Mastering Posterior Cruciate Ligament Reconstruction: BPTB and Achilles Tendon Grafts
Key Takeaway
Posterior cruciate ligament (PCL) reconstruction using bone-patellar tendon-bone (BPTB) or Achilles tendon-bone grafts requires meticulous surgical precision. This comprehensive guide details the open posterior approach, highlighting critical neurovascular anatomy, isometric tunnel placement, and graft tensioning. By mastering these advanced techniques and understanding potential complications like motion loss and popliteal artery injury, orthopedic surgeons can optimize biomechanical stability and clinical outcomes in complex knee ligament reconstructions.
INTRODUCTION TO POSTERIOR CRUCIATE LIGAMENT RECONSTRUCTION
The posterior cruciate ligament (PCL) is the primary restraint to posterior tibial translation, providing critical biomechanical stability to the knee joint throughout its arc of motion. Injuries to the PCL, while less common than anterior cruciate ligament (ACL) tears, often result from high-energy trauma such as dashboard injuries or severe hyperflexion events. When conservative management fails, or in the setting of multiligamentous knee injuries, surgical reconstruction becomes imperative to restore joint kinematics and prevent early-onset osteoarthritis.
Reconstruction of the PCL utilizing bone-patellar tendon-bone (BPTB) autografts or allografts, as well as Achilles tendon-bone allografts, represents a gold-standard approach for achieving robust, rigid fixation. These grafts are favored for their high ultimate tensile strength and the biomechanical advantage of bone-to-bone healing within the osseous tunnels. This comprehensive surgical guide details the open posterior approach as described by Burks and Schaffer, elucidating the critical steps, anatomical considerations, and complication management necessary for successful PCL reconstruction.
SURGICAL ANATOMY AND BIOMECHANICS
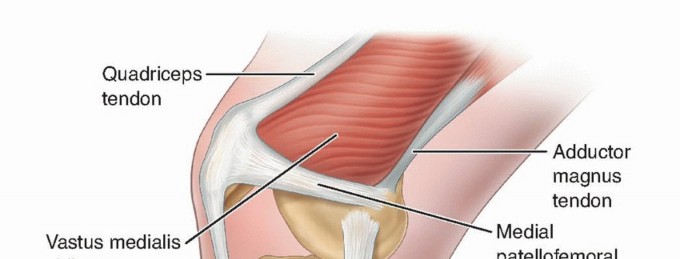
A profound understanding of PCL anatomy is non-negotiable for the operating surgeon. The PCL originates from the anterolateral aspect of the medial femoral condyle and inserts onto the posterior tibial sulcus, approximately 1 to 1.5 cm distal to the joint line.
The ligament is composed of two primary functional bundles:
* Anterolateral (AL) Bundle: The larger and stiffer of the two, the AL bundle is tightest in knee flexion and serves as the primary restraint to posterior tibial translation at 90 degrees of flexion.
* Posteromedial (PM) Bundle: Smaller in cross-sectional area, the PM bundle is tightest in full extension and deep flexion, providing secondary restraint.
💡 Clinical Pearl: Isometric Graft Placement
True isometry in PCL reconstruction is virtually impossible due to the broad anatomical footprint of the native ligament. However, achieving a "near-isometric" placement is critical. The position of the femoral tunnel dictates graft tension throughout the range of motion. Deviations of even a few millimeters can result in catastrophic graft failure or severe loss of motion.
GRAFT SELECTION RATIONALE
The choice between BPTB and Achilles tendon-bone grafts depends on patient-specific factors, surgeon preference, and the presence of multiligamentous injuries.
Bone-Patellar Tendon-Bone (BPTB) Grafts
BPTB grafts (autograft or allograft) offer excellent structural integrity. The native patellar tendon has an ultimate tensile strength of approximately 2,900 N, which closely mimics the native PCL. The presence of bone blocks at both ends allows for rigid aperture fixation using interference screws, promoting rapid osteointegration and allowing for accelerated rehabilitation.
Achilles Tendon-Bone Grafts
Achilles allografts provide a massive collagenous cross-section, offering superior tensile strength. The calcaneal bone block is typically utilized for the femoral tunnel, providing rigid fixation at the critical isometric point, while the robust soft-tissue tail is passed through the tibial tunnel. This allows for a larger graft diameter to fill the tibial footprint, which is anatomically broader than the femoral origin.
⚠️ Surgical Warning: Suboptimal Graft Choices
Poor graft selection has been heavily implicated in the failure of PCL reconstructions. Tissues such as the iliotibial band, the medial head of the gastrocnemius, or standard hamstring tendons often possess insufficient biomechanical strength to prevent posterior sag and drawer over time. These softer, more elastic grafts are prone to creep and elongation under the constant posterior gravitational and muscular forces exerted on the tibia.
PREOPERATIVE PLANNING AND PATIENT POSITIONING
Meticulous preoperative planning includes a thorough clinical examination (posterior drawer, dial test, external rotation recurvatum test) to rule out concurrent posterolateral corner (PLC) injuries. High-resolution MRI is mandatory to assess the exact location of the PCL tear and evaluate the menisci and chondral surfaces.
Positioning Setup
- Anesthesia: General anesthesia with complete neuromuscular blockade is required to eliminate muscle spasms and facilitate posterior translation of the tibia during reduction.
- Positioning: The patient is placed in the prone position. All bony prominences must be meticulously padded to prevent pressure necrosis.
- Tourniquet: A high-thigh pneumatic tourniquet is applied.
- Preparation: The operative leg is prepped and draped free to allow full range of motion during the procedure.
SURGICAL TECHNIQUE: THE POSTERIOR APPROACH (BURKS AND SCHAFFER)
The open posterior approach provides direct, unparalleled visualization of the tibial footprint of the PCL, minimizing the risk of iatrogenic neurovascular injury compared to blind arthroscopic transtibial drilling.
Step 1: Incision and Superficial Dissection
With the patient prone, make a gently curved incision. The incision should feature a horizontal limb located near the flexion crease of the knee to prevent postoperative scar contracture, extending distally and laterally.
Incise the skin and subcutaneous tissues down to the popliteal fascia. Care must be taken to identify and protect the lesser saphenous vein and the medial sural cutaneous nerve, which typically lie in the midline of the distal popliteal fossa.
Step 2: Deep Dissection and Neurovascular Protection
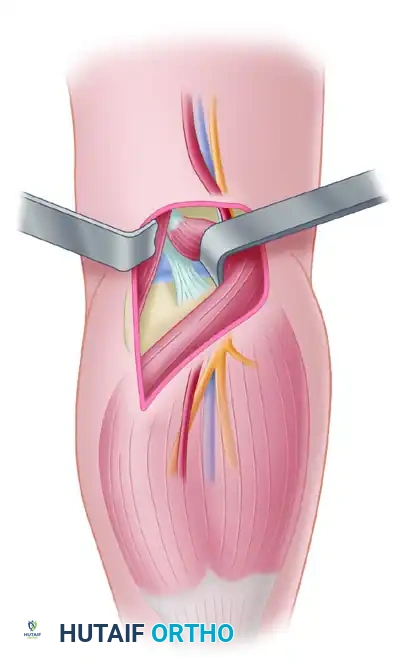
Incise the popliteal fascia. The key to this approach is navigating the interval between the medial head of the gastrocnemius and the semimembranosus muscle.
Retract the semimembranosus medially and the medial head of the gastrocnemius laterally. This retraction protects the critical neurovascular bundle, which is mobilized laterally with the gastrocnemius.

As demonstrated in the deep dissection, the popliteal artery and vein, along with the tibial nerve, lie directly posterior to the joint capsule. The peroneal nerve courses further laterally.
🚨 Surgical Pitfall: Neurovascular Proximity
The popliteal artery is tethered at the adductor hiatus proximally and the soleal arch distally, making it highly susceptible to traction injury or direct laceration. Always maintain direct visualization of the posterior capsule and utilize blunt retractors (such as a posterior cruciate retractor) to shield the neurovascular bundle during all drilling and debridement steps.
Step 3: Preparation of the Tibial Tunnel
- Capsulotomy: Perform a vertical capsulotomy to expose the posterior aspect of the tibial plateau and the PCL facet.
- Footprint Preparation: Excise the remnants of the native PCL using a combination of electrocautery and pituitary rongeurs. Elevate the periosteum slightly distal to the joint line to identify the anatomical insertion site.
- Guide Pin Placement: Place a tibial aiming guide. The pin should exit at the distal and lateral aspect of the native PCL footprint.
- Drilling: Over-drill the guide pin with a reamer matched to the diameter of the graft's bone block. Crucial Step: The tip of the guide pin and the reamer must be viewed directly at all times to prevent penetration into the popliteal fossa.
Step 4: Preparation of the Femoral Tunnel
The femoral tunnel is typically prepared from an inside-out or outside-in approach, targeting the anterolateral bundle footprint on the medial femoral condyle.
1. Identify the articular margin of the medial femoral condyle.
2. The center of the femoral tunnel should be placed approximately 8 to 10 mm proximal to the articular cartilage margin, at the 1 o'clock (right knee) or 11 o'clock (left knee) position.
3. Drill the guide pin and subsequent reamer, ensuring the tunnel length is sufficient to accommodate the bone plug.
Step 5: Graft Passage and Fixation
- Pass the graft into the joint. If using an Achilles allograft, the bone block is typically secured in the femoral tunnel first using a titanium or bioabsorbable interference screw.
- Pass the soft tissue tail (or the second bone block of a BPTB graft) into the tibial tunnel.
- Tensioning: Reduce the tibia to its neutral anatomical position (restoring the normal anterior step-off of the medial tibial plateau). Cycle the knee through a full range of motion 15 to 20 times to remove creep from the graft.
- Fix the tibial side with an interference screw or a cortical suspensory device while applying an anterior drawer force to the tibia with the knee flexed at 90 degrees.
ARTHROSCOPICALLY AIDED POSTERIOR CRUCIATE LIGAMENT RECONSTRUCTION
As described extensively in the literature regarding anterior cruciate ligament reconstruction, the posterior cruciate ligament also can be replaced utilizing entirely arthroscopic or arthroscopically-assisted surgical techniques. These techniques rely on specialized trans-septal portals and angled instrumentation to view the posterior tibial facet. While arthroscopic techniques reduce surgical morbidity and incision size, they demand a steep learning curve and rely heavily on fluoroscopic imaging to ensure the guide pin does not violate the posterior neurovascular structures.
COMPLICATIONS OF POSTERIOR CRUCIATE LIGAMENT RECONSTRUCTION
PCL reconstruction is a technically demanding procedure with a unique complication profile. Aside from the usual postoperative complications (infection, DVT, hematoma), the surgeon must be acutely aware of the following specific issues.
1. Loss of Motion (Arthrofibrosis)
The most common problem associated with posterior cruciate ligament reconstruction is loss of motion. Clinically, flexion loss is significantly more common than extension loss. Many studies report between 10 and 20 degrees of permanent flexion loss.
Etiology of Motion Loss:
* Improper Graft Placement: The position of the femoral tunnel is far more critical than that of the tibial tunnel. Femoral attachments placed anterior and distal to the most isometric region result in exponentially increased graft tension as the knee flexes. This flexion loss results directly from an abnormal increase in the distance between the femoral and tibial attachment sites during the arc of motion.
* Inadequate Rehabilitation: Failure to initiate early, controlled passive range of motion.
* Prolonged Immobilization: Loss of extension or the development of a flexion contracture most likely is caused by prolonged immobilization of the knee in a flexed position postoperatively.
2. Failure to Obtain Objective Stability
Recurrent posterior sag and positive posterior drawer tests indicate a failure of the reconstruction.
Etiology of Instability:
* Poor Graft Selection: As previously noted, the use of the iliotibial band, the medial head of the gastrocnemius, or standard hamstring tendons often leads to failure. These tissues simply have insufficient tensile strength to prevent posterior sag and drawer over the long term.
* Improper Tunnel Placement: Femoral tunnel placement posterior and proximal to the most isometric region results in decreased graft tension in flexion. This occurs secondary to a decrease in the distance between the femoral and tibial attachment sites as the knee bends. This results in immediate graft laxity and an inability to prevent posterior sag. Furthermore, non-anatomical tunnel placement can result in severe graft abrasion against the condylar walls, leading to subsequent mechanical failure and rupture.
* Untreated Associated Injuries: Failure of the reconstruction may frequently be the result of untreated associated ligamentous injuries. Missed injuries to the posterolateral corner (PLC) are the most common culprits. A deficient PLC allows excessive external rotation and posterior translation forces to be applied directly to the PCL graft, leading to rapid elongation and failure.
3. Neurological Injuries
Neurological complications can be devastating and require meticulous surgical technique to avoid.
* Neurapraxia: Can result from excessive tourniquet time or excessive traction on the neurovascular bundle during lateral retraction of the gastrocnemius.
* Direct Tibial Nerve Injury: Direct injury to the tibial nerve can result from penetration by either the tibial guide pin or the reamer. This catastrophic complication can be entirely avoided by ensuring direct, visual exposure of the tip of the pin and drill during the preparation of the tibial tunnel.
4. Vascular Complications
Vascular complications include laceration, thrombosis, and intimal injury to the popliteal artery. Because the popliteal artery lies immediately posterior to the posterior capsule, blind drilling is strictly contraindicated. Viewing the tip of the guide pin and reamer at all times, combined with the use of a protective posterior retractor, can prevent this limb-threatening injury.
5. Osteonecrosis of the Medial Femoral Condyle
Osteonecrosis (avascular necrosis) of the medial femoral condyle has been reported following PCL reconstruction.
* Presentation: It may occur months to years after the index surgery, presenting as insidious onset medial joint line pain.
* Pathophysiology: The cause is thought to be local iatrogenic trauma to the delicate blood supply of the subchondral bone. This vascular insult stems from a combination of extensive soft tissue dissection around the medial epicondyle and the thermal/mechanical trauma of drilling the large femoral condyle tunnel.
* Management: This complication has been treated successfully with surgical curettage of the necrotic bone and autogenous bone grafting of the defect, often requiring a period of protected weight-bearing.
POSTOPERATIVE REHABILITATION PROTOCOL
Rehabilitation following PCL reconstruction is generally more conservative than ACL rehabilitation due to the constant posterior gravitational forces acting on the tibia.
- Phase I (0-6 Weeks): The knee is locked in full extension in a dynamic PCL brace (which applies an anterior force to the posterior calf). Weight-bearing is typically restricted to toe-touch or partial weight-bearing. Passive prone flexion is initiated slowly, strictly avoiding active hamstring contraction, which pulls the tibia posteriorly and stresses the graft.
- Phase II (6-12 Weeks): Progression to full weight-bearing. The brace is unlocked for ambulation. Active quadriceps strengthening (closed kinetic chain) is emphasized to provide dynamic anterior translation of the tibia, protecting the PCL graft.
- Phase III (3-6 Months): Introduction of light jogging, proprioceptive training, and gradual introduction of isolated hamstring strengthening.
- Phase IV (6-9+ Months): Return to sport-specific activities and multidirectional agility drills, contingent upon achieving >90% limb symmetry index on functional testing and a stable posterior drawer exam.
You Might Also Like