Posterior Cruciate Ligament: Anatomy, Biomechanics & Surgery
Key Takeaway
The posterior cruciate ligament (PCL) is the primary restraint to posterior tibial translation. Comprising the anterolateral and posteromedial bundles, it dictates knee kinematics and the screw-home mechanism. Surgical management requires precise anatomic tunnel placement and robust graft fixation. This guide details PCL anatomy, biomechanical properties, step-by-step operative reconstruction techniques, and critical considerations for cruciate ligament revision surgery to optimize patient outcomes.
INTRODUCTION TO THE POSTERIOR CRUCIATE LIGAMENT
The posterior cruciate ligament (PCL) is a robust, intra-articular, extrasynovial structure that serves as the primary stabilizer of the knee against posterior tibial translation. Recognized as the central axis of knee rotation, the PCL is integral to normal knee kinematics, including the complex "screw-home" mechanism. Due to its intrinsic strength and complex multifascicular anatomy, injuries to the PCL are less common than those to the anterior cruciate ligament (ACL) but present significant challenges in both conservative and operative management.
This comprehensive masterclass delineates the advanced surgical anatomy, biomechanical properties, clinical evaluation, and step-by-step operative reconstruction of the PCL, alongside critical principles for cruciate ligament revision surgery.
SURGICAL ANATOMY
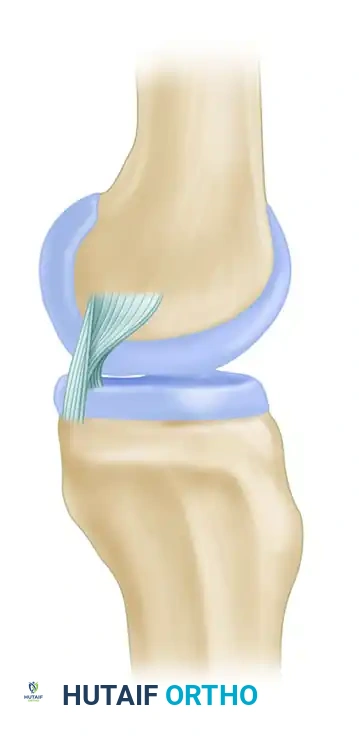
The posterior cruciate ligament is the largest and strongest ligament in the human knee. It is composed of two major functional components: a large anterior portion (the anterolateral bundle) that forms the bulk of the ligament, and a smaller posterior portion (the posteromedial bundle) that runs obliquely to the back of the tibia.
Femoral Attachment
The PCL attaches proximally to the posterior part of the lateral surface of the medial femoral condyle. Like the ACL, it forms a segment of a circle. The anatomic footprint is expansive, typically measuring approximately 32 mm in length and 23 mm in width. The proximal boundary of the femoral footprint is located roughly 3 mm from the articular cartilage margin, while the distal boundary sits approximately 5 mm from the articular edge, aligning closely with the level of the adductor tubercle.
Surgical Warning: Failure to respect the expansive 32 mm × 23 mm femoral footprint during tunnel preparation is a primary cause of graft failure. The insertion sites are 300% to 500% larger than the cross-section of the midsubstance, necessitating precise anatomic graft placement to replicate native kinematics.
Tibial Attachment
The tibial attachment is situated in a distinct depression behind and below the intra-articular portion of the tibia (the posterior tibial facet). This insertion site extends distally over the posterior aspect of the tibia, with a fascial slip usually blending with the posterior horn of the lateral meniscus.
Meniscofemoral Ligaments
The meniscofemoral ligaments (MFLs) are critical accessory structures of the PCL complex. They arise from the posterior horn of the lateral meniscus and insert onto the lateral aspect of the medial femoral condyle.
* Ligament of Humphry: Passes anterior to the PCL.
* Ligament of Wrisberg: Passes posterior to the PCL.
Harner et al. extensively measured the cross-sectional shape and area of the ACL, PCL, and MFLs in cadaveric studies. They demonstrated that the PCL increases in cross-sectional area from the tibia to the femur. Specifically, the PCL is approximately 50% larger than the ACL at the femoral insertion and 20% larger at the tibial insertion. The meniscofemoral ligaments average approximately 22% of the entire cross-sectional area of the PCL, highlighting their significant contribution to posterior knee stability.
BIOMECHANICS AND KINEMATICS
The PCL is more vertically than obliquely oriented and serves as the central axis around which rotation of the knee occurs. It is the primary restraint to posterior tibial translation, accounting for 89% of the resistance to posterior translation of the tibia on the femur at 90 degrees of flexion.
Bundle Tensioning Patterns
The two bundles of the PCL exhibit distinct tensioning patterns throughout the knee's range of motion:
* Anterolateral (AL) Bundle: This larger component tightens in flexion and becomes lax in extension. Biomechanical evaluations reveal that the AL component possesses significantly greater linear stiffness and ultimate load to failure than both the posteromedial component and the meniscofemoral ligaments.
* Posteromedial (PM) Bundle: This smaller band tightens in extension and becomes lax in deep flexion.
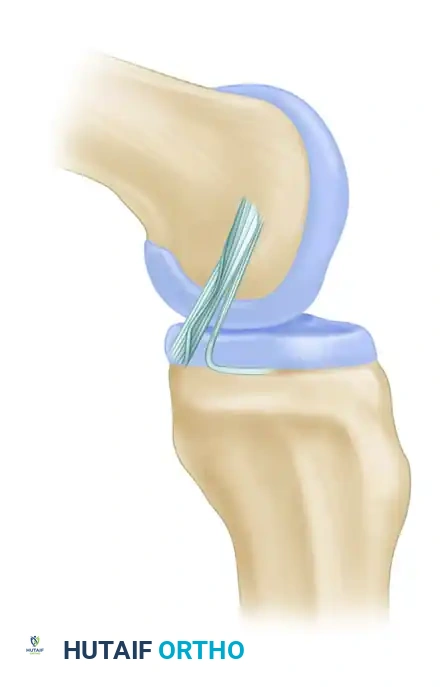
As the knee transitions from extension to flexion, there is a dynamic change in the shape and tension of the PCL components. With flexion, there is a tightening of the bulk of the ligament (the AL bundle), but less tension is placed on the smaller PM band.
Rotational Stability and the Screw-Home Mechanism
The PCL appears to guide the "screw-home" mechanism—the obligatory internal rotation of the femur on the tibia during terminal extension of the knee. Selective cutting studies of the PCL demonstrate its critical role in flexion: when the PCL is sectioned, posterior drawer displacement is markedly increased, with no change in the anterior drawer sign. While rotational stability remains largely unchanged in extension, it is significantly altered in flexion following PCL transection. Furthermore, the PCL acts as a secondary check against hyperextension, but only after the ACL has been ruptured.
CLINICAL EVALUATION AND INDICATIONS FOR SURGERY
Mechanism of Injury
PCL injuries typically occur via a posteriorly directed force on the proximal tibia with the knee flexed (e.g., a "dashboard injury" during a motor vehicle collision or a fall onto a flexed knee with a plantarflexed foot).
Physical Examination
- Posterior Drawer Test: The most accurate clinical test for PCL insufficiency, performed at 90 degrees of knee flexion.
- Posterior Sag Sign (Godfrey's Test): Observation of the tibial tubercle dropping posteriorly relative to the patella when the hips and knees are flexed to 90 degrees.
- Quadriceps Active Test: Contraction of the quadriceps at 90 degrees of flexion causes an anterior shift of the posteriorly subluxated tibia.
- Dial Test: Used to differentiate an isolated PCL injury from a combined PCL and Posterolateral Corner (PLC) injury. Increased external rotation at 90 degrees of flexion (but not at 30 degrees) suggests an isolated PCL injury.
Indications for Operative Management
- Grade III isolated PCL tears (posterior translation > 10 mm) in active, symptomatic patients.
- Combined multiligamentous knee injuries (e.g., PCL + PLC, or PCL + ACL).
- Chronic PCL deficiency with progressive medial compartment or patellofemoral chondrosis.
- Bony avulsion fractures of the PCL tibial insertion (amenable to primary repair).
SURGICAL POSITIONING AND SETUP
Optimal visualization and access to the posterior compartment are mandatory for safe PCL reconstruction.
1. Patient Positioning: The patient is placed supine on the operating table. A lateral post or a specialized leg holder is utilized to allow full range of motion and secure the knee at 90 degrees of flexion.
2. Tourniquet: A proximal thigh tourniquet is applied but inflated only if necessary to maintain a bloodless field.
3. Fluoroscopy: An image intensifier should be available to confirm the precise placement of the tibial and femoral guide pins, ensuring anatomic tunnel trajectories.
4. Portal Placement:
* Standard anterolateral (viewing) and anteromedial (working) portals.
* Posteromedial Portal: Absolutely critical for PCL reconstruction. It allows direct visualization of the tibial footprint, safe elevation of the posterior capsule, and protection of the popliteal neurovascular bundle.
Clinical Pearl: When establishing the posteromedial portal, the knee should be flexed to 90 degrees to allow the saphenous nerve and vein to fall posteriorly. Transilluminate the skin to avoid superficial vessels, and make the incision under direct intra-articular visualization.
STEP-BY-STEP SURGICAL APPROACH: PCL RECONSTRUCTION
1. Graft Selection
Autografts (Bone-Patellar Tendon-Bone, Quad Tendon, or Hamstrings) and allografts (Achilles tendon, Tibialis anterior) are viable options. Achilles tendon allograft is frequently favored for single-bundle reconstructions due to its robust bone block (ideal for femoral fixation) and ample soft tissue length.
2. Tibial Tunnel Preparation (Transtibial Technique)
- Through the posteromedial portal, the posterior capsule is carefully elevated off the posterior tibial facet using a periosteal elevator or radiofrequency wand.
- A PCL tibial guide is introduced through the anteromedial portal and hooked over the posterior facet of the tibia, approximately 7 mm anterior to the posterior tibial cortex.
- The guide pin is drilled from the anteromedial tibia, aiming for the anatomic footprint.
- Fluoroscopic Confirmation: Lateral fluoroscopy must confirm the pin is directed toward the "champagne glass drop-off" of the posterior tibia.
- The tunnel is reamed over the guide pin. A curette is placed over the tip of the guide pin through the posteromedial portal to protect the popliteal artery during reaming.
3. Femoral Tunnel Preparation
- The femoral footprint is identified on the lateral aspect of the medial femoral condyle.
- For a single-bundle reconstruction (targeting the AL bundle), the guide pin is placed 2-3 mm from the articular cartilage margin at the 1 o'clock (right knee) or 11 o'clock (left knee) position.
- The tunnel is reamed to the appropriate depth based on the graft's bone block dimensions.
4. Graft Passage and Fixation
- The graft is typically passed retrogradely from the tibial tunnel into the joint space, then advanced into the femoral tunnel.
- Femoral Fixation: Secured first using an interference screw (metal or bioabsorbable).
- Tibial Fixation: The knee is cycled through a full range of motion. The graft is tensioned with the knee at 90 degrees of flexion while an anterior drawer force is applied to restore the normal tibial step-off. Fixation is achieved with a tibial interference screw, often supplemented with a cortical backup button or staple.
CRUCIATE LIGAMENT REVISION CONSIDERATIONS
While primary reconstructions yield high success rates, revision cruciate surgery presents unique anatomical and biomechanical challenges. The clinical results of revision anterior and posterior cruciate ligament reconstruction are generally not as favorable as those of primary reconstruction. Patients must be appropriately counseled regarding their expectations. The success rate for primary reconstructions is generally reported to be 90% to 95%, compared with 65% to 75% for revisions.
In a series of 63 patients with revision cruciate reconstructions reported by Battaglia et al., approximately 60% were able to return to sports, though most returned at lower levels than before the revision. Furthermore, significant progression of osteoarthritis, despite satisfactory stability and function, was reported by Diamantopoulos et al. at mid-term follow-up of 148 patients undergoing revision surgery.
Hardware Removal and Bone Defect Management
The most frequently cited reason for failure of primary cruciate reconstruction is inappropriate tunnel positioning. Addressing this often requires hardware removal and management of resultant bone voids.
* Synthetic Grafts: Prosthetic ligaments should be removed en bloc to avoid fragmentation of synthetic materials within the joint space.
* Retained Hardware: Femoral or tibial hardware present from a previous two-incision technique, or occasionally from an endoscopic technique, can be left intact depending on its location and whether it interferes with the new anatomic tunnel trajectory.
* Bone Grafting: Screw and graft removal can cause large bony defects, which may require staged or simultaneous bone grafting. A cylinder-shaped graft can be taken from the tibia with a hand-held trephine harvester. Alternatively, bony defects can be filled with oversized absorbable or metal interference screws, which can be stacked adjacent to one another to fill a defect.
* Harner et al. described the use of a large bone block allograft for massive defects. For a posterior wall deficiency, it may be necessary to convert to an over-the-top technique or utilize suspensory cortical fixation (e.g., EndoButton).
Pitfall: A generous revision notchplasty may be indicated in revision scenarios to prevent graft impingement. However, the adequacy of the notchplasty must be meticulously assessed after graft placement to ensure it does not lateralize the femoral footprint or compromise the structural integrity of the condyle.
POSTOPERATIVE REHABILITATION PROTOCOL
Rehabilitation following PCL reconstruction is inherently more conservative than ACL rehabilitation to protect the graft from the posterior pull of gravity and hamstring forces.
- Phase I (0-6 Weeks): The knee is locked in full extension in a dynamic PCL brace (which applies an anterior force to the posterior calf). Weight-bearing is typically restricted to toe-touch or partial weight-bearing. Passive prone flexion is initiated to prevent gravity-assisted posterior tibial subluxation. Active hamstring contraction is strictly prohibited.
- Phase II (6-12 Weeks): Progressive weight-bearing is allowed. Range of motion is gradually advanced. Closed kinetic chain quadriceps strengthening (e.g., leg presses limited to 0-70 degrees) is initiated.
- Phase III (3-6 Months): Discontinuation of the brace. Progression to full range of motion and advanced proprioceptive training.
- Phase IV (6-12 Months): Return to sport-specific activities is permitted only when quadriceps strength reaches >90% of the contralateral limb, and clinical examination demonstrates a stable knee with no posterior sag.
CONCLUSION
The posterior cruciate ligament is a complex, multifascicular structure vital for maintaining posterior and rotational stability of the knee. A profound understanding of its anatomy—specifically the distinct roles of the anterolateral and posteromedial bundles—and its biomechanical properties is essential for accurate diagnosis and successful surgical intervention. Whether performing a primary reconstruction or navigating the complexities of revision surgery, meticulous attention to anatomic footprint restoration, rigid graft fixation, and a disciplined postoperative rehabilitation protocol are paramount to optimizing patient outcomes and restoring knee kinematics.
You Might Also Like

