degrees of flexion.

Imaging
While plain radiographs (weight-bearing AP, lateral, Rosenberg, and skyline views) are essential to rule out osteoarthritis or loose bodies, Magnetic Resonance Imaging (MRI) is the gold standard for diagnosing meniscal tears. MRI accurately delineates tear morphology (horizontal, longitudinal, radial, root, or bucket-handle) and assesses the integrity of the cruciate ligaments.
Surgical Positioning and Setup
Arthroscopic meniscal surgery requires meticulous setup to ensure adequate visualization and compartment access.
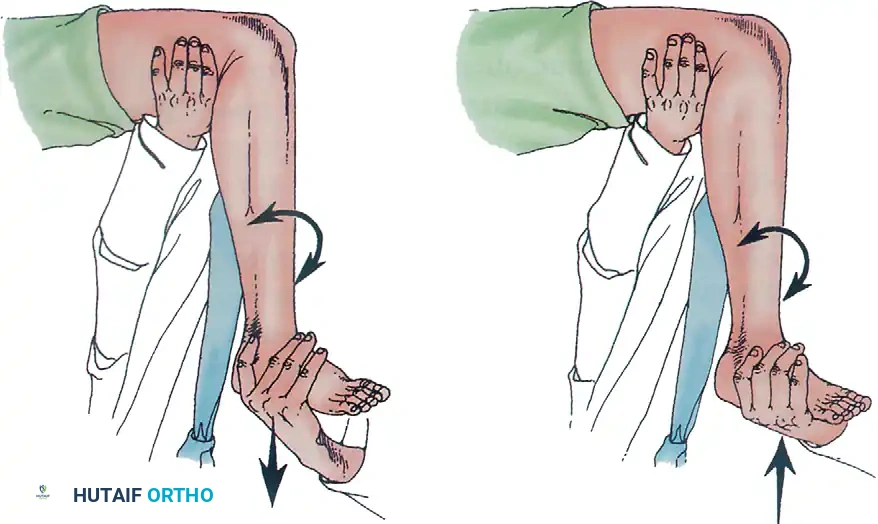
1. Positioning: The patient is placed supine. A lateral post or a circumferential leg holder is applied to the proximal thigh. The foot of the bed is dropped to allow the knee to hang at 90 degrees of flexion.
2. Tourniquet: A pneumatic tourniquet is placed proximally but is often left uninflated unless visualization is compromised by bleeding.
3. Portals: Standard anterolateral (viewing) and anteromedial (working) portals are established adjacent to the patellar tendon. Accessory portals (far medial, far lateral, or posteromedial) may be required for complex repairs.
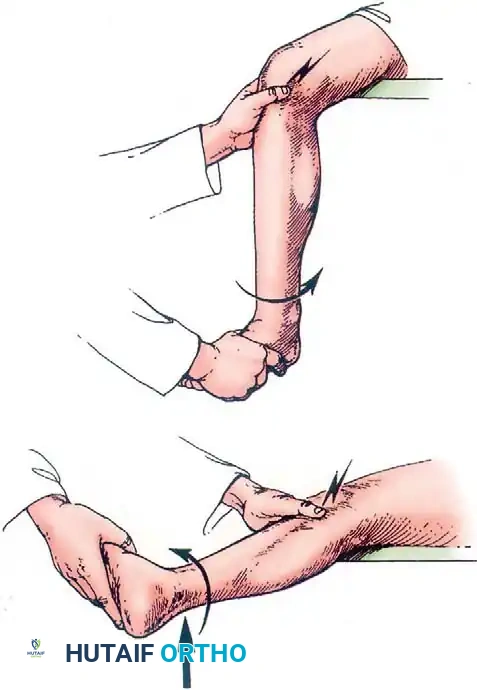
Valgus stress with the knee in slight flexion opens the medial compartment, while the "figure-of-four" position (hip flexed, abducted, externally rotated with varus stress) opens the lateral compartment.
Operative Techniques: Partial Meniscectomy
Indications
Partial meniscectomy is indicated for symptomatic tears in the avascular white-white zone, complex degenerative tears that are not amenable to repair, or in patients who cannot comply with postoperative repair protocols.
Surgical Steps
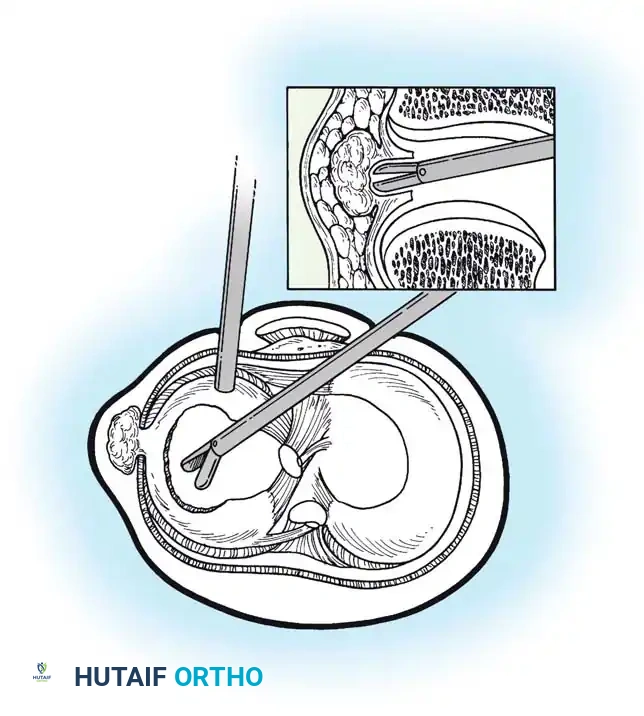
- Probing: Thoroughly probe the meniscus to define the tear pattern and assess stability.
- Resection: Use arthroscopic biters (punches) to resect the mobile, unstable fragments.
- Contouring: The goal is to create a smooth, stable transition zone between the resected area and the intact meniscus. Avoid leaving sharp corners that can act as stress risers.
- Preservation: Resect only the unstable tissue. Preservation of the peripheral rim is critical to maintain hoop tension.
Pitfall: Over-resection of the meniscus, particularly the lateral meniscus, guarantees accelerated chondrolysis. Always adhere to the principle of "maximum preservation."
Operative Techniques: Meniscal Repair
Indications
Repair is strongly indicated for longitudinal tears in the red-red or red-white zones, particularly in young, active patients, and especially when performed concurrently with ACL reconstruction (which enhances the biological healing environment via hemarthrosis).
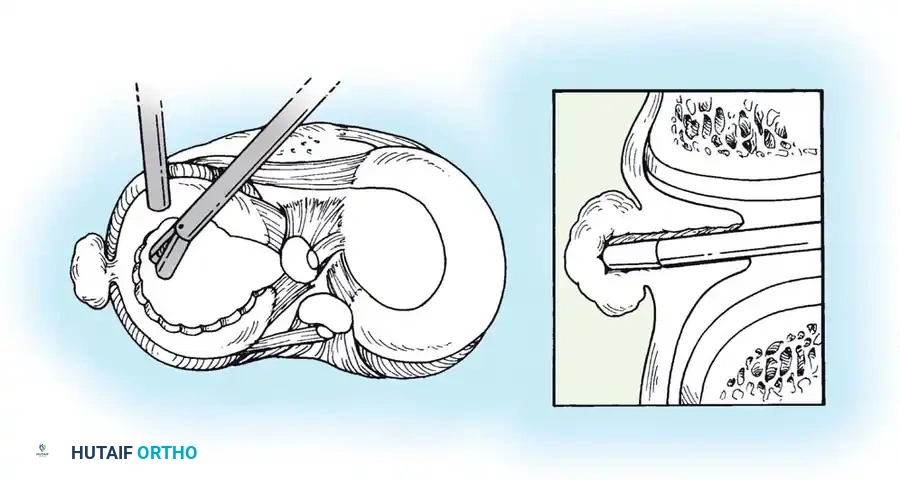
Preparation of the Tear
Healing requires a vascular response. The torn edges must be debrided of degenerative tissue using a motorized shaver or arthroscopic rasp to expose bleeding, healthy fibrocartilage. Trephination (punching small holes from the vascular periphery into the tear) or the introduction of a fibrin clot can augment healing in the red-white zone.
Repair Techniques
1. Inside-Out Technique:
Considered the gold standard for middle-third and posterior-third tears.
* Cannulas are passed through the anterior portals.
* Long, flexible needles carrying non-absorbable sutures are passed across the tear and out through the joint capsule.
* A posterior safety incision is made to retrieve the needles and tie the sutures directly over the capsule, protecting the saphenous nerve (medially) or peroneal nerve (laterally).
2. Outside-In Technique:
Ideal for anterior horn tears. Spinal needles are passed from the outside of the knee, through the capsule and meniscus, into the joint. Sutures are shuttled and tied over the capsule.
3. All-Inside Technique:
Utilizes specialized deployment devices (e.g., FasT-Fix) to place anchors behind the capsule, connected by a sliding knot. This avoids posterior incisions and is highly efficient for posterior horn tears.

Advanced Techniques: Meniscal Root Repair
Meniscal root tears (avulsions of the meniscal attachment to the tibial plateau) completely disrupt hoop tension, leading to rapid meniscal extrusion and catastrophic joint overloading.
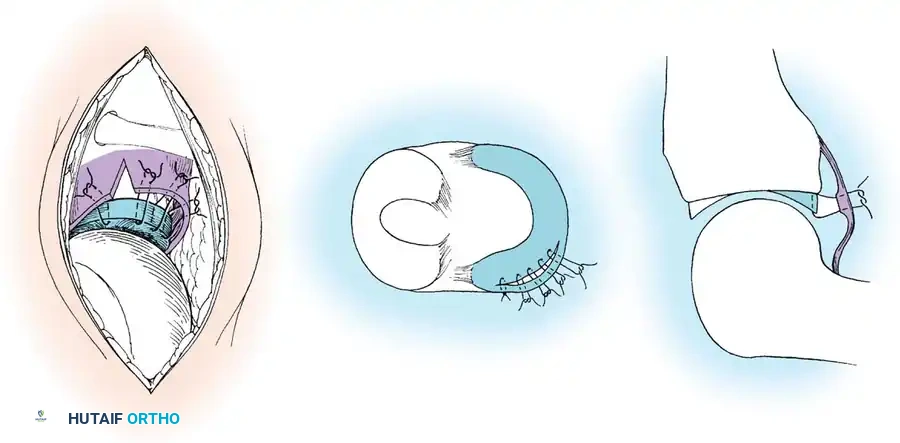
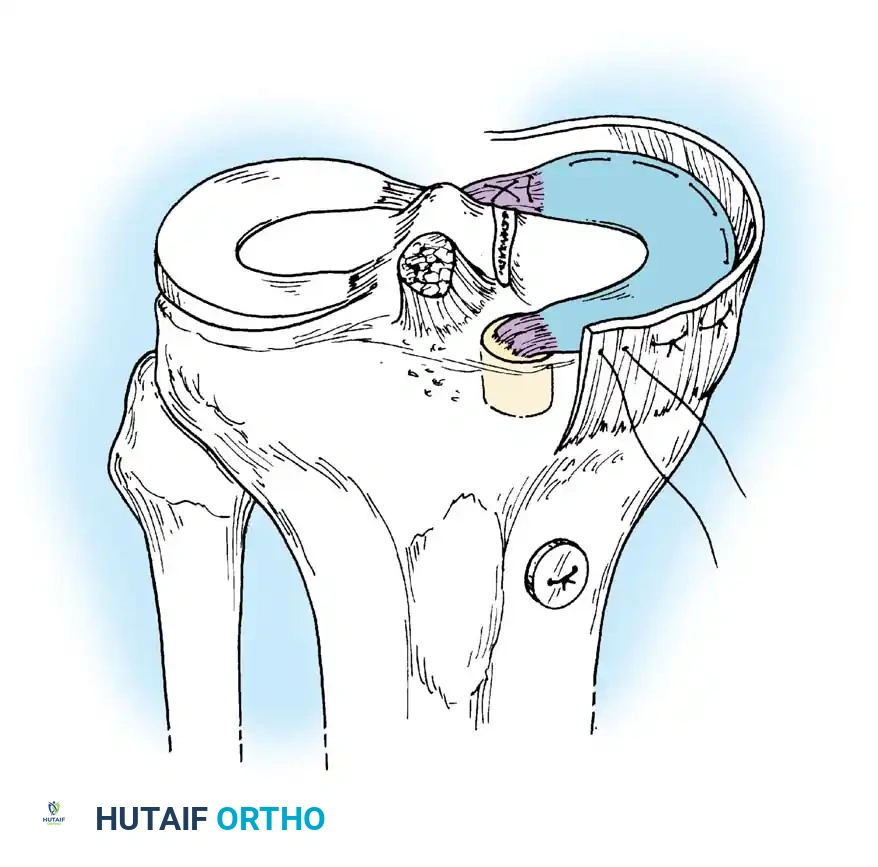
Transtibial Pull-Out Repair
- Debridement: The anatomic footprint of the root is decorticated to a bleeding bone bed using a shaver or curette.
- Suture Passing: Heavy, non-absorbable tapes are passed through the detached meniscal root using a specialized suture-passing device.
- Tunnel Creation: A tibial aiming guide is used to drill a tunnel from the anteromedial tibia to the anatomic root footprint.
- Fixation: The sutures are shuttled down the tibial tunnel and tied over a cortical button or secured with a bio-tenodesis screw on the anterior tibia.
Postoperative healing of the root to the bony footprint restores hoop tension and prevents meniscal extrusion, halting the rapid progression to osteoarthritis.
Postoperative Protocols and Rehabilitation
Following Partial Meniscectomy
- Weight-Bearing: Immediate weight-bearing as tolerated.
- Range of Motion (ROM): Immediate full ROM.
- Return to Sport: Typically
📚 Medical References
- meniscal surgery, Arthroscopy 9:33, 1993.
- Ngo IU, Hamilton WG, Wichern WA, et al: Local anesthesia with sedation for arthroscopic surgery of the knee, Arthroscopy 1:237, 1985.
- Nole R, Munson NM, Fulkerson JP: Bupivacaine and saline effects on articular cartilage, Arthroscopy 1:123, 1985.
- Northmore-Ball MD, Dandy DJ: Long-term results of arthroscopic partial meniscectomy, Clin Orthop Relat Res 167:34, 1982.
- Northmore-Ball MD, Dandy DJ, Jackson RW: Arthroscopic, open partial, and total meniscectomy: a comparative study, J Bone Joint Surg 65B:400, 1983.
- Novak PJ, Bach BR: Selection criteria for knee arthroscopy in the osteoarthritic patient, Orthop Rev 7:798, 1993.
- Noyes FR, Barber-Westin SD: Irradiated meniscus allografts in the human knee: a twoto fi ve-year follow-up study. Paper presented at the Arthroscopy Association of North America Specialty Day, Orlando, Fla, Feb 1995.
- Noyes FR, Barber-Westin SD: Revision anterior cruciate ligament surgery: experience from Cincinnati, Clin Orthop Relat Res 325:116, 1996.
- Noyes FR, Barber-Westin S: Posterior cruciate ligament replacement with a two-strand quadriceps tendon-patellar bone autograft and a tibial inlay technique, J Bone Joint Surg 87A:1241, 2005.
- Noyes FR, Barber-Westin SD: Posterior cruciate ligament revision reconstruction, part 1: causes of surgical failure in 52 consecutive operations, Am J Sports Med 33:646, 2005.
- Noyes FR, Barber-Westin SD: Posterior cruciate ligament revision reconstruction, part 2: results of revision using a 2-strand quadriceps tendon-patellar bone autograft, Am J Sports Med 33:655, 2005.
- Noyes FR, Barber-Westin SD, Butler DL, et al: The role of allografts in repair and reconstruction of knee joint ligaments and menisci, Instr Course Lect 47:379, 1998.
- Noyes FR, Barber-Westin SD, Rankin M: Meniscal transplantation in symptomatic patients less than fi fty years old, J Bone Joint Surg 86A:1392, 2004.
- Noyes FR, Bassett RW, Grood ES, et al: Arthroscopy in acute traumatic hemarthrosis of the knee: incidence of anterior cruciate tears and other injuries, J Bone Joint Surg 62A:687, 1980.
- Noyes FR, Spievack ES: Extraarticular fl uid dissection in tissues during arthroscopy: a report of clinical cases and a study of intraarticular and thigh pressures in cadavers, Am J Sports Med 10:346, 1982.
- O’Connor RL: Arthroscopy in the diagnosis and treatment of acute ligament injuries of the knee, J Bone Joint Surg 56A:333, 1974.
- O’Connor RL: Arthroscopy of the knee, Surg Annu 9:265, 1977.
- Ogilvie-Harris DJ, Basinski A: Arthroscopic synovectomy of the knee for rheumatoid arthritis, Arthroscopy 7:91, 1991.
- Ogilvie-Harris DJ, Biggs DJ, Mackay M, et al: Posterior portals for arthroscopic surgery of the knee, Arthroscopy 10:608, 1994.
- Ogilvie-Harris DJ, Giddens J: Hoffa’s disease: arthroscopic resection of the infrapatellar fat pad, Arthroscopy 10:184, 1994.
- Ogilvie-Harris DJ, Weisleder L: Arthroscopic synovectomy of the knee: is it helpful? Arthroscopy 11:91, 1995.
- Ohkoshi Y, Takeuchi T, Inoue C, et al: Arthroscopic studies of variants of the anterior horn of the medial meniscus, Arthroscopy 13:725, 1997.
- O’Neill DB, Micheli LJ, Warner JP: Patellofemoral stress: a prospective analysis of exercise treatment in adolescents and adults, Am J Sports Med 20:151, 1992.
- Outerbridge HK, Outerbridge AR, Outerbridge RE: The use of a lateral patellar autologous graft for the repair of a large osteochondral defect in the knee, J Bone Joint Surg 77A:65, 1995.
- Patel D: Proximal approaches to arthroscopic surgery of the knee, Am J Sports Med 9:296, 1981.
- Patel D: Superior lateral-medial approach to arthroscopic meniscectomy, Orthop Clin North Am 13:299, 1982.
- Paulos LE, Wnorowski C, Greenwald AE: Infrapatellar contracture syndrome: diagnosis, treatment, and long-term follow-up, Am J Sports Med 22:440, 1994.
- Pellacci F, Montanari G, Prosperi P, et al: Lateral discoid meniscus: treatment and results, Arthroscopy 8:526, 1992.
- Peters TA, McLean ID: Osteochondritis dissecans of the patellofemoral joint, Am J Sports Med 28:63, 2000.
- Petersen W, Lenschow S, Weimann A, et al: Importance of femoral tunnel placement in double-bundle posterior cruciate ligament reconstruction, Am J Sports Med 34:456, 2006.
- Peterson L, Minas T, Brittberg M, et al: Twoto nine-year outcome after autologous chondrocyte transplantation of the knee, Clin Orthop Relat Res 374:212, 2000.
- Pettrone FA: Meniscectomy: arthrotomy versus arthroscopy, Am J Sports Med 10:355, 1982.
- Phillips BB, Cain LE, Dlabach JA: Correlation of interference screw insertion torque with depth of placement in tibial tunnel using quadrupled hamstring graft. Paper presented at the Southern Orthopaedic Annual Meeting, S. Hamilton, Bermuda, 1998.
- Port J, Simon TM, Jackson DW: Preparation of an exogenous fi brin clot, Arthroscopy 11:332, 1995.
- Race A, Amis AA: The mechanical properties of the two bundles of the human posterior cruciate ligaments, J Biomech 27:13, 1994.
- Rath E, Richmond JC, Yassir W, et al: Meniscal allograft transplantation: twoto eight-year results, Am J Sports Med 29:410, 2001.
- Rodeo SA: Arthroscopic meniscal repair with use of the outsidein technique, Instr Course Lect 49:195, 2000.
- Rodeo SA, Seneviratne A, Suzuki K, et al: Histological analysis of human meniscal allografts: a preliminary report, J Bone Joint Surg 82A:1071, 2000.
- Rodeo SA, Warren RF: Meniscal repair using the outside-toinside technique, Clin Sports Med 15:469, 1996.
- Rokito AS, Kvitne RS, Lee MR, et al: Long-term results following meniscal repair. Paper presented at the Arthroscopy Association of North America Specialty Day, Orlando, Fla, Feb 1995.
- Rosenberg TD: Technique for rear entry ACL guide, Miami, Fla, 1988, Acufex Microsurgical. Rosenberg TD: Techniques for endoscope method of ACL reconstruction, Miami, Fla, 1989, Acufex Microsurgical. Rosenberg TD: Revision of failed ACL reconstruction with semitendinosus autograft. Paper presented at the Arthroscopy Association of North America Specialty Day, Orlando, Fla, Feb 1995.
- Rosenberg TD, Graf B: Techniques for ACL reconstruction with Multi-Track drill guide, Miami, Fla, 1994, Acufex Microsurgical. Rosenberg TD, Scott SM, Coward DB, et al: Arthroscopic meniscal repair evaluated with repeat arthroscopy, Arthroscopy 2:14, 1986.
- Rosenberg TD, Scott S, Paulos L: Arthroscopic surgery: repair of peripheral detachment of the meniscus, Contemp Orthop 10:43, 1985.
- Rosenberg TD, Wong HC: Arthroscopic knee surgery in a freestanding outpatient surgery center, Orthop Clin North Am 13:277, 1982.
- Rubman MH, Noyes FR, Barber-Westin SD: Arthroscopic repair of meniscal tears that extend into the avascular zone: a review of 198 single and complex tears, Am J Sports Med 26:87, 1998.
- Ryu KN, Kim IS, Kim EJ, et al: MR imaging of tears of discoid lateral menisci, AJR Am J Roentgenol 171:963, 1998.
- Sagastibelza J, Zuniga JJR, Blasco JJL, et al: Case report: osteochondritis dissecans of the anterior tibial spine, Arthroscopy 9:695, 1993.
- Scheller G, Sobau C, Bulow JU: Arthroscopic partial lateral meniscectomy in an otherwise normal knee: clinical, functional, and radiographic results of a long-term follow-up study, Arthroscopy 17:946, 2001.
- Schimmer RC, Brulhart KB, Duff C, et al: Arthroscopic partial meniscectomy: a 12-year follow-up and two-step evaluation of the long-term course, Arthroscopy 14:136, 1998.
- Schonholtz GJ: Arthroscopy and arthroscopic surgery, Md State Med J 30:56, 1981.
- Schonholtz GJ, Zahn MG, Magee CM:
You Might Also Like
