Mastering the Lateral Approach to the Posterior Talocalcaneal Joint
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Mastering the Lateral Approach to the Posterior Talocalcaneal Joint. The lateral approach to the posterior talocalcaneal joint is a surgical method for arthrodesis, providing extensive exposure of the joint's posterior facet. The patient is positioned supine, and a 10-13 cm curved incision is made on the lateral ankle, following the fibula's posterior border and passing over the peroneal tubercle, mobilizing the peroneal tendons.
Introduction and Epidemiology
The posterior talocalcaneal joint, an integral component of the subtalar joint complex, plays a critical role in hindfoot mechanics, enabling inversion and eversion of the foot and allowing for adaptation to uneven terrain. Pathology affecting this articulation can severely impair ambulation and quality of life. The lateral approach to the posterior talocalcaneal joint is a well-established surgical pathway primarily utilized for procedures requiring extensive exposure of the posterior facet, most notably for arthrodesis in cases of end-stage subtalar arthritis or complex fracture management.
Subtalar arthritis, whether post-traumatic, degenerative, inflammatory, or idiopathic, represents a significant burden. Post-traumatic arthritis following calcaneal or talar fractures is particularly common, often leading to progressive pain, stiffness, and deformity. Epidemiological studies suggest a considerable incidence of subtalar joint involvement in hindfoot pain, with fusion rates for subtalar arthritis demonstrating long-term symptomatic relief and improved function in appropriately selected patients. While arthroscopic techniques and less invasive approaches have emerged, the open lateral approach remains a gold standard for its unparalleled visualization and direct access, particularly in cases requiring substantial debridement, bone grafting, or intricate fixation. This review aims to delineate the anatomical considerations, indications, surgical technique, potential complications, and rehabilitation principles associated with mastering this essential surgical approach.
Surgical Anatomy and Biomechanics
A thorough understanding of the surgical anatomy of the lateral hindfoot is paramount for a safe and effective lateral approach to the posterior talocalcaneal joint. This region is complex, featuring crucial neurovascular structures, musculotendinous units, and intricate bony architecture.
Bony Anatomy
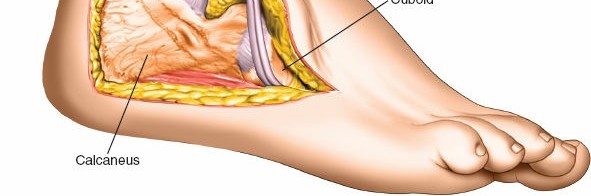
The subtalar joint comprises three facets: anterior, middle, and posterior. The lateral approach specifically targets the posterior facet, which is the largest of the three. It is formed by the concave posterior facet of the talus articulating with the convex posterior facet of the calcaneus. The talus, a unique bone without direct muscular attachments, relies on its ligamentous connections and the forces transmitted from the tibia and calcaneus for stability. The calcaneus, the largest tarsal bone, provides the lever arm for the triceps surae and forms the heel pad. Key lateral bony landmarks include:
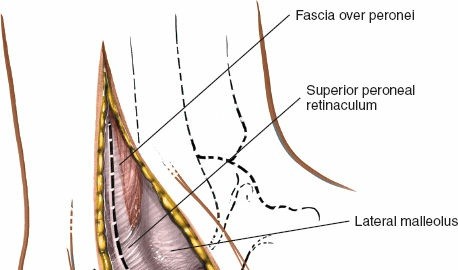
* The lateral malleolus: The distal subcutaneous end of the fibula, forming the lateral border of the ankle mortise.
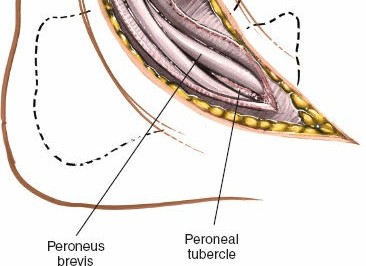
* The peroneal tubercle (trochlear process): A small bony protuberance on the lateral surface of the calcaneus, typically located distal and anterior to the lateral malleolus. It serves as a separator for the tendons of the peroneus longus and brevis muscles.
* The sinus tarsi: A conical cavity located between the talus and calcaneus, anterior to the posterior facet and containing fat, blood vessels, and the critical interosseous and cervical ligaments.
Soft Tissue Anatomy and Neurovascular Structures
The soft tissue envelope of the lateral hindfoot is intricate:
* Skin and subcutaneous tissue: Relatively thin over the lateral malleolus but thicker inferiorly.
* Fascia: Deep fascia encasing the peroneal tendons.
* Musculotendinous structures: The peroneus longus and peroneus brevis muscles lie within the lateral compartment. Their tendons course posterior to the lateral malleolus, with the peroneus brevis typically anterior to the longus. The peroneal tubercle separates these tendons. These tendons are crucial anatomical structures that are retracted anteriorly during the lateral approach.
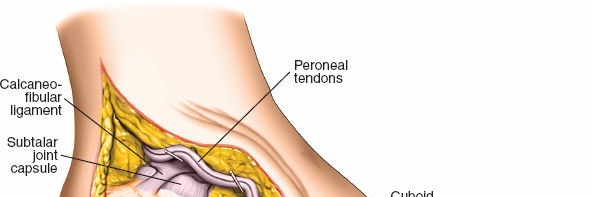
* Ligaments: Key ligaments include the anterior and posterior talofibular ligaments, calcaneofibular ligament (part of the lateral ankle complex), and within the sinus tarsi, the interosseous talocalcaneal ligament and the cervical ligament, which are often disrupted or resected during joint exposure.
* Neurovascular structures:
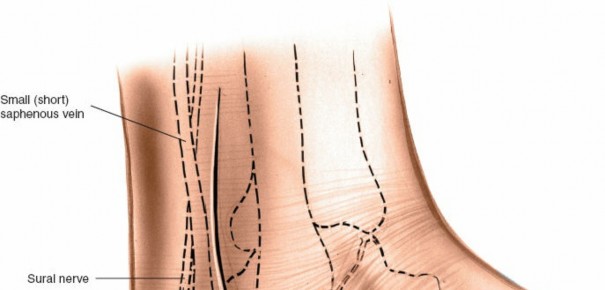
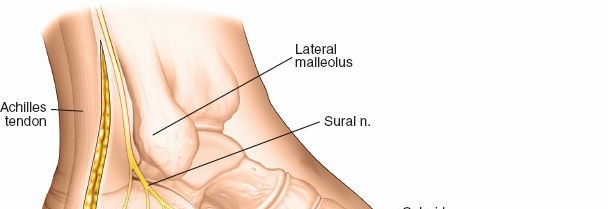
* Sural nerve: This sensory nerve typically arises from the tibial and common peroneal nerves. It descends superficially, often posterior to the lateral malleolus, and then courses along the lateral border of the foot. It is highly susceptible to injury during lateral approaches and must be carefully identified and protected. It generally lies superficial to the peroneal tendons.
* Lesser saphenous vein: Often accompanies the sural nerve and requires similar careful management.
* Calcaneal branches of the superficial peroneal nerve: May be encountered more distally.
* Peroneal nerves: The peroneus muscles are innervated by the superficial peroneal nerve, which typically supplies branches well proximal to the surgical field, making the approach safe in terms of muscle innervation provided the main nerve trunk is protected.
Biomechanics of the Subtalar Joint
The subtalar joint functions as a torque converter, allowing the foot to adapt to uneven surfaces while maintaining stability for propulsion. Its primary motions are pronation (eversion, abduction, dorsiflexion) and supination (inversion, adduction, plantarflexion). The posterior facet is critical for transmitting ground reaction forces and facilitating these triplanar motions. Subtalar arthrodesis, while effective for pain relief and stability, eliminates this motion, transferring stress to adjacent joints (tibiotalar and talonavicular joints). This altered biomechanics can lead to adjacent joint arthritis over time, a recognized long-term sequela. The fusion position is critical, typically aiming for 0-5 degrees of hindfoot valgus, neutral dorsiflexion, and slight external rotation, to optimize gait mechanics and minimize stress on the ankle.
Indications and Contraindications
The decision to proceed with a lateral approach to the posterior talocalcaneal joint is predicated upon a careful assessment of the patient's symptoms, physical examination findings, and advanced imaging.
Indications
The primary indications for this approach typically involve conditions requiring arthrodesis or extensive debridement of the posterior subtalar joint.
- Subtalar Arthritis:
- Post-traumatic arthritis: Most common cause, particularly following calcaneal or talar fractures, leading to pain, stiffness, and often deformity.
- Degenerative arthritis: Idiopathic or secondary to long-standing hindfoot malalignment.
- Inflammatory arthritis: Rheumatoid arthritis or other seronegative spondyloarthropathies affecting the subtalar joint.
- Subtalar Instability: Persistent symptomatic instability after non-operative treatment, often post-traumatic.
- Talocalcaneal Coalition: Resection of symptomatic osseous or fibrous coalitions that restrict motion and cause pain. Arthrodesis may be indicated in cases of extensive coalition or failed resection.
- Subtalar Fractures/Dislocations: While often approached posteromedially or via sinus tarsi for reduction, extensive comminution or articular damage may necessitate the lateral approach for definitive fixation or primary fusion.
- Subtalar Nonunion/Malunion: After previous subtalar surgery, requiring revision surgery, debridement, and repeat fusion.
- Hindfoot Deformity: Corrective arthrodesis for painful hindfoot deformities such as pes planus (flatfoot) or pes cavus, often as part of a triple arthrodesis, but the subtalar component is accessed laterally.
- Avascular Necrosis of the Talus/Calcaneus: If severe and involving the articular surface of the posterior facet, leading to collapse and arthritis.
- Tumor Resection: Rare, for benign or malignant lesions affecting the talus or calcaneus that necessitate lateral hindfoot exposure.
Contraindications
Absolute contraindications are few but critical, while relative contraindications require careful consideration and risk-benefit analysis.
- Absolute Contraindications:
- Active Infection: Osteomyelitis or septic arthritis in the surgical field.
- Severe Peripheral Vascular Disease: Compromised healing potential, increasing risk of wound complications and nonunion.
- Uncontrolled Systemic Illness: Significant comorbidities that preclude safe anesthesia or surgical recovery (e.g., uncontrolled diabetes, severe cardiac disease).
- Poor Soft Tissue Envelope: Compromised skin or subcutaneous tissue from previous surgery, trauma, or radiation, increasing wound complication risk.
- Relative Contraindications:
- Severe Hindfoot Valgus Deformity: May necessitate a more medial or combined approach for adequate correction and hardware placement.
- Neuropathic Arthropathy (Charcot Foot): While arthrodesis is often indicated, these cases have higher complication rates and require specialized approaches and extended non-weight bearing.
- Patient Refusal: Unwillingness to comply with post-operative rehabilitation protocols.
- Smoking/Nicotine Use: Significantly increases rates of nonunion and wound complications. Aggressive counseling and cessation are strongly recommended preoperatively.
Operative vs. Non-Operative Indications Table
| Indication Type | Specific Pathology/Condition | Operative Indications (Lateral Approach) | Non-Operative Indications |
|---|---|---|---|
| Arthritis | Post-traumatic subtalar arthritis | Persistent, debilitating pain unresponsive to conservative measures; radiographic evidence of advanced arthritis (joint space narrowing, osteophytes, subchondral sclerosis); significant functional impairment; deformity correction required. Arthrodesis for end-stage disease. | Mild to moderate pain; early radiographic changes; activity modification; NSAIDs; custom orthotics/braces; corticosteroid injections (diagnostic and therapeutic); physical therapy for pain management and mobility. |
| Degenerative subtalar arthritis | Same as post-traumatic arthritis; often idiopathic or secondary to biomechanical misalignment. | Same as post-traumatic arthritis. | |
| Inflammatory arthritis (e.g., Rheumatoid) | Active inflammation controlled; joint destruction with pain and deformity; failure of medical management; fusion for stability and pain relief. | Systemic medical management (DMARDs, biologics); NSAIDs; custom orthotics; injections; physical therapy. | |
| Instability | Chronic subtalar instability | Persistent symptomatic instability despite adequate immobilization and rehabilitation; recurrent sprains; functional limitations. Ligament repair/reconstruction or arthrodesis in severe cases. | Immobilization (brace, cast); physical therapy focusing on proprioception and peroneal strengthening; activity modification. |
| Deformity | Talocalcaneal coalition | Symptomatic fibrous or osseous coalition causing chronic pain, stiffness, and limping, especially with failure of initial non-operative treatment or extensive coalition. Excision of coalition (for smaller, fibrous) or arthrodesis (for extensive, osseous, or failed excision). | Activity modification; NSAIDs; orthotics; casting/bracing for rest; corticosteroid injections; physical therapy. |
| Hindfoot malalignment (e.g., severe pes planus/cavus) | Progressive painful deformity refractory to conservative measures; involvement of subtalar joint in complex hindfoot reconstruction. Arthrodesis often combined with other procedures. | Orthotics; shoe modifications; physical therapy; bracing. | |
| Trauma | Subtalar fracture/dislocation (select cases) | Irreducible dislocations; comminuted articular fractures with significant displacement or joint depression; nonunion or malunion after prior fixation; primary arthrodesis for severely destroyed articular surfaces. | Closed reduction and casting/bracing for stable injuries; non-displaced fractures; early range of motion for select stable injuries; pain management. |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is fundamental to achieving optimal outcomes and minimizing complications. This phase involves a comprehensive evaluation of the patient's condition, detailed imaging analysis, and precise intraoperative setup.
Imaging Modalities
- Plain Radiographs: Standard views (AP, lateral, oblique of the ankle and foot) are essential. Harris heel views (axial calcaneal view) are critical for assessing hindfoot alignment (valgus/varus) and calcaneal body pathology. Weight-bearing views are imperative to evaluate the true anatomical and functional alignment of the hindfoot.
- Computed Tomography (CT) Scan: The gold standard for assessing bony pathology of the subtalar joint. It provides detailed information regarding joint space narrowing, osteophyte formation, subchondral cysts, talocalcaneal coalition, and the extent of fracture involvement. Three-dimensional (3D) reconstructions are invaluable for understanding complex deformities and planning screw trajectories, especially in arthrodesis.
- Magnetic Resonance Imaging (MRI): Primarily useful for evaluating soft tissue structures, such as cartilage integrity, synovial inflammation, stress reactions, and interosseous ligament pathology. It can also detect early avascular necrosis or subtle coalitions not clearly seen on plain films.
Preoperative Surgical Planning
Based on imaging, the surgeon should:
1. Determine the extent of arthritic involvement: Confirm that the posterior facet is the primary pain generator.
2. Assess bone quality and quantity: Important for hardware selection and potential need for bone grafting.
3. Plan hardware placement: Determine optimal screw size, length, and trajectory for compression and stability, avoiding critical neurovascular structures.
4. Anticipate deformity correction: Plan for any wedges, osteotomies, or bone graft requirements to achieve optimal hindfoot alignment.
5. Identify potential challenges: Note any significant osteophytes, hardware from previous surgeries, or severe deformity that may complicate exposure.
Patient Positioning
The patient's position on the operating table is crucial for optimizing surgical access and ergonomics.
- Place the patient supine on the operating table.
- A sandbag or bump should be positioned under the ipsilateral buttock (the affected side). This maneuver internally rotates the limb, bringing the lateral malleolus and the entire lateral aspect of the hindfoot forward, significantly improving surgical access and reducing strain on the surgeon.
- A support on the contralateral iliac crest can further stabilize the patient and optimize the tilt.
- The operating table should be tilted 20 to 30 degrees away from the surgeon. This combined positioning strategy maximizes exposure and allows for a more direct line of sight to the posterior facet.
- The entire lower limb from the hip to the toes should be prepped and draped in a sterile fashion, allowing for free manipulation of the foot and ankle to assess alignment and facilitate hardware placement.
- Exsanguination of the limb is performed either by elevating it for 3 to 5 minutes or by applying a soft rubber bandage (e.g., Esmarch bandage).
- A thigh tourniquet is then inflated to maintain a bloodless field, which is critical for clear visualization of anatomical structures and reducing operative time. The tourniquet pressure should be appropriate for the patient's blood pressure and maintained for the shortest duration possible to minimize complications.
Depiction of limb exsanguination and tourniquet application. - The C-arm fluoroscopy unit should be positioned to allow unobstructed AP, lateral, and oblique views of the hindfoot without contamination of the sterile field or excessive repositioning of the limb during the procedure.
Detailed Surgical Approach and Technique
The lateral approach provides excellent exposure of the posterior facet of the talocalcaneal joint, offering ample space for debridement, bone preparation, and hardware insertion, particularly advantageous for arthrodesis.
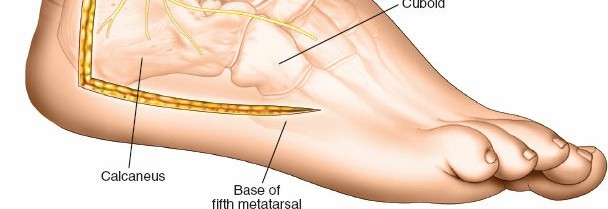
Landmarks and Incision
The key bony landmarks for the incision are the lateral malleolus and the peroneal tubercle. The peroneal tubercle typically lies distal and anterior to the lateral malleolus.
The incision is generally longitudinal or slightly curvilinear, centered over the sinus tarsi, extending from the tip of the lateral malleolus distally towards the calcaneocuboid joint or further to the base of the fifth metatarsal if broader exposure is needed. Its length typically ranges from 5 to 8 cm, depending on the extent of pathology and the patient's body habitus. A curvilinear incision can provide a slightly wider skin flap.
The original seed content refers to a figure 12-46). for the incision, which isn't provided. However, a relevant image of an incision is among the provided files.
Typical curvilinear incision for the lateral approach to the posterior talocalcaneal joint.
Superficial Dissection and Neurovascular Protection
After incising the skin and subcutaneous tissue, meticulous dissection is crucial for protecting the superficial neurovascular structures.
- Identify and protect the sural nerve and its accompanying lesser saphenous vein. The sural nerve typically courses superficially, often posterior to the lateral malleolus, and then runs along the lateral aspect of the foot. It is frequently seen within the superficial adipose tissue layers and should be carefully isolated, retracted dorsally or ventrally, and protected throughout the procedure. Any direct traction or cautery should be avoided.
Initial incision of skin and subcutaneous tissue, highlighting the need for careful dissection.

Careful blunt dissection to identify superficial nerves and vessels, such as the sural nerve.
Retraction of superficial structures to expose deeper fascial layers.
Deep Dissection and Internervous Plane
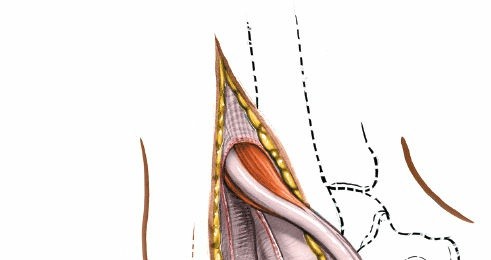
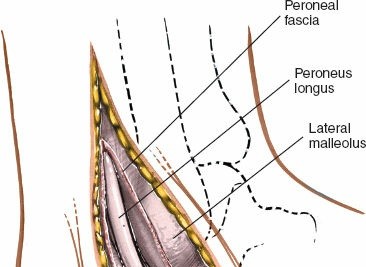
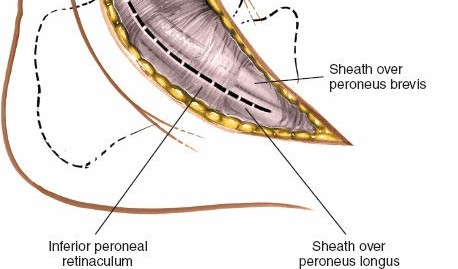
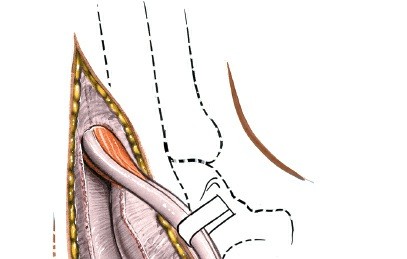
- Incise the deep fascia overlying the peroneal tendons.
- Identify the peroneus longus and peroneus brevis tendons. The peroneus brevis tendon typically lies anterior and deep to the longus. Both tendons run posterior to the lateral malleolus and then across the lateral aspect of the calcaneus.
- Retract the peroneal tendons and their sheaths anteriorly using a self-retaining retractor or blunt Hohmann retractors. This exposes the underlying calcaneus and the sinus tarsi.
Deep dissection exposing the peroneal tendons.

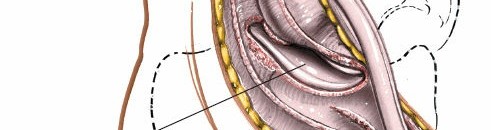
Retraction of peroneal tendons to expose the underlying structures of the sinus tarsi.

Further anterior retraction of peroneal tendons, providing a clear view of the sinus tarsi.
The original seed content correctly states that no true internervous plane exists in this approach. The peroneus muscles, whose tendons are mobilized and retracted anteriorly, share a nerve supply from the superficial peroneal nerve. The approach is safe because these muscles receive their nerve supply at a point well proximal to the surgical field, making them resistant to denervation injury from retraction.
Joint Exposure and Preparation for Arthrodesis
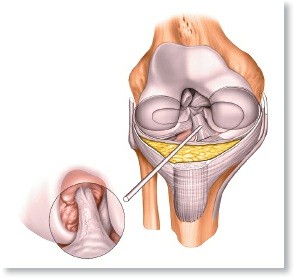
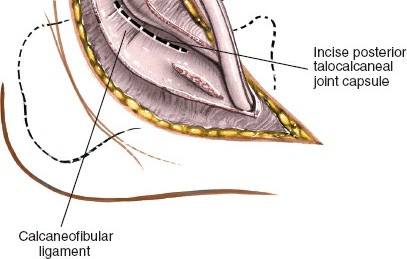
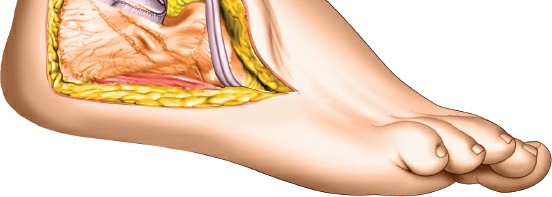
- Once the peroneal tendons are retracted, the sinus tarsi is exposed. The fat pad within the sinus tarsi and the strong interosseous talocalcaneal ligament and cervical ligament must be incised and resected. This step provides access to the posterior facet of the subtalar joint.
- Carefully release the capsule of the posterior talocalcaneal joint. Osteophytes, if present, are then resected to facilitate joint distraction and alignment.
- Using osteotomes, curettes, and burrs, the articular cartilage from both the talar and calcaneal sides of the posterior facet must be completely removed to expose bleeding subchondral bone. This is critical for promoting fusion. The subchondral bone can also be fenestrated or microfractured to encourage bleeding and osteogenesis.

Exposure of the posterior subtalar joint, demonstrating the sinus tarsi and surrounding ligaments.
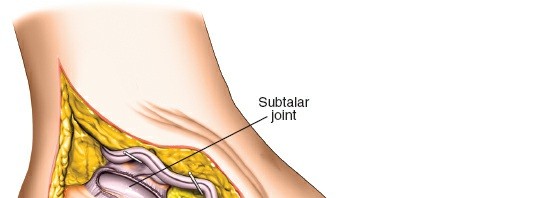
Initial debridement and removal of soft tissues within the sinus tarsi to visualize the joint.
More extensive debridement of articular cartilage and preparation of the bony surfaces.
Detailed view of cartilage removal and decortication of the subchondral bone on the calcaneal side.
Preparation of the talar articular surface for fusion, ensuring all cartilage is removed.
Demonstration of complete cartilage removal and exposure of cancellous bone, ready for fusion.
The prepared joint surfaces after decortication and removal of eburnated bone.- If significant bone loss or deformity exists, bone grafting may be necessary to fill defects and enhance fusion rates. Autograft (e.g., from the distal tibia, calcaneus, or iliac crest) or allograft can be utilized.
Alignment and Fixation
- The foot must be positioned in an optimal functional alignment prior to fixation. The generally accepted position for subtalar arthrodesis is neutral dorsiflexion, 0-5 degrees of hindfoot valgus, and 5-10 degrees of external rotation relative to the tibia. This position optimizes biomechanics for walking and reduces stress on adjacent joints.
- Temporary K-wires can be used to hold the desired position.
- Fixation typically involves two or three large cannulated screws (e.g., 6.5mm or 7.3mm) placed across the fusion site.
- Screws are usually inserted from the calcaneus into the talus. One common trajectory is from the posterior-lateral aspect of the calcaneal tuberosity, aiming anterior-medially into the body of the talus. Another screw can be placed more anteriorly from the lateral calcaneus into the talar neck.
- Careful use of fluoroscopy in multiple planes (AP, lateral, Harris heel view) is essential to confirm correct placement, length, and compression across the fusion site, while avoiding intra-articular penetration into the ankle joint or damage to neurovascular structures.
Initial placement of guide wires for screw fixation, aiming from calcaneus to talus.
Screws being advanced over guide wires, ensuring proper trajectory and compression.
Final screw placement achieving compression across the prepared subtalar joint.
Post-fixation image demonstrating stable fusion with appropriate screw placement.
- Once satisfactory fixation and alignment are achieved, the wound is copiously irrigated.
Closure
- The peroneal tendons are allowed to fall back into their anatomical position.
- The deep fascia is repaired.
- Subcutaneous layers are closed.
- The skin is closed with sutures or staples.
- A drain may be considered if significant dead space or concern for hematoma exists.
- A sterile dressing and a posterior splint or cast are applied, maintaining the foot in the corrected fusion position.
Complications and Management
Despite meticulous surgical technique, complications can arise following a lateral approach to the posterior talocalcaneal joint. Awareness of these potential issues and proactive management strategies are critical for optimizing patient outcomes.
Common Complications
| Complication | Typical Incidence (%) | Management Strategy |
|---|---|---|
| Nonunion/Delayed Union | 5-20% | Risk factors: Smoking, NSAID use, diabetes, poor bone quality, inadequate debridement, insufficient compression, infection. Diagnosis: Persistent pain, motion at fusion site, lack of bridging trabeculae on radiographs/CT after 3-6 months. Management: Initial management may involve extended non-weight bearing, bracing, bone stimulators (electrical/ultrasound). For established nonunion, revision surgery with debridement of fibrous tissue, fresh bone grafting (autograft preferred), and rigid internal fixation is typically required. Consider adjunctive biologics (e.g., PRP, BMPs). |
| Sural Nerve Injury | 5-15% | Risk factors: Direct transection, traction injury, entrapment in scar tissue. Diagnosis: Numbness, dysesthesia, neuropathic pain in the lateral foot and ankle. Management: Prevention is key (careful identification and protection). For mild neuropraxia, observation, gabapentin/pregabalin, local nerve blocks may suffice. For persistent or severe symptoms, neurolysis may be considered. Transection may require nerve repair or grafting, though outcomes are variable. Neuroma formation may require excision. |
| Infection | 1-5% | Risk factors: Diabetes, immunosuppression, prolonged surgery, poor wound healing, compromised soft tissue. Diagnosis: Local signs of inflammation (erythema, warmth, tenderness, purulence), fever, elevated inflammatory markers (ESR, CRP). Management: Superficial infections may respond to oral antibiotics and local wound care. Deep infections (osteomyelitis) typically require surgical debridement, washout, IV antibiotics based on culture results, and potentially hardware removal. Fusion may be compromised, necessitating further revision procedures. |
| Wound Complications | 5-10% | Risk factors: Smoking, diabetes, obesity, steroid use, tension on closure, hematoma. Diagnosis: Dehiscence, necrosis, delayed healing. Management: Local wound care, serial debridement, moist dressings. May require secondary closure, negative pressure wound therapy (NPWT), or rarely, plastic surgery consultation for flap coverage. |
| Malunion | 2-10% | Risk factors: Inadequate preoperative planning, incorrect intraoperative positioning, loss of fixation. Diagnosis: Persistent hindfoot pain, gait abnormalities, progressive adjacent joint arthritis, radiographic evidence of improper alignment (e.g., excessive varus/valgus, equinus). Management: For symptomatic malunion, corrective osteotomy and revision arthrodesis may be required. Asymptomatic malunion may be managed with orthotics and activity modification. |
| Painful Hardware | 5-15% | Risk factors: Prominent screw heads, superficial placement, persistent inflammation. Diagnosis: Localized pain over hardware, often exacerbated by shoe wear or palpation. Management: Often resolves spontaneously. If persistent and debilitating after fusion is confirmed (typically >6-12 months post-op), hardware removal can be performed. This is usually a straightforward procedure with low morbidity once fusion is solid. |
| Peroneal Tendinitis/Tenosynovitis | <5% | Risk factors: Irritation from hardware, excessive retraction, scar tissue, altered biomechanics. Diagnosis: Pain and tenderness along the peroneal tendon course, worse with ankle motion. Management: Rest, NSAIDs, physical therapy. Steroid injections can be diagnostic and therapeutic. Surgical exploration, tenolysis, or hardware removal may be necessary if symptoms persist. |
| Adjacent Joint Arthritis | 10-30% (long-term) | Risk factors: Arthrodesis alters biomechanics, increasing stress on the tibiotalar and talonavicular joints. Diagnosis: Gradual onset of pain and stiffness in the ankle or midfoot years after subtalar fusion; radiographic evidence of joint space narrowing, osteophytes. Management: Non-operative (NSAIDs, orthotics, injections, physical therapy) for mild to moderate symptoms. For severe, debilitating arthritis, further surgical intervention (e.g., total ankle arthroplasty, ankle fusion, midfoot fusion) may eventually be required. |
| Complex Regional Pain Syndrome (CRPS) | <1% | Risk factors: Unpredictable; more common in patients with pre-existing neuropathic conditions or anxiety/depression. Diagnosis: Disproportionate pain, allodynia, hyperalgesia, swelling, skin changes (color, temperature, sweating). Management: Early recognition is key. Multidisciplinary approach involving pain management specialists, physical therapy, sympathetic blocks, medications (gabapentinoids, antidepressants). |
| Deep Vein Thrombosis (DVT)/Pulmonary Embolism (PE) | <1% | Risk factors: Prolonged immobilization, hypercoagulable states, history of DVT/PE, obesity, advanced age. Diagnosis: Swelling, pain, warmth in calf/thigh (DVT); dyspnea, chest pain (PE). Management: Prophylactic anticoagulation (chemical or mechanical) as per institutional guidelines. For diagnosed DVT/PE, therapeutic anticoagulation is initiated. |
Salvage Strategies for Failed Arthrodesis
In cases of symptomatic nonunion or severe malunion, revision surgery is the primary salvage strategy. This typically involves:
* Hardware removal: If existing hardware is loose or causing symptoms.
* Debridement: Meticulous removal of all fibrous tissue, sclerotic bone, and remaining cartilage from the nonunion site to expose fresh, bleeding bone.
* Bone grafting: Often crucial to enhance biological healing. Autogenous bone graft (e.g., iliac crest, distal tibia, calcaneus) is generally preferred due to its osteoinductive, osteoconductive, and osteogenic properties. Allograft or bone graft substitutes may also be used.
* Re-fixation: Stable internal fixation with larger or additional screws, plates, or a combination, ensuring strong compression across the fusion site.
* Corrective osteotomy: If significant malunion is present, a corrective osteotomy of the talus or calcaneus may be necessary to restore proper hindfoot alignment before re-arthrodesis.
* Biologics: Consideration of adjuncts such as bone morphogenetic proteins (BMPs) or platelet-rich plasma (PRP), although evidence for routine use in subtalar fusion is still evolving.
Post Operative Rehabilitation Protocols
A structured and progressive postoperative rehabilitation protocol is crucial for optimizing healing, achieving successful fusion, and restoring function after a lateral approach to the posterior talocalcaneal joint. Protocols may vary slightly based on surgeon preference, patient factors, and intraoperative findings (e.g., bone quality, stability of fixation).
Phase 1: Immobilization and Non-Weight Bearing (Weeks 0-6)
- Goal: Protect the fusion site, promote initial healing, manage pain and swelling.
- Immediate Post-op (Day 0-3):
- Posterior splint or bulky soft dressing applied in the operating room.
- Strict non-weight bearing (NWB) with crutches or walker.
- Elevation of the limb above heart level (first 48-72 hours particularly important).
- Ice application (avoiding direct contact with skin).
- Pain management protocol (multimodal approach including NSAIDs, opioids, nerve blocks if applicable).
- Early Post-op (Weeks 1-2):
- Wound check at 1-2 weeks. Staples/sutures removed as appropriate.
- Transition from posterior splint to a short leg non-weight bearing cast or controlled ankle motion (CAM) boot locked at neutral.
- Patient education on NWB status, wound care, and DVT prophylaxis.
- Initiate gentle active range of motion (AROM) of the knee and hip on the operative side, and foot/toe wiggles to prevent stiffness and promote circulation.
- Mid-Post-op (Weeks 2-6):
- Continue NWB in a cast or CAM boot.
- Continue elevation and ice as needed.
- Focus on general conditioning and upper body strengthening.
- Monitor for signs of complications (infection, nerve irritation).
- Radiographs typically taken at 4-6 weeks to assess early fusion progress.
Phase 2: Progressive Weight Bearing (Weeks 6-12)
- Goal: Gradually introduce weight bearing, maintain immobilization of the fusion, and address adjacent joint mobility.
- Weeks 6-8 (or when radiographic signs of early fusion appear):
- If radiographs show early evidence of bridging bone and the fusion site is stable, transition to protected weight bearing.
- Begin partial weight bearing (PWB) in the CAM boot, typically starting at 25% of body weight, progressing to 50-75% over 2-4 weeks as tolerated.
- Physical therapy initiated:
- Continue NWB exercises for general conditioning.
- Initiate gentle range of motion for adjacent joints (ankle dorsiflexion/plantarflexion, midfoot and forefoot motion) if not fused.
- Gait training with crutches, focusing on proper heel-toe progression.
- Regular radiographic checks (every 2-4 weeks) to monitor fusion progression.
- Weeks 8-12:
- Continue progressive weight bearing in the CAM boot.
- Advance to full weight bearing (FWB) in the CAM boot as radiographic union progresses and pain allows.
- Physical therapy advances:
- Balance and proprioception exercises (within the boot).
- Strengthening of surrounding muscles (e.g., hip abductors, knee extensors, gastroc-soleus complex).
- Continue gait training, aiming for symmetrical weight distribution.
Phase 3: Transition to Regular Footwear and Advanced Strengthening (Weeks 12-24)
- Goal: Discontinue external immobilization, restore full range of motion in adjacent joints, improve strength, balance, and prepare for functional activities.
- Weeks 12-16 (or when radiographic union is evident):
- Discontinue CAM boot when radiographic signs confirm solid fusion and patient comfort allows.
- Transition to supportive lace-up shoes (e.g., athletic shoes). Orthotics may be prescribed.
- Physical therapy:
- Aggressive ankle and midfoot range of motion exercises (if not fused).
- Strengthening exercises for entire lower extremity, particularly focusing on calf muscles (gastroc-soleus).
- Advanced balance and proprioception training (e.g., single-leg stance, unstable surfaces).
- Gradual return to low-impact activities (e.g., stationary cycling, swimming).
- Radiographs at 3 months post-op to confirm union.
- Weeks 16-24:
- Continue progressive strengthening and conditioning.
- Introduce higher-impact activities incrementally, depending on patient goals and fusion solidity (e.g., light jogging, hiking).
- Focus on sport-specific training if applicable.
- Continue home exercise program.
Phase 4: Return to Full Activity (Beyond 24 Weeks)
- Goal: Achieve maximum functional recovery and return to desired activities.
- 6 Months and Beyond:
- Full return to work and recreational activities as tolerated, guided by symptomology and physical therapy progress.
- Long-term monitoring for adjacent joint arthritis due to altered biomechanics.
- Encourage activity modification to minimize stress on the fused joint and surrounding articulations.
Throughout all phases, patient compliance, regular clinical assessment, and radiographic monitoring are paramount. Individual progression rates will vary.
Summary of Key Literature and Guidelines
The lateral approach to the posterior talocalcaneal joint, primarily for arthrodesis, has a robust history in orthopedic foot and ankle surgery. A wealth of literature supports its efficacy and defines best practices, though comparative studies with other approaches and long-term outcomes continue to evolve.
Efficacy of Subtalar Arthrodesis
- High Fusion Rates: Studies consistently report high fusion rates for subtalar arthrodesis, typically ranging from 85% to 95%. Early series and meta-analyses, such as those by Russotti and Johnson (1992) or Easley et al. (2000), established the procedure's reliability in achieving union. Nonunion rates, while present, are often mitigated by meticulous surgical technique, aggressive decortication, bone grafting, and rigid internal fixation. Patient factors like smoking and diabetes are consistently identified as significant risk factors for nonunion.
- Pain Relief and Functional Improvement: The primary goal of subtalar arthrodesis is pain relief, which is achieved in a vast majority of patients. Functional improvement, while often significant, is dependent on the preoperative functional status and the presence of adjacent joint pathology. Patients typically experience improved stability and walking tolerance on uneven ground, albeit with a loss of subtalar motion.
- Long-Term Outcomes: Long-term follow-up studies, some extending beyond 10-15 years, highlight the challenge of adjacent joint arthritis, particularly in the tibiotalar and talonavicular joints. This phenomenon, often termed "adjacent segment disease," results from the increased biomechanical stress transferred to these joints following the loss of subtalar motion. While not universally problematic, it underscores the importance of careful patient selection and preoperative counseling regarding potential late sequelae. Hintermann et al. (2002) and others have extensively studied these compensatory changes.
Comparison with Other Approaches
- Sinus Tarsi Approach: Often considered a minimally invasive variant of the lateral approach, the sinus tarsi approach provides excellent visualization of the anterior and middle facets, and can be extended to view the posterior facet. It minimizes soft tissue stripping and can be used for both arthroscopic and open procedures. However, for extensive posterior facet pathology or significant deformity requiring extensive correction, the direct lateral approach offers superior access and working space for instrumentation and bone grafting.
- Posterior Approach: Provides direct access to the posterior talus and calcaneus. It is typically utilized for posterior ankle arthroscopy, os trigonum excision, or occasionally for isolated posterior subtalar fusion. Its utility for comprehensive posterior facet arthrodesis is more limited compared to the lateral approach, especially for calcaneal pathology or when aiming for specific hindfoot alignment.
- Medial Approach: Primarily used for conditions requiring access to the medial aspect of the hindfoot, such as for talonavicular or tibiotalar fusions, or severe valgus deformities that are more effectively corrected from the medial side. It is rarely a primary approach for isolated posterior subtalar issues.
- Arthroscopic Subtalar Arthrodesis: Gained popularity due to potential for reduced soft tissue morbidity, smaller incisions, and faster recovery. It is effective for early-stage subtalar arthritis or for isolated, less complex fusions. However, it presents a steeper learning curve, may offer less robust decortication in severe cases, and can be challenging for significant deformity correction. Open lateral approach remains the gold standard for complex cases.
Current Guidelines and Best Practices
- Rigid Internal Fixation: Consensus supports the use of at least two large-diameter, fully threaded cannulated screws for rigid internal fixation, providing stable compression across the fusion site.
- Complete Cartilage Removal and Decortication: Essential for successful arthrodesis. Exposure of bleeding subchondral bone is paramount to stimulate bone healing.
- Bone Grafting: Autogenous bone graft is preferred, especially in high-risk patients (smokers, revision cases) or when bone voids are present.
- Optimal Foot Alignment: Critical for long-term function and minimizing adjacent joint stress. The target is typically 0-5 degrees of hindfoot valgus, neutral dorsiflexion, and slight external rotation. Fluoroscopic control throughout the procedure is mandatory.
- Neurovascular Protection: Meticulous dissection to identify and protect the sural nerve is emphasized to prevent chronic neuropathic pain.
- Multimodal Pain Management and Early Rehabilitation: Protocols promoting early controlled mobility of unfused joints and gradual weight bearing once radiographic union is evident are standard.
Future Directions
Research continues to focus on:
* Biologics: The role of platelet-rich plasma (PRP), bone marrow aspirate concentrate (BMAC), and bone morphogenetic proteins (BMPs) in enhancing fusion rates, particularly in high-risk patients or revision surgeries.
* Advanced Imaging: Improved preoperative planning with advanced 3D imaging and patient-specific guides.
* Outcomes Research: Further long-term studies comparing open and arthroscopic techniques, refining indications, and better understanding the progression of adjacent joint arthritis.
* Ankle Replacement vs. Hindfoot Fusion: While primarily relevant to ankle arthritis, the increasing success of total ankle arthroplasty sometimes places it in a decision-making algorithm when considering the broader impact of hindfoot pathology and fusion on overall lower extremity function.
Mastering the lateral approach to the posterior talocalcaneal joint remains a cornerstone skill for any orthopedic foot and ankle surgeon, enabling effective management of a range of debilitating hindfoot pathologies with predictable outcomes when executed with precision and comprehensive patient care.
Clinical & Radiographic Imaging

You Might Also Like