Masterclass in Tendon Transfers: The Modified Bunnell Flexor Digitorum Sublimis Transfer
Key Takeaway
The modified Bunnell Flexor Digitorum Sublimis (FDS) transfer is a cornerstone surgical technique for correcting intrinsic minus hand deformities. By harvesting the ring or long finger FDS, splitting it into four tails, and routing them through the lumbrical canals to the extensor aponeuroses, surgeons can restore metacarpophalangeal flexion and interphalangeal extension. This guide details the biomechanics, step-by-step surgical approach, tensioning protocols, and postoperative rehabilitation required for optimal functional outcomes.
Introduction to Intrinsic Paralysis and Tendon Transfer
The restoration of intrinsic hand function following ulnar nerve palsy, combined median and ulnar nerve lesions, or severe neuropathies (such as Charcot-Marie-Tooth disease or Hansen’s disease) remains one of the most complex challenges in reconstructive hand surgery. The hallmark of intrinsic paralysis is the "intrinsic minus" or claw hand deformity, characterized by hyperextension of the metacarpophalangeal (MCP) joints and flexion of the proximal and distal interphalangeal (PIP and DIP) joints.
This predictable collapse of the digital cascade occurs due to the unopposed action of the extensor digitorum communis (EDC) at the MCP joint and the unopposed pull of the flexor digitorum profundus (FDP) and flexor digitorum sublimis (FDS) at the interphalangeal joints. To correct this biomechanical imbalance, the Modified Bunnell Flexor Digitorum Sublimis Transfer is employed. By re-routing a powerful extrinsic flexor (the FDS of the ring or long finger) to substitute for the paralyzed lumbricals and interossei, the surgeon can restore the critical volar flexion moment at the MCP joints and, depending on the insertion site, assist in IP joint extension.
This comprehensive guide details the preoperative considerations, precise surgical anatomy, step-by-step operative technique, critical tensioning parameters, and postoperative rehabilitation protocols required to execute this transfer successfully.
Pathoanatomy and Biomechanical Principles
To master the FDS transfer, the operating surgeon must possess a profound understanding of digital kinematics. The intrinsic muscles (lumbricals and interossei) normally pass volar to the transverse metacarpal ligament, providing a primary flexion force to the MCP joint. They then continue dorsally to insert into the lateral bands of the extensor aponeurosis, providing an extension force to the PIP and DIP joints.
When these muscles are paralyzed, the EDC hyperextends the MCP joint. Once the MCP joint falls into hyperextension, the EDC's excursion is exhausted, rendering it incapable of extending the PIP and DIP joints.
💡 Clinical Pearl: The Tenodesis Effect
The primary goal of the Bunnell FDS transfer is to prevent MCP hyperextension. By simply stabilizing the MCP joint in slight flexion, the extrinsic extensor (EDC) can effectively transmit its force distally to extend the PIP and DIP joints. This is the fundamental biomechanical principle behind all intrinsic replacement procedures.
Preoperative Evaluation and Indications
Patient Selection
The ideal candidate for an FDS transfer possesses supple, passively correctable joints. If fixed contractures are present at the PIP joint (e.g., severe volar plate contracture), tendon transfer alone will fail. Preoperative hand therapy and serial casting or surgical release of the volar plate must precede any tendon transfer.
The Bouvier Test
Always perform the Bouvier test during the clinical examination. Block the patient's MCP joints in slight flexion and ask them to actively extend their interphalangeal joints.
* Bouvier Positive: The patient can fully extend the PIP and DIP joints. This indicates that the EDC is functional and the extensor apparatus is intact. A standard MCP flexion block (like the Brooks modification) will suffice.
* Bouvier Negative: The patient cannot extend the PIP and DIP joints despite MCP stabilization. This indicates attenuation of the central slip or lateral bands. In these cases, the tendon transfer must be inserted into the lateral bands (the classic Bunnell technique) to actively extend the IP joints.
Surgical Technique: The Modified Bunnell FDS Transfer
The procedure is performed under regional anesthesia (brachial plexus block) or general anesthesia, utilizing a well-padded proximal pneumatic tourniquet inflated to 250 mm Hg. Loupe magnification (2.5x to 3.5x) is highly recommended for the precise handling of the extensor aponeurosis.
Step 1: Harvesting the Donor Tendon
The FDS of either the ring or the long finger may be selected as the donor. The ring finger is most commonly utilized to preserve the independent grasping function of the long finger.
- Incision: Make a midlateral incision, approximately 4.0 cm in length, on the radial side of the selected donor finger. Begin at the mid-shaft of the proximal phalanx and extend distally to just beyond the proximal interphalangeal (PIP) joint.
- Dissection: Carefully dissect through the subcutaneous tissue. Identify and protect the neurovascular bundle, retracting it volarly. Divide Cleland’s and Grayson’s ligaments to expose the flexor tendon sheath.
- Tendon Division: Deepen the incision to the flexor tendon sheath and open the sheath laterally (preserving the A2 and A4 pulleys if possible, though the A3 is often sacrificed). Identify the FDS tendon.
- Release: Divide the FDS tendon at the level of the proximal interphalangeal joint, just proximal to Camper's chiasm.
- Separation: Carefully separate the two slips of the FDS tendon. This separation must be meticulous to ensure the tendon can be smoothly withdrawn into the palm without tethering.
Step 2: Palmar Delivery and Preparation of the Graft
- Palmar Incision: Make a transverse incision, approximately 4.0 cm long, at the level of the proximal palmar crease.
- Identification: Deepen the incision through the palmar fascia. Identify the superficial palmar arch and the common digital nerves, protecting them with blunt retractors. Locate the previously divided FDS tendon of the donor finger.
- Withdrawal: Gently withdraw the FDS tendon through the palmar incision.
- Splitting the Tendon: Once delivered into the palm, the FDS tendon must be split longitudinally into four equal tails. Use a fresh #15 blade to divide the tendon along its natural fascicular planes. Ensure the splits extend far enough proximally to allow independent routing to each digit without creating a restrictive tether at the lumbrical origins.
Step 3: Recipient Site Incisions and Routing
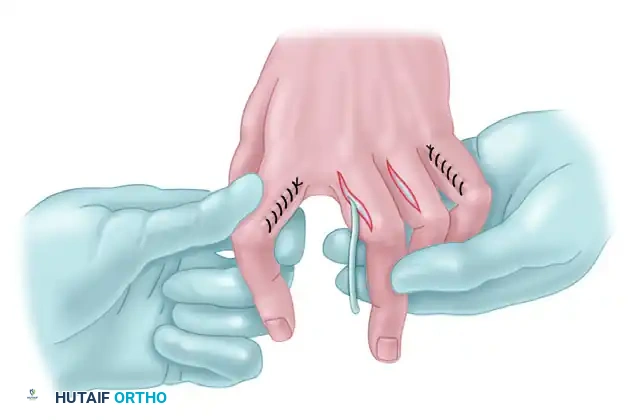
- Digital Incisions: Make a longitudinal incision, about 2.5 cm long, on the radial side (and slightly dorsal) of the proximal phalanx of each finger requiring transfer (typically the index, long, ring, and little fingers, excluding the donor digit if it does not require intrinsic substitution).
- Exposure: Deepen these incisions to identify the extensor aponeuroses, specifically isolating the lateral bands and the oblique fibers.
- Lumbrical Canal Routing: This is a critical biomechanical step. The tendon tails must pass volar to the deep transverse metacarpal ligament to replicate the moment arm of the native lumbricals.
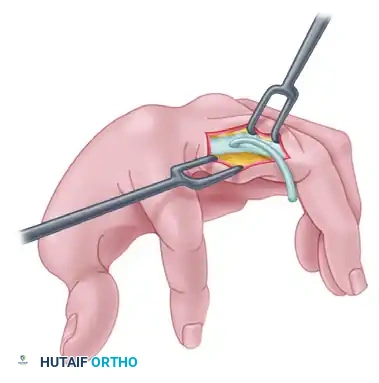
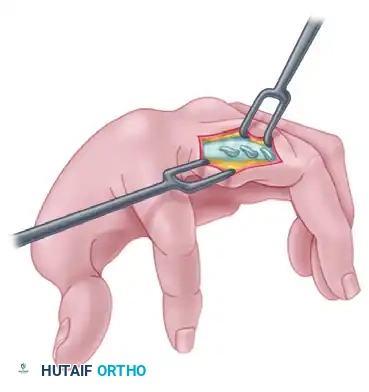
- Passage: With a narrow instrument, a wire loop, or a specialized tendon carrier (e.g., a Brand tendon passer), pass each tail of the tendon from the palmar incision, through the respective lumbrical canal, and over the oblique fibers of the extensor aponeurosis to its dorsum.
🚨 Surgical Warning: Lumbrical Canal Obstruction
Passage through the lumbrical canals should be smooth and effortless. If any obstruction or resistance is met, do not force the instrument. Withdraw and redirect the tendon carrier. Forcing the instrument can damage the digital neurovascular bundles or create false passages that will lead to severe postoperative adhesions.
Step 4: Insertion and Weaving
The specific insertion of the tendon slips dictates the functional outcome. According to the modified technique described by White, the slips are sutured to the appropriate lateral bands.
- Order of Fixation: To ensure balanced tensioning, follow a specific sequence. First, one slip of the graft is sutured to the ulnar lateral band of the index finger (1). Subsequently, one slip each is routed to the radial lateral band of the little (2), long (3), and ring (4) fingers, in that specific order.

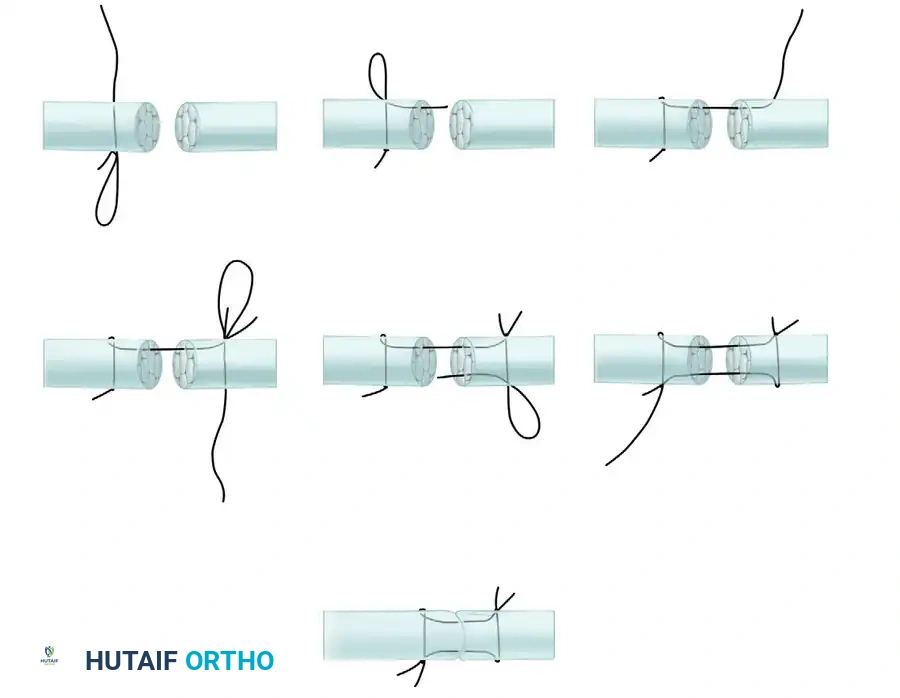
- Weaving Technique: The slip of the graft is woven into the lateral band to ensure a robust, pull-out resistant repair. Create a small slit in the lateral band, pass the FDS tail through it, and fold it back upon itself.
Step 5: Tensioning and Fixation
Tensioning is arguably the most unforgiving aspect of tendon transfer surgery. Incorrect tensioning will result in either a recurrent claw deformity (under-tensioned) or an intrinsic-plus deformity (over-tensioned).
- Positioning for Tensioning:
- Set the wrist at 30 to 45 degrees of dorsiflexion (flexion/extension parameters vary slightly by author; White recommended 45 degrees of dorsiflexion for optimal tenodesis effect during setting).
- Set the metacarpophalangeal (MCP) joints at 70 to 90 degrees of flexion.
- Maintain the interphalangeal (IP) joints in neutral (0 degrees of extension).
- Suturing: With the hand held strictly in this posture, suture each tail to the aponeurosis under some tension using non-absorbable braided sutures (e.g., 3-0 or 4-0 braided polyester).
- Excision of Redundancy: Bury the ends of the tendon. Usually, 2.5 cm or more of redundant tendon must be excised to maintain a clean, low-profile repair that will not catch on the overlying skin.
The Brooks Modification: Preventing Swan Neck Deformity
A critical evolution of the Bunnell transfer addresses a severe potential complication: the iatrogenic swan neck deformity.
If a patient has highly supple PIP joints, transferring a powerful muscle like the FDS directly into the lateral bands can exert excessive extension force on the PIP joint, driving it into hyperextension (swan neck).
🔪 Clinical Pearl: The Brooks Insertion
To prevent the development of hyperextension deformities at the PIP joints, Brooks recommended attaching each transfer to the flexor pulley (A1 or A2) or the periosteum of the proximal phalanx, rather than the lateral band.
By inserting the tendon into the proximal phalanx, the transfer acts exclusively as an MCP joint flexor. It prevents MCP hyperextension, allowing the native EDC to extend the IP joints via the tenodesis effect, without the risk of overpowering the PIP joint into a swan neck posture. This modification is highly preferred in patients with a positive Bouvier test and hypermobile joints.
Postoperative Care and Rehabilitation
The success of an FDS transfer relies heavily on meticulous postoperative immobilization and a structured, phased rehabilitation program. The transferred muscle must undergo cortical re-education to fire in its new phase (acting as an MCP flexor/IP extensor rather than an independent digit flexor).
Phase 1: Immobilization (Weeks 0-3)
Immediately following closure of the incisions, the hand is immobilized in a bulky, rigid plaster or fiberglass cast.
* Wrist: Neutral to 30 degrees of flexion (or 45 degrees dorsiflexion depending on the specific tensioning philosophy utilized intraoperatively, as noted by White).
* MCP Joints: 70 to 90 degrees of flexion.
* IP Joints: Full extension (0 degrees).

Phase 2: Splinting and Early Motion (Weeks 3-6)
At exactly 3 weeks postoperative, the rigid cast is removed.
1. Gutter Splints: Each finger is individually splinted with a plaster or thermoplastic gutter splint holding the IP joints in a neutral position.
2. Active Motion: Movement of the metacarpophalangeal joints is initiated. The patient is instructed to actively flex the MCP joints.
3. Synergistic Re-education: Resisted active extension of the wrist is highly encouraged. Because the FDS is a volar muscle, extending the wrist naturally increases tension on the flexor compartment (tenodesis), assisting the patient in learning how to fire the transferred FDS to flex the MCP joints.
Phase 3: Weaning and Strengthening (Weeks 6+)
The finger splints are removed for therapy sessions and reapplied daily. They are gradually weaned during the day as the patient demonstrates independent ability to maintain IP extension without MCP hyperextension. Night splinting may continue for up to 12 weeks to protect the transfer from stretching during sleep. Heavy grasping and forceful intrinsic activities are restricted until 10 to 12 weeks postoperative.
Complications and Pitfalls
- Swan Neck Deformity: As discussed, over-tensioning the lateral band insertion in a hypermobile hand leads to PIP hyperextension. Management requires surgical revision, often converting the insertion to a Brooks-style proximal phalanx attachment or performing a PIP volar dermodesis.
- Tendon Adhesions: The extensive routing through the palmar fascia and lumbrical canals makes this transfer prone to scarring. Meticulous hemostasis, gentle tissue handling, and strict adherence to the 3-week mobilization protocol are mandatory to prevent tethering.
- Donor Digit Stiffness: Harvesting the FDS can lead to PIP joint stiffness or a mild recurvatum deformity in the donor finger. Preserving the A2 and A4 pulleys during harvest minimizes this risk.
- Under-tensioning: If the transfer is sutured too loosely, the claw deformity will recur as the tendon stretches during the healing phase. It is generally safer to err on the side of slight over-tensioning at the MCP joint, as the transfer will naturally stretch out slightly over the first year.
Conclusion
The modified Bunnell Flexor Digitorum Sublimis transfer remains a highly reliable, powerful, and versatile procedure for the correction of the intrinsic minus hand. By mastering the intricate anatomy of the lumbrical canals and extensor aponeurosis, and by judiciously applying modifications like the Brooks proximal phalanx insertion, the orthopedic surgeon can predictably restore the functional digital cascade and significantly improve the patient's grip strength and hand mechanics.
You Might Also Like