Surgical Treatment of Injection Injuries in the Hand
Introduction and Epidemiology
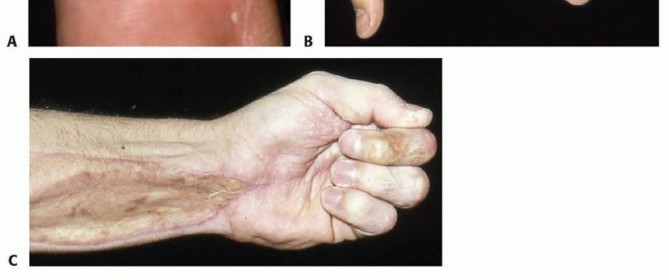
High-pressure injection injuries of the hand represent a catastrophic orthopedic and hand surgery emergency. Despite an initial clinical presentation that frequently appears innocuous, these injuries carry a profoundly high risk of morbidity, irreversible tissue necrosis, and eventual amputation. The fundamental mechanism involves industrial equipment capable of generating extreme hydrostatic pressures—typically ranging from 2,000 to 12,000 pounds per square inch (psi). To contextualize this kinetic force, the pressure required to breach intact human skin is merely 100 psi. Consequently, the kinetic energy transferred during a high-pressure injection event is more than sufficient to drive foreign material, debris, and toxic solvents deep into the fascial planes, tendon sheaths, and neurovascular bundles of the upper extremity.
The substances typically injected in these industrial accidents vary widely, dictating the subsequent pathophysiological cascade. The most commonly encountered materials include grease, oil, oil-based paints, paint thinners, diesel fuel, hydraulic fluid, and cement. Less frequent, yet well-documented, cases involve molten metal, dry cleaning solvents, fluorocarbons, and veterinary vaccines. The pathognomonic hallmark of a high-pressure injection injury is a deceptively small, benign-appearing superficial puncture wound that drastically underestimates the true extent of deep tissue infiltration, chemical contamination, and structural destruction.

Epidemiologically, these injuries occur most frequently in young men, particularly those employed as manual laborers in industrial, automotive, or construction settings. The non-dominant index finger is the most commonly involved digit, reflecting the mechanics of holding a nozzle or wiping a tip while the dominant hand triggers the device. Historically, it was a prevailing misconception that these injuries primarily affected inexperienced workers. However, contemporary occupational health studies demonstrate that the mean time on the job for affected individuals is approximately 11 years. This suggests that complacency, circumvention of safety protocols, and over-familiarity with dangerous equipment play significant roles in the etiology of these accidents. Typical injury scenarios include grasping pressurized tubing that possesses a microscopic break in the seal, or attempting to manually unclog the nozzle of a high-pressure injector or paint gun with the safety guard removed.
It is crucial for the evaluating surgeon to distinguish high-pressure industrial injection injuries from iatrogenic contrast extravasation injuries. With the increasing utilization of power contrast injection in computed tomography (CT), contrast extravasation may technically be classified under injection injuries of the upper extremity. However, the pressures involved in medical imaging are generally much lower (approximately 100 to 150 psi), the associated injuries are typically located more proximally in the forearm or antecubital fossa, and the natural history is generally benign. Surgical intervention for contrast extravasation is rarely required, contrasting sharply with the absolute emergent surgical mandate for high-pressure industrial injections.
Surgical Anatomy and Biomechanics
Understanding the surgical anatomy and biomechanics of the hand is paramount for predicting the trajectory of the injected substance, anticipating the zones of injury, and executing a comprehensive surgical debridement. The dissemination of fluid within the hand strictly follows the path of least resistance, which is dictated by the complex network of fascial septa, synovial sheaths, and neurovascular canals.
Fascial Planes and Synovial Sheaths
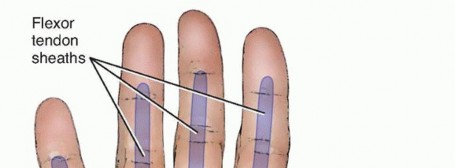
When a high-pressure jet breaches the volar skin of a digit, the fluid rapidly distends the subcutaneous tissues before encountering the rigid boundary of the flexor tendon sheath. If the sheath is penetrated—which occurs in the majority of high-pressure cases—the fluid will travel proximally along the synovial space with minimal resistance. The anatomical continuity of these sheaths dictates the proximal extent of the injury:
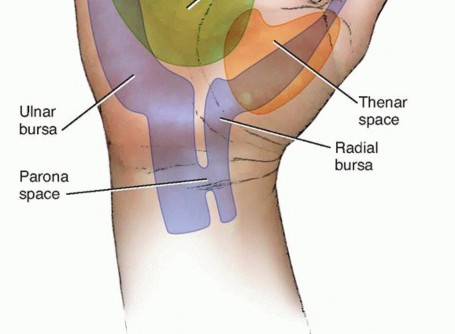
* Index, Long, and Ring Fingers: The flexor tendon sheaths of these central digits typically terminate at the level of the distal palmar crease. Injections into these digits will often rupture proximally, extravasating into the midpalmar space (long and ring fingers) or the thenar space (index finger).
* Thumb and Small Finger: The flexor pollicis longus (FPL) sheath (radial bursa) and the small finger flexor sheath (ulnar bursa) frequently communicate directly with Parona's space (the deep fascial space in the distal forearm, located between the pronator quadratus and the deep flexor tendons). Consequently, an injection into the thumb or small finger can rapidly track through the carpal tunnel and deposit highly toxic material into the deep volar compartment of the forearm, necessitating an extensile forearm decompression.
Pathogenesis of Tissue Destruction
Two distinct but synergistic pathogenic mechanisms are responsible for the severe morbidity associated with high-pressure injection injuries:
1. Mechanical Injury (Acute Compartment Syndrome): This is a direct result of the injected material acting as a high-velocity projectile. The mechanical destruction is a function of the fluid's viscosity, velocity, and volume. The sudden introduction of a large volume of non-compressible fluid into the closed, inelastic compartments of the digit leads to an immediate and profound increase in compartmental interstitial pressure. This rapidly surpasses capillary perfusion pressure, resulting in acute compartment syndrome, mechanical ischemia, and subsequent ischemic necrosis of the digital tissues.
2. Inflammatory Host Response (Chemical Necrosis): This is driven by the chemical and irritant properties of the injected material. Organic solvents, such as paint thinners, turpentine, and oil-based paints, are highly lipophilic and profoundly cytotoxic. They dissolve lipid cell membranes, causing rapid saponification and liquefaction necrosis of the subcutaneous fat, alongside profound chemical thrombosis of the digital vessels. Conversely, substances like grease and hydraulic fluid are less acutely cytotoxic but provoke a severe, chronic granulomatous inflammatory response. If not meticulously debrided, this leads to the formation of oleomas, intense fibrosis, tendon adherence, and profound, irreversible stiffness.

Indications and Contraindications
The management of high-pressure injection injuries is almost universally operative. The innocuous appearance of the entry wound must never deter the orthopedic surgeon from proceeding with emergent surgical exploration. Time to the operating room is the most critical modifiable prognostic factor.
Surgical Decision Making
The risk of amputation increases exponentially with delayed surgical intervention. Debridement should ideally occur within 6 hours of the injury to halt the ischemic and chemical cascade.
| Management Strategy | Indications | Contraindications |
|---|---|---|
| Emergent Surgical Debridement | High-pressure injection of paint, solvents, grease, oil, or unknown industrial substances; Clinical signs of compartment syndrome; Neurovascular compromise (pallor, pulselessness, altered two-point discrimination). | Extreme hemodynamic instability precluding anesthesia (exceedingly rare in this demographic). |
| Primary Amputation | Massive infiltration of highly toxic solvents (e.g., oil-based paint) with irreversible digital ischemia and mummification on presentation; Delayed presentation (>48 hours) with established frank gangrene. | Viable digit with intact capillary refill and sensation; Patient refusal; Isolated distal phalanx involvement where salvage is functionally superior. |
| Non-Operative Observation | Low-pressure (<100 psi) water or air injection with absolutely normal serial neurovascular exams (Highly controversial and requires extremely close inpatient observation); Iatrogenic CT contrast extravasation. | High-pressure industrial injuries; Any injection of organic solvents, paint, or grease; Pain out of proportion to exam. |
Pre Operative Planning and Patient Positioning
Thorough preoperative evaluation and meticulous planning are essential for optimizing outcomes in these complex and unforgiving injuries.
Clinical Evaluation
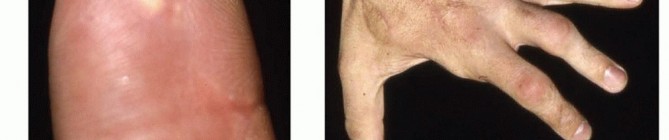
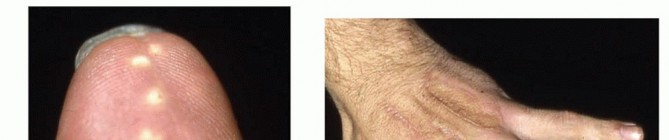
The history must ascertain the exact substance injected, the estimated pressure of the device, the time elapsed since the injury, and the precise mechanism. Physical examination often reveals a pinpoint puncture wound, typically on the volar aspect of the non-dominant index finger or palm. The digit may appear swollen, tense, and pale. Pain out of proportion to the visible injury is a hallmark sign of acute compartment syndrome secondary to the injection. Sensory examination (static and moving two-point discrimination) must be documented carefully, as chemical neuropathy occurs rapidly.
Diagnostic Imaging
Standard posteroanterior, lateral, and oblique radiographs of the affected hand and forearm are mandatory prior to incision. Imaging serves multiple critical purposes:
* Identification of radiopaque substances (e.g., lead-based paints, cement, certain industrial greases).
* Detection of subcutaneous emphysema, which effectively outlines the proximal extent of the injection track and helps plan the surgical incisions.
* Evaluation of underlying osseous structures, though fractures are exceedingly rare in this specific mechanism unless direct blunt trauma also occurred.
Medical Optimization
Preoperative medical management must be initiated immediately upon presentation in the emergency department:
* Tetanus Prophylaxis: Administer updated tetanus toxoid and immune globulin as indicated by immunization history.
* Antibiotic Therapy: Initiate broad-spectrum intravenous antibiotics immediately. Coverage should target typical skin flora (Staphylococcus and Streptococcus species) as well as gram-negative organisms and anaerobes, given the highly contaminated nature of industrial equipment.
* Analgesia and Absolute Contraindication to Digital Blocks: Systemic intravenous analgesia is required. Digital blocks are strictly contraindicated. The introduction of additional volume (local anesthetic) into an already distended, inelastic digital compartment will exacerbate the elevated interstitial pressure, precipitating or worsening acute digital ischemia by completely occluding arterial inflow.
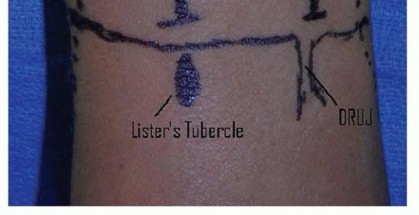
Patient Positioning and Tourniquet Management
The patient is positioned supine with the affected upper extremity extended on a radiolucent hand table. Regional (axillary or supraclavicular block) or general anesthesia is preferred to allow for proximal extension of the incision into the forearm if necessary.
Tourniquet Considerations: A pneumatic tourniquet is applied to the upper arm to provide a bloodless field. Crucially, the extremity must not be exsanguinated with an Esmarch bandage. Wrapping the arm tightly with an Esmarch will force the injected toxic material further proximally into the uninjured fascial planes of the hand and forearm, converting a localized injury into a catastrophic regional one. Instead, the arm should be exsanguinated by simple gravity elevation for 3 to 5 minutes prior to tourniquet inflation.
Detailed Surgical Approach and Technique
The surgical objective is radical, thorough decompression of all involved compartments and meticulous microscopic excision of all foreign material and necrotic tissue. This is not a simple irrigation; it is an aggressive oncologic-style debridement of dead and contaminated tissue.
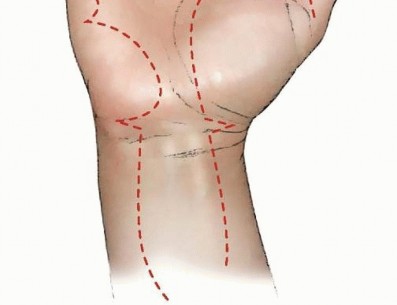
Incision and Exposure
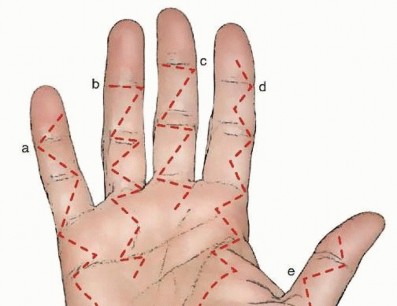
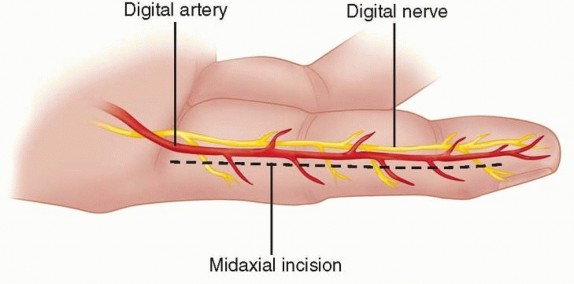
The surgical approach must be extensile. For digital involvement, a mid-lateral incision or a volar Bruner (zigzag) incision is utilized. The incision must incorporate the puncture site, which is elliptically excised to remove the heavily contaminated skin edges.
* Mid-lateral Approach: Placed dorsal to the neurovascular bundle (connecting the apices of the flexion creases), providing excellent exposure of the flexor tendon sheath while minimizing volar scar contracture.
* Bruner Incisions: Provide wide, direct exposure of the volar structures. Care must be taken to ensure the apices of the flaps do not cross the flexion creases perpendicularly to avoid disabling flexion contractures.
If the injection tracks proximally, the incisions must be extended into the palm, adhering to the principles of carpal tunnel and palmar space exposure. If Parona's space is involved (common with thumb and small finger injections), a standard volar forearm approach (extensile carpal tunnel incision extending proximally across the wrist creases) is mandatory.
Dissection and Debridement
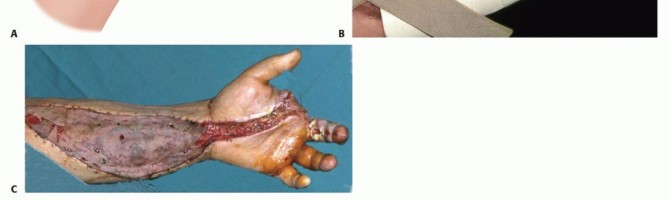
Once the skin flaps are elevated, the true, devastating extent of the injury becomes apparent. The subcutaneous fat is often heavily impregnated with the injected substance and may already show signs of necrosis.
1. Tissue Excision: All non-viable tissue, particularly the infiltrated subcutaneous fat, must be sharply excised. Fat undergoes rapid saponification and necrosis when exposed to industrial solvents.
2. Neurovascular Bundle Management: The digital nerves and arteries must be carefully identified and protected. If the substance has tracked along the neurovascular bundle, meticulous microscopic debridement is required. In cases where toxic solvents have infiltrated the epineurium, an epineurotomy under loupe or operating microscope magnification may be necessary to decompress the nerve fascicles and remove the chemical irritant. This carries a risk of iatrogenic nerve injury but is often necessary to salvage nerve function.
3. Flexor Tendon Sheath: The flexor tendon sheath must be opened longitudinally. If the substance is confined within the sheath, the crucial biomechanical pulleys (A2 and A4) should be preserved if possible, while the membranous portions and expendable pulleys (A1, A3, A5) are excised to allow for thorough irrigation. However, if the A2 or A4 pulleys are heavily infiltrated, necrotic, or compromised by solvent, they must be sacrificed to ensure adequate debridement; a live, functional finger without an A2 pulley is infinitely preferable to an amputated digit.
Irrigation and Wound Management
Following macroscopic sharp debridement, the surgical bed is subjected to copious irrigation. Low-pressure pulsatile lavage or gravity irrigation with several liters of normal saline is recommended to dilute and mechanically wash away residual chemical irritants. Avoid high-pressure lavage, which can inadvertently drive microscopic particles deeper into adjacent healthy tissues.
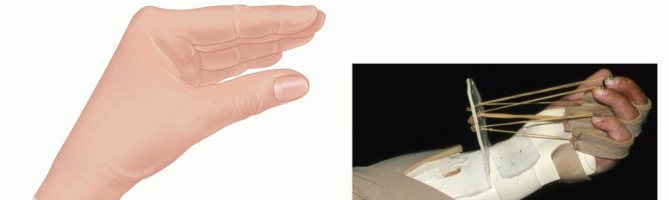
Closure: The wounds must never be closed primarily. Primary closure traps residual inflammatory mediators, ongoing edema, and necrotic debris, inevitably leading to deep space infection, progressive ischemia, and a drastically increased risk of amputation. The wounds are left open or loosely approximated with vessel loops (the "shoelace" technique) to prevent skin flap retraction while allowing for unimpeded drainage. A bulky, non-adherent, absorptive dressing is applied, and the hand is splinted in a safe position (intrinsic plus: wrist extended 30 degrees, MCP joints flexed 70-90 degrees, IP joints fully extended).
A mandatory second-look debridement is scheduled for 48 to 72 hours postoperatively to assess ongoing tissue viability and perform further excision if demarcation has occurred.
Complications and Management
The complication profile for high-pressure injection injuries is exceptionally severe, reflecting the devastating nature of the initial mechanical trauma compounded by chemical toxicity.

Digital Amputation
Amputation is the most feared and frequently encountered complication. The rate of amputation is intrinsically linked to the type of substance injected and the delay in surgical intervention. Organic solvents, particularly oil-based paints and paint thinners, carry the highest amputation rates, often exceeding 50% to 80% in historical cohorts. These substances cause immediate, irreversible liquefaction necrosis and profound thrombosis of the digital microvasculature. Conversely, grease and water carry lower amputation rates (approximately 20% and <5%, respectively), though they still require aggressive surgical management to prevent late functional loss.

Summary of Complications
| Complication | Incidence/Risk Factors | Management and Salvage Strategies |
|---|---|---|
| Amputation | Highest with paint/solvents (>50%); Delayed surgery (>10 hours). | Early recognition of irreversible ischemia; Ray amputation to optimize hand function and pinch grip; Prosthetic fitting. |
| Severe Stiffness | Nearly universal due to massive fibrosis, oleoma formation, and tendon sheath destruction. | Aggressive early hand therapy once wounds are stable; Tenolysis and capsulotomy as late reconstructive procedures (often with limited success). |
| Infection | Polymicrobial; High risk with delayed debridement, retained foreign material, or primary wound closure. | Serial debridement; Culture-directed IV antibiotics; Strict avoidance of primary closure. |
| Chronic Pain / CRPS | Common due to severe nerve irritation, chemical neuritis, and epineural fibrosis. | Multidisciplinary pain management; Stellate ganglion blocks; Desensitization therapy; Neuromodulators (Gabapentinoids). |
| Cold Intolerance | Secondary to digital vessel thrombosis and sympathectomy effect from nerve injury. | Thermal protection; Calcium channel blockers (nifedipine) in severe cases; Often permanent and highly debilitating. |
Post Operative Rehabilitation Protocols
The postoperative phase demands a delicate balance between meticulous wound management and the prevention of catastrophic hand stiffness.
Wound Care and Soft Tissue Coverage
Following the second-look debridement (and subsequent debridements as dictated by tissue viability), definitive wound management is planned.
* Negative Pressure Wound Therapy (NPWT): May be utilized to manage exudate, promote robust granulation tissue, and reduce edema. However, NPWT is contraindicated if there is exposed tendon without paratenon or exposed neurovascular structures, as it can cause desiccation and necrosis of these vital tissues.
* Delayed Primary Closure: Rarely possible due to the extent of tissue excision and persistent postoperative edema.
* Skin Grafting and Flaps: Full-thickness skin grafts or local/regional flaps (e.g., cross-finger flaps, reverse radial forearm flaps) may be required to cover exposed vital structures once the wound bed is definitively clean, uninfected, and granulating.
Hand Therapy
Rehabilitation must be initiated as soon as the soft tissue envelope permits. The intense inflammatory response generated by the injected substance inevitably leads to dense, unyielding adhesions between the flexor tendons, neurovascular bundles, and surrounding fascia.
* Early Motion: Active and passive range of motion exercises are critical. Dynamic splinting may be employed to counteract flexion contractures that rapidly develop.
* Edema Control: Compressive garments (once wounds are closed and healed), strict elevation, and retrograde massage.
* Desensitization: Crucial for managing the hypersensitivity that frequently follows chemical neuropathy and surgical exploration.
Surgeons must counsel patients extensively from the outset that the final functional outcome will likely involve some degree of permanent stiffness, sensory deficit, and cold intolerance, regardless of the excellence of surgical execution and therapeutic care.
Summary of Key Literature and Guidelines
The academic literature surrounding high-pressure injection injuries consistently reinforces a set of core principles that dictate surgical decision-making and patient counseling.
Determinants of Morbidity
Extensive retrospective reviews and meta-analyses have solidified the three primary determinants of morbidity and amputation risk:
1. Type of Substance Injected: This is the single most critical prognostic factor. Organic solvents (paint, thinners, fuel) induce a violent chemical necrosis that rapidly destroys tissue viability, leading to amputation rates historically reported between 50% and 80%. In contrast, grease and hydraulic fluids cause a chronic, space-occupying granulomatous reaction (oleoma) that, while destructive, results in lower immediate amputation rates (15% to 25%) if adequately and emergently debrided.
2. Delay in Treatment: The concept of "time is tissue" is paramount. Classic literature frequently cites a "6-hour rule," suggesting that surgical debridement performed within 6 hours of injury significantly reduces the risk of amputation. More recent multivariate analyses indicate that while the 6-hour window is ideal, any delay beyond 10 hours results in a precipitous increase in amputation rates, particularly with solvent injections.
3. Anatomic Location and Volume: Injections into the digital pulp or tendon sheaths have worse prognoses due to the confined, inelastic nature of these spaces, which rapidly succumb to compartment syndrome. Larger volumes of injected material correlate directly with the extent of proximal tracking and systemic toxicity.
Standard of Care Guidelines
The universally accepted standard of care among orthopedic and hand surgeons dictates that high-pressure injection injuries are absolute surgical emergencies. The initial benign appearance of the puncture wound is a dangerous clinical trap. Non-operative management is virtually never indicated for industrial injections. The surgical approach must be aggressive, prioritizing wide extensile exposure, radical excision of chemically impregnated tissue, copious low-pressure irrigation, and open wound management to mitigate the devastating sequelae of these injuries.
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
You Might Also Like

Chapter Index
Back to Master Guide