Surgical Management of Web Space and Deep Fascial Space Infections of the Hand
Key Takeaway
Hand space infections, including collar button abscesses and deep fascial space purulence, require urgent surgical intervention to prevent devastating functional loss. This comprehensive guide details the complex pathoanatomy, clinical presentation, and step-by-step surgical drainage techniques for web space, midpalmar, thenar, and Parona space infections. Mastery of these approaches ensures optimal eradication of infection while preserving vital neurovascular and tendinous structures.
INTRODUCTION TO HAND COMPARTMENT INFECTIONS
Infections of the hand represent a critical orthopedic emergency. The complex, compartmentalized fascial architecture of the hand dictates the predictable, yet potentially devastating, pathways through which purulence can spread. Before the advent of modern antimicrobial therapy, deep fascial space infections frequently resulted in catastrophic functional loss or amputation. Today, while systemic antibiotics have reduced the incidence of rampant spread, the cornerstone of management remains prompt, meticulous surgical decompression and drainage.
Understanding the precise anatomical boundaries of the web spaces, the deep palmar spaces (midpalmar and thenar), and the potential spaces of the distal forearm (Parona’s space) is paramount. Failure to recognize the extent of an infection or inadequate surgical drainage can lead to tendon necrosis, osteomyelitis, stiffening joint contractures, and systemic sepsis.
WEB SPACE INFECTION (COLLAR BUTTON ABSCESS)
Pathoanatomy and Biomechanics
A web space infection, classically referred to as a "collar button" or bouton en chemise abscess, typically localizes in one of the three fat-filled interdigital spaces. These spaces are situated just proximal to the superficial transverse metacarpal ligament (natatory ligament) at the level of the metacarpophalangeal (MCP) joints.
The pathogenesis frequently begins with a penetrating injury or an infected palmar blister/callus, particularly in manual laborers. Because the palmar skin and underlying palmar aponeurosis are thick, unyielding, and firmly anchored by vertical fascial septa, the accumulating purulence follows the path of least resistance. It tracks dorsally through the web space, creating an hourglass-shaped abscess with a smaller palmar component and a larger, more obvious dorsal component.
Clinical Pearl: The dorsal swelling in a collar button abscess is often a "decoy." While the dorsum of the hand appears dramatically swollen and erythematous due to the loose dorsal skin accommodating the fluid, the primary nidus and the most dangerous component of the abscess remain volar, deep to the palmar fascia.
If left untreated, the palmar component can rupture proximally, tracking along the lumbrical canal to invade the deep midpalmar space, converting a localized web space infection into a limb-threatening deep fascial space infection.
Clinical Presentation
Patients typically present with severe pain, throbbing, and swelling localized to the affected web space. The adjacent fingers are often held in an abducted position to maximize the volume of the web space and reduce tension. Erythema and fluctuance are predominantly noted on the dorsal aspect, but exquisite point tenderness will be elicited upon deep palpation of the palmar aspect of the web space.
Surgical Technique: Dual-Incision Drainage
Adequate drainage of a collar button abscess mandates a dual-incision approach to decompress both the palmar and dorsal components of the hourglass collection.
Step 1: Positioning and Preparation
* The patient is placed supine with the arm extended on a hand table.
* General anesthesia or a regional brachial plexus block is preferred. Local infiltration is contraindicated due to the risk of spreading the infection and inadequate anesthesia in acidic, infected tissues.
* A well-padded pneumatic tourniquet is applied to the proximal arm. Exsanguination should be performed by elevation rather than an Esmarch bandage to prevent proximal milking of purulence.
Step 2: The Dorsal Incision
* Make a 2 to 3 cm longitudinal incision on the dorsal surface of the web space, centered between the metacarpal heads.
* Carefully dissect through the subcutaneous tissues, avoiding injury to the dorsal sensory nerve branches and the dorsal venous network.
* Enter the abscess cavity and obtain cultures (aerobic, anaerobic, mycobacterial, and fungal).
Step 3: The Palmar Incision
* Make a separate palmar incision beginning just distal to the distal palmar crease, curving proximally.
* Surgical Warning: Never cross the palmar creases at a right angle. Perpendicular incisions across flexion creases inevitably lead to hypertrophic scarring and severe flexion contractures.
* Surgical Warning: Do not incise the web itself (the free edge of the skin between the digits). Incising the web directly leads to a devastating adduction contracture of the digits.
Step 4: Decompression and Irrigation
* Using blunt dissection (e.g., a curved hemostat), connect the palmar and dorsal incisions through the web space, staying superficial to the deep transverse metacarpal ligament.
* Thoroughly irrigate the cavity with copious amounts of sterile saline.
* If the cavity is large, a small Penrose drain or a sterile silicone loop may be passed loosely between the incisions to maintain patency and prevent premature skin closure.
DEEP FASCIAL SPACE INFECTIONS
The deep fascial spaces of the hand are potential spaces that become actual cavities only when distended by purulence or hemorrhage. They are anatomically defined by unyielding fascial borders, making them prone to compartment syndrome-like physiology when infected.
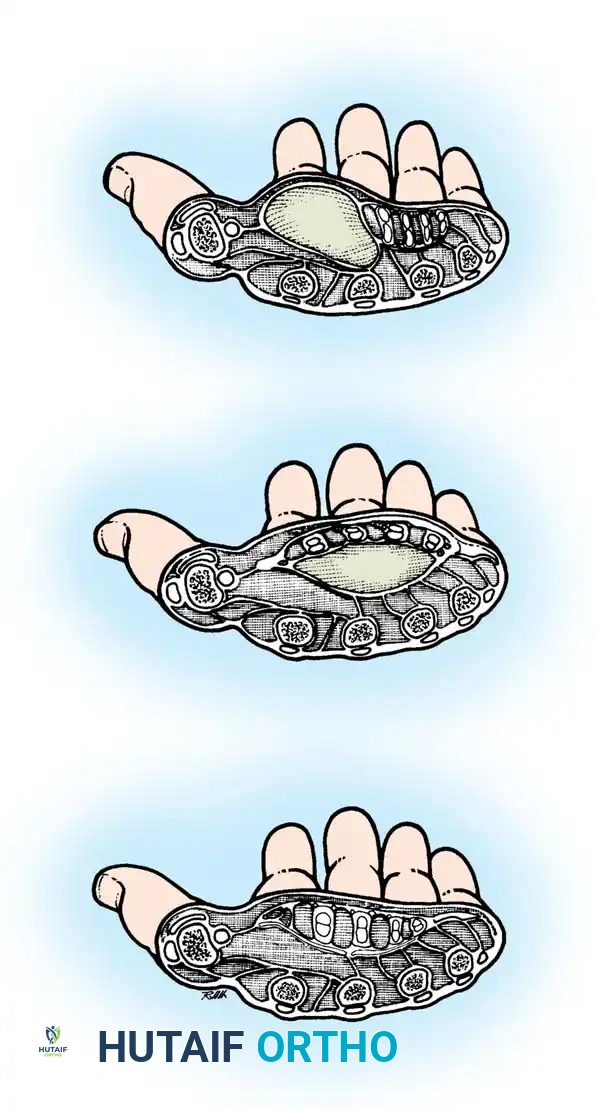
Anatomy of the Deep Spaces
The palmar fascial space lies deep to the flexor tendons and superficial to the fascia covering the metacarpals and interosseous muscles. This large area is divided into distinct compartments by the oblique septum of Legueu and Juvara, a fascial membrane that passes obliquely from the third metacarpal shaft to the fascia dorsal to the flexor tendons of the index finger.
- Middle Palmar Space: Located ulnar to the oblique septum. Its ulnar border is the hypothenar septum. It lies deep to the flexor tendons of the middle, ring, and small fingers, and superficial to the interosseous muscles of the 3rd and 4th spaces.
- Thenar Space: Located radial to the oblique septum. It lies deep to the flexor tendons of the index finger and the first lumbrical, and superficial to the adductor pollicis muscle. Its radial border is the fascia of the thenar musculature.
- Hypothenar Space: A tightly enclosed compartment bounded laterally by the hypothenar septum, dorsally by the fifth metacarpal, and volarly/medially by the hypothenar muscle fascia.
- Space of Parona: A potential space in the distal volar forearm. It is bordered dorsally by the pronator quadratus, laterally by the flexor pollicis longus (FPL), medially by the flexor carpi ulnaris (FCU), and volarly by the deep flexor tendons. It represents a proximal extension pathway for infections originating in the radial or ulnar bursae.
Pathogenesis and Clinical Presentation
Primary infections of these deep spaces are rare. They almost exclusively result from the secondary spread of adjacent infections, most notably neglected purulent flexor tenosynovitis, penetrating trauma, or proximal extension of a collar button abscess.
Middle Palmar Space Abscess:
Patients present with a profound systemic inflammatory response. The hand exhibits massive generalized swelling, often described as resembling an "inflated rubber glove." The normal palmar concavity is obliterated, bulging outward. Active and passive motion of the middle and ring fingers is severely restricted and exquisitely painful due to the proximity of the abscess to their flexor tendons and lumbricals.
Thenar Space Abscess:
The hallmark of a thenar space infection is massive, asymmetric swelling of the first web space and thenar eminence. The thumb is forced into abduction and extension to maximize compartment volume. The index finger is typically held in a flexed posture, and any attempt at active or passive motion of the index finger or thumb elicits severe pain.
Surgical Pitfall: Do not confuse a thenar space abscess with a superficial thenar subcutaneous abscess. A true thenar space abscess lies deep to the adductor pollicis and requires deep dissection for adequate drainage. Superficial drainage will fail to resolve the infection.
Surgical Drainage Techniques
Drainage of the Thenar Space
The thenar space can be approached via a volar or dorsal route, though the volar approach is most common.
- Incision: Make a curved incision in the palmar aspect of the thumb web, running parallel to the border of the first dorsal interosseous muscle, or along the medial side of the thenar crease.
- Nerve Protection: Extreme caution must be exercised at the proximal extent of the thenar crease to avoid injuring the recurrent motor branch of the median nerve (the "million-dollar nerve").
- Dissection: Avoid sharp, deep dissection. Once the skin and subcutaneous tissues are incised, use blunt dissection (e.g., spreading with a blunt hemostat) to penetrate the fascia and enter the thenar space anterior to the adductor pollicis.
- Evacuation: Obtain cultures, evacuate the purulence, and irrigate copiously.
Drainage of the Middle Palmar Space
- Incision: A transverse incision can be made parallel to the distal palmar crease, or a longitudinal incision can be made in the mid-palm, carefully avoiding perpendicular crossing of the creases.
- Dissection: Dissect bluntly between the flexor tendons (usually between the long and ring finger flexors) to enter the space deep to the tendons and superficial to the interosseous fascia.
- Protection: Protect the common digital neurovascular bundles, which lie superficial and between the flexor tendons.
Drainage of Parona’s Space
Infections in the space of Parona are typically associated with horseshoe abscesses spreading from the flexor tendon sheaths.
- Incision: Make a straight or slightly curved longitudinal incision on the volar forearm, beginning just proximal to the wrist flexion crease and slightly ulnar to the midaxial line. Extend proximally as needed for adequate exposure.
- Dissection: Incise the antebrachial fascia. Retract the flexor tendon mass and the median nerve radially. The ulnar neurovascular bundle must be identified and protected medially.
- Evacuation: The abscess cavity lies immediately superficial to the pronator quadratus. Drain the purulence, obtain cultures, and irrigate thoroughly.
- Drain Placement: Due to the depth and volume of this space, placement of a Penrose drain or a perforated irrigation tube is highly recommended to prevent premature closure and reaccumulation.
SUBAPONEUROTIC SPACE INFECTIONS
Anatomy and Etiology
The dorsal aspect of the hand contains two distinct potential spaces: the dorsal subcutaneous space (superficial to the extensor tendons) and the dorsal subaponeurotic space (deep to the extensor tendons and superficial to the metacarpals and dorsal interosseous muscles).
Subaponeurotic space infections are typically caused by direct penetrating trauma (e.g., human bites, puncture wounds) or local spread from a severe palmar infection tracking dorsally.
Clinical Evaluation
Patients present with profound dorsal hand swelling, erythema, calor, and exquisite tenderness. A key differentiating clinical sign between a superficial cellulitis/subcutaneous abscess and a deep subaponeurotic abscess is painful finger extension. Because the extensor tendons form the roof of the subaponeurotic space, active or passive extension of the digits stretches the inflamed tissue, causing severe pain.
If the presence of an abscess is equivocal amidst severe cellulitis, needle aspiration under sterile conditions can confirm purulence. While ultrasound or MRI can delineate the fluid collection, they are rarely necessary and should not delay surgical intervention.
Surgical Drainage Technique
- Incision Placement: Most dorsal subaponeurotic abscesses can be adequately drained through a single longitudinal dorsal incision centered over the fluctuance.
- Dual Incisions: For massive collections spanning the entire dorsum, two parallel longitudinal incisions may be required. These are typically placed over the second metacarpal and between the fourth and fifth metacarpals.
- Skin Bridge Viability: If dual incisions are used, they must be kept relatively short (2 to 3 cm) and spaced widely apart to avoid compromising the vascularity of the intervening skin bridge.
- Dissection: Incise the skin and subcutaneous tissue. Avoid sharp deep dissection to prevent iatrogenic laceration of the extensor tendons or paratenon. Retract the extensor tendons laterally and use blunt dissection to enter the subaponeurotic space.
- Irrigation and Drainage: Thoroughly irrigate the cavity. If a significant "dead space" exists, a Penrose drain should be placed.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The surgical procedure is only the first phase of managing hand space infections. Postoperative care is equally critical to ensure eradication of the infection and restoration of hand function.
Wound Management:
* Wounds are universally left open to heal by secondary intention or for delayed primary closure. Primary closure of an infected hand space is strictly contraindicated.
* Apply a nonadherent contact layer (e.g., Xeroform or Adaptic) directly to the wound bed, followed by a bulky, highly absorbent gauze dressing.
Splinting and Positioning:
* The hand must be immobilized in a volar resting splint in the "safe position" (James position or intrinsic-plus position): wrist extended 20 to 30 degrees, MCP joints flexed 70 to 90 degrees, and interphalangeal (IP) joints in full extension.
* This position maintains the collateral ligaments of the MCP and IP joints at their maximal length, preventing devastating joint contractures during the inflammatory phase of healing.
* Strict elevation of the affected limb above the level of the heart is mandatory to reduce edema.
Medical Management:
* Empiric broad-spectrum intravenous antibiotics (covering MRSA, Streptococcus species, and gram-negative/anaerobic organisms if a bite or specific exposure is suspected) should be initiated immediately after intraoperative cultures are obtained.
* Antibiotic therapy is subsequently tailored based on final culture and sensitivity reports.
Rehabilitation:
* Dressings should be changed frequently (often daily or twice daily initially), with bedside irrigation as needed.
* Once the acute infection and purulent drainage are controlled (typically within 48 to 72 hours), the splint is removed for supervised, active range-of-motion exercises.
* Early involvement of a specialized hand therapist is crucial to prevent tendon adhesions and joint stiffness.
* If the wound is large but clean and granulating, delayed secondary closure or split-thickness skin grafting may be considered, though most incisions for hand infections heal excellently by secondary intention with minimal functional deficit.
===
You Might Also Like
