Operative Management of Median and Superficial Radial Nerves at the Wrist
Key Takeaway
Division of the median nerve at the wrist severely compromises hand function. Successful restoration requires meticulous microsurgical repair, precise rotational alignment, and tension-free coaptation. This guide details the operative management of median nerve lacerations, recurrent motor branch variations, and the strategic handling of superficial radial nerve injuries to prevent debilitating neuromas and optimize both sensory and motor recovery in the hand.
INTRODUCTION TO MEDIAN NERVE INJURIES AT THE WRIST
Division of the median nerve at the wrist is a common and functionally devastating injury. Because the vital sensory function of the palmar aspect of the hand—particularly the thumb, index, and middle fingers—depends entirely on the success of this repair, meticulous microsurgical technique is mandatory. Furthermore, the median nerve at this level is a mixed nerve; it carries critical motor fibers to the thenar musculature. Failure to restore motor function results in severe impairment of thumb opposition and pinch strength.
According to Boyes' foundational principles of nerve repair, functional results are directly proportional to the accuracy of fascicular approximation and inversely proportional to the degree of postoperative scarring and fibrosis. Regeneration occurs in an orderly, albeit slow, biological sequence. The ultimate prognosis relies heavily on the surgeon’s ability to create a tension-free, well-vascularized, and anatomically precise coaptation.
Clinical Pearl: Historical texts occasionally reference testing the first dorsal interosseous (FDI) muscle to monitor median nerve recovery. Anatomically, the FDI is innervated by the ulnar nerve. True median motor recovery must be evaluated via the voluntary activity of the Abductor Pollicis Brevis (APB). However, the surgeon must remain cognizant of Martin-Gruber anastomoses in the forearm or Riche-Cannieu anastomoses in the hand, which can confound standard clinical motor testing.
SURGICAL ANATOMY AND BIOMECHANICS
The Median Nerve at the Carpal Tunnel
As the median nerve transitions from the distal forearm into the carpal tunnel, it lies superficial and slightly radial to the superficial flexor tendons. It is bordered radially by the flexor carpi radialis (FCR) and ulnarly by the palmaris longus (PL). At this level, the nerve has a distinct fascicular architecture. The motor fibers destined for the thenar eminence are typically grouped in the radial-volar quadrant of the nerve, a critical anatomical detail when aligning the nerve ends for repair.
The Recurrent Motor Branch
Every effort must be made to identify and repair the recurrent motor branch of the median nerve if it has been severed. This branch usually projects from the main trunk radially and superficially, passing just over the distal margin of the transverse carpal ligament. It courses slightly posteriorly and laterally to innervate the thenar muscles (APB, opponens pollicis, and the superficial head of the flexor pollicis brevis).
Surgeons must be intimately familiar with the anatomical variations of the recurrent branch (often categorized by the Lanz classification):
1. Extraligamentous (Standard): Branches distal to the transverse carpal ligament and recurrently enters the thenar musculature.
2. Subligamentous: Branches within the carpal tunnel and runs deep to the ligament before entering the muscle.
3. Transligamentous: Pierces directly through the transverse carpal ligament (highly susceptible to injury during carpal tunnel release or trauma).
4. Ulnar Origin: Originates from the ulnar aspect of the median nerve and crosses over the main trunk.
5. Bifurcated/Duplicated: Represented by two distinct branches instead of one.
PREOPERATIVE EVALUATION AND INDICATIONS
Indications for Surgery
- Acute Lacerations: Immediate or early delayed (within 1-3 weeks) primary repair is the gold standard for sharp transections.
- Delayed Presentations: Secondary repair or nerve grafting is indicated if the injury was missed or if the wound was heavily contaminated, necessitating delayed closure.
- Neuroma-in-Continuity: Requires exploration, intraoperative nerve monitoring, and potential resection with grafting if conduction is absent.
Clinical Assessment
Preoperative documentation of sensory and motor deficits is medicolegally and clinically essential.
* Sensory: Static and moving two-point discrimination (2PD) in the autonomous zones (volar tip of the index finger for the median nerve).
* Motor: Palpation of the APB muscle belly during resisted palmar abduction of the thumb.
SURGICAL TECHNIQUE: MEDIAN NERVE REPAIR
1. Positioning and Setup
The patient is placed supine with the arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The procedure must be performed under loupe magnification (3.5x to 4.5x) or an operating microscope.
2. Incision and Exposure
Extend the traumatic laceration using a standard extensile carpal tunnel approach. The incision should cross the wrist flexion creases obliquely or in a zigzag fashion to prevent postoperative flexion contractures.
* Open the carpal tunnel by dividing the transverse carpal ligament completely to decompress the nerve and allow for proximal and distal mobilization.
* Identify the normal nerve proximally and distally in virgin tissue planes before tracing it into the zone of injury.
3. Preparation of the Nerve Ends
The most critical step in delayed or secondary repair is the preparation of the nerve stumps.
* Proximal Stump: The neuroma must be carefully and sequentially excised using a fresh scalpel blade or nerve cutting scissors until healthy, pouting fascicles ("mushrooming") are visualized.
* Distal Stump: The distal glioma (Schwannoma) must similarly be excised until healthy fascicular architecture is reached.
* Vascular Bed: The surrounding scar tissue must be radically excised to provide a healthy, well-vascularized soft-tissue bed for the repaired nerve. A nerve repaired over a bed of avascular scar will fail to regenerate due to ischemia.
4. Rotational Alignment
Because the median nerve is a mixed motor and sensory nerve, rotational mismatch will result in motor fibers regenerating down sensory endoneurial tubes, leading to functional failure.
* Vasa Nervorum: A longitudinal epineurial vessel usually lies on the anterior surface of the median nerve parallel with its long axis. This vessel is the most reliable landmark for securing proper rotational alignment. (Note: This vessel may be obliterated by scar in late repairs).
* Fascicular Matching: Match the size and grouping of the fascicles. The distinct motor group in the radial-volar quadrant should be aligned precisely.
* Epineurial Sutures: Placing a single epineurial marking suture in each segment prior to final resection can aid in maintaining proper rotation during the repair process.
5. Neurorrhaphy (Coaptation)
The repair must be accurate and completely tension-free.
* Use 8-0 or 9-0 nylon for the external epineurial repair.
* Use 10-0 nylon for internal group fascicular repair as needed to ensure alignment of the critical motor bundles.
* Tension Reduction: Tension can be reduced by dissecting and mobilizing the nerve proximally into the distal forearm. Flexing the wrist and elbow can temporarily relieve tension during the repair, but extreme flexion should be avoided as it leads to postoperative joint contractures and traction injury upon mobilization.
Surgical Warning: If the nerve ends cannot be coapted without tension while the wrist is in a neutral or slightly flexed position (no more than 20-30 degrees), a primary repair is contraindicated. A nerve graft must be utilized.
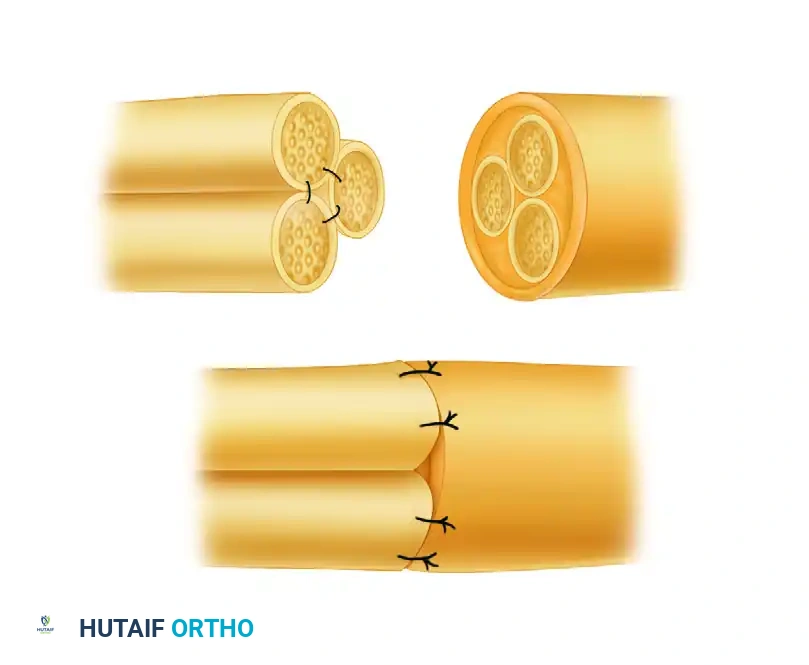
6. Managing Segmental Gaps
If a tension-free primary repair is impossible, interpositional nerve grafting is required. Sural nerve autografts are the gold standard. The grafts are reversed to prevent axonal escape through branches.
For segmental gaps, bundle suturing techniques (as illustrated in Figure 68-14) are employed to secure the cable grafts to the proximal and distal fascicular groups.
7. Repair of the Recurrent Motor Branch
The recurrent branch may be difficult to find because of surrounding fascia, hematoma, and scar tissue. When visualized, it can be identified readily by its distinct yellow fibers running transversely toward the base of the thumb.
* It is repaired using the microsurgical technique described for digital nerves, utilizing 10-0 or 11-0 nylon under high magnification.
* The prognosis for motor recovery is good if careful attention is given to anatomical detail and tension-free coaptation.
* Salvage: If the recurrent median nerve branch is avulsed or cannot be repaired, a neurovascular island free graft or a secondary tendon transfer (e.g., Extensor Indicis Proprius to APB - Burkhalter transfer) may be indicated at a later stage to restore opposition.
8. Closure
- Suture the volar carpal ligament (if reconstructed, though often left open to prevent compartment syndrome/compression).
- Replace the insertion of the palmaris brevis.
- Close the skin with non-absorbable sutures.
MANAGEMENT OF THE SUPERFICIAL RADIAL NERVE
Anatomy and Functional Impact
The superficial radial nerve (SRN) emerges from beneath the brachioradialis in the distal third of the forearm to provide sensation to the dorsoradial aspect of the hand, the dorsum of the thumb, and the index finger.
Disability after interruption of the SRN at the wrist is significantly less than that after interruption of the median or ulnar nerves on the volar surface. The resulting anesthesia over the dorsum of the thumb and index finger is generally well-tolerated. However, it is important to note that in some patients, the ulnar side of the area of pinch of the thumb receives its major innervation from the SRN via overlapping dermatomes.
The Problem of SRN Neuromas
The primary clinical issue with SRN lacerations is not the loss of sensation, but the development of exquisitely painful neuromas. Neuromas caught in dorsal wrist scars are particularly debilitating. They are mechanically stimulated not only by direct touch (resulting in a severe Tinel's sign) but also by the stretching of the surrounding skin, nerve, and scar tissue whenever the wrist and fingers are flexed or ulnarly deviated.
Surgical Decision Making: Resection vs. Repair
Unless there is a highly unusual and specific reason for repairing the SRN or one of its terminal branches, it should be resected proximal to its site of severance.
- Rationale: It is exceedingly common to develop a painful and disabling neuroma after a primary repair of the SRN. The small area of lost sensibility is a minor disability in comparison to the crippling neuropathic pain of a dorsal wrist neuroma.
- Technique for Resection:
- Identify the SRN proximal to the zone of injury.
- Apply gentle distal traction to the nerve.
- Transect the nerve sharply with a scalpel.
- Allow the proximal stump to retract deeply into the proximal forearm musculature (e.g., deep to the brachioradialis muscle belly).
- Ensure the nerve end lies in a well-vascularized area of minimal scar tissue, completely free from the mechanical excursion of the wrist joint and overlying skin.
Clinical Pearl: When resecting the SRN, burying the proximal stump into the brachioradialis muscle or capping the nerve end with a vein graft or synthetic conduit can further reduce the incidence of symptomatic neuroma formation.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Phase 1: Immobilization (Weeks 0-3)
- The wrist is immobilized in a dorsal blocking splint in neutral to slight flexion (10-20 degrees) to remove tension from the median nerve repair.
- Digital range of motion (ROM) is encouraged immediately to prevent tendon adhesions, provided it does not place tension on the nerve repair.
Phase 2: Early Mobilization (Weeks 3-6)
- The splint is gradually adjusted to bring the wrist into neutral and then slight extension.
- Active and active-assisted ROM of the wrist is initiated.
- Nerve gliding exercises are introduced cautiously to prevent the nerve from adhering to the carpal tunnel bed.
Phase 3: Strengthening and Sensory Re-education (Weeks 6+)
- Progressive strengthening of the forearm and hand musculature begins.
- Sensory Re-education: As the advancing Tinel's sign reaches the palm and digits (regenerating at approximately 1 mm per day), formal sensory re-education programs are instituted. This involves cortical remapping exercises using various textures, temperatures, and object recognition tasks.
- Motor Monitoring: The APB is monitored clinically and via electromyography (EMG) at 3 to 6 months postoperatively to confirm reinnervation. If no clinical or electrical signs of motor recovery are present by 6 to 9 months, tendon transfer surgery should be considered to restore thumb opposition.
You Might Also Like