Postoperative Care and Web Space Reconstruction in Hand Surgery
Key Takeaway
Optimal postoperative care in hand surgery is paramount for restoring function and mitigating edema. This comprehensive guide details evidence-based protocols for dressing application, limb elevation, and rehabilitation. Furthermore, it provides step-by-step surgical techniques for addressing web space contractures using four-flap Z-plasties and dorsal flaps, ensuring orthopaedic surgeons and residents achieve superior clinical outcomes.
PRINCIPLES OF POSTOPERATIVE CARE IN HAND SURGERY
The ultimate success of any hand surgery is inextricably linked to the quality of postoperative care. Care after surgery must be meticulously managed so that tissues are allowed to heal optimally while the complex biomechanical functions of the affected extremity are restored as rapidly as possible. The postoperative phase begins in the operating room with the application of the surgical dressing and extends through structured rehabilitation.
The Biomechanics of the Surgical Dressing
The application of a hand dressing is not merely a protective measure; it is the first critical step in postoperative rehabilitation. A poorly applied dressing can lead to catastrophic complications, including ischemia, maceration, and irreversible joint stiffness.
The routine dressing should be applied systematically:
* Primary Layer (Contact Layer): A closely woven patch of nonadherent gauze, such as Xeroform (bismuth tribromophenate) or Adaptic (cellulose acetate), is placed directly over each incision. Granulation tissue cannot grow through this tightly woven material, preventing adherence and trauma during dressing changes. Furthermore, this layer prevents the wound from becoming macerated by allowing exudate to pass through to the secondary layers.
* Secondary Layer (Conformational Layer): After the hand has been positioned properly—typically in the "intrinsic plus" or "safe" position (metacarpophalangeal joints flexed 70°–90°, interphalangeal joints fully extended, and the wrist extended 20°–30°)—sponges moistened in sterile saline or a glycerin solution are carefully placed around the digits and incisions.
* Tertiary Layer (Padding and Splinting): A roll of cotton or synthetic sheet padding (e.g., Webril) is wrapped circumferentially around the hand and forearm. Finally, an appropriate splint of plaster or fiberglass is applied and secured with a 2-inch or 3-inch gauze bandage.
Clinical Pearl: Moist sponges are biomechanically superior to dry sponges in the immediate postoperative setting. They conform to the complex topographical contours of the hand more accurately, distribute compressive pressure more evenly, and actively promote the capillary absorption of blood and exudate, thereby minimizing hematoma formation.
Tourniquet Management and Immediate Elevation
Immediately before the pneumatic tourniquet is deflated, the hand must be kept constantly elevated. This critical step prevents the sudden engorgement of the vascular tree, mitigating immediate postoperative edema and reactive hemorrhage.
Elevation must be maintained rigorously for at least 48 hours postoperatively. Effective elevation requires the hand to be positioned above the level of the heart. This can be achieved by:
* Positioning the hand on a pillow resting on the patient's chest.
* Utilizing a specialized sling that positions the hand higher than the elbow.
* Employing light overhead suspension that elevates the hand and forearm while the elbow rests comfortably on the bed.
* Using a preformed, commercially available rubber sponge block.
* Pinning two pillows together over two rolled towels to create a stable, elevated trough.
Pediatric Considerations in Postoperative Care
Managing postoperative dressings in the pediatric population presents unique challenges. Splints and bandages on children have a high propensity to slip distally due to the conical shape of the pediatric forearm and the child's inherent noncompliance with immobilization.
To effectively control this, surgeons should apply a long-arm splint or cast, extending above the elbow, combined with a tube of stockinette that encloses the entire extremity. Adults and caregivers responsible for the child’s postoperative care must be thoroughly educated and proven competent in evaluating the vascular status of the fingers and hand (capillary refill, color, temperature, and turgor).
EDEMA MANAGEMENT AND REHABILITATION PROTOCOLS
Body activity inherently increases edema of the hand due to dependent positioning and increased cardiac output. Merely supporting the hand in a standard sling while the patient is ambulatory is highly ineffective for edema control.
Early Mobilization
Fingers that are not explicitly splinted for surgical reasons must be exercised immediately. Active range of motion (AROM) acts as a musculovenous pump, clearing protein-rich lymphatic fluid that would otherwise organize into fibrotic scar tissue. Furthermore, the shoulder is highly susceptible to becoming stiff, especially in older patients. Patients must be instructed to abduct and elevate the shoulder toward the head several times daily to prevent adhesive capsulitis.
Wound Inspection and Suture Removal
Although sutures are traditionally removed 10 to 14 days after surgery, hand surgery often dictates a modified timeline. Sutures may not require removal until the splint is officially discarded, which can be 3 to 4 weeks postoperatively in cases of tendon or ligament repair.
Complete redressing of wounds is generally unnecessary and disrupts the healing milieu, unless a hematoma or infection is clinically suspected. In such instances, the dressing must be opened under sterile conditions, the wound inspected, and the splint reapplied. Even when no complications are suspected, a routine wound inspection at approximately 7 days allows for the timely management of unexpected superficial infections or marginal skin necrosis.
The Role of Hand Therapy
Active use of the hand is the single most effective modality to reestablish motion after surgery. Physical therapy and occupational therapy techniques are indispensable.
Surgical Warning: Applying excessive heat to the hand and forcing passive manipulation of joints by the patient, therapist, or surgeon are strictly contraindicated. Forced passive motion induces microtrauma, exacerbates inflammation, and ultimately leads to increased fibrosis and stiffness.
The patient, therapist, and surgeon must function as a well-integrated team. The surgeon should take the lead in prescribing and monitoring the therapy program. Often, the best therapy is the patient’s usual work; if possible, patients should be offered the opportunity to return to work on a limited or modified-duty basis. This return to activities of daily living (ADLs) provides functional rehabilitation and yields significant beneficial psychological effects.
SURGICAL MANAGEMENT OF WEB SPACE CONTRACTURES
While general postoperative care dictates the overall recovery trajectory, specific reconstructive procedures require meticulous surgical execution. Web space contractures of the hand severely limit digit abduction and independent flexion/extension. They frequently result from trauma, burns, infection, or congenital syndactyly. Addressing these contractures requires precise local flap reconstruction.
First Web Space Contracture Reconstruction
The first web space is critical for thumb opposition, pinch, and grasp. Contractures here severely debilitate hand function. When the contracture is secondary to a narrow linear scar but possesses normal, elastic surrounding tissue, a four-flap Z-plasty is highly effective.
Indications and Biomechanics:
The standard 60-degree Z-plasty provides a 73% increase in length along the axis of the central limb. However, the four-flap Z-plasty (often utilizing 90-degree and 120-degree angles) provides a significantly broader and deeper release, making it the gold standard for severe first web space linear contractures.
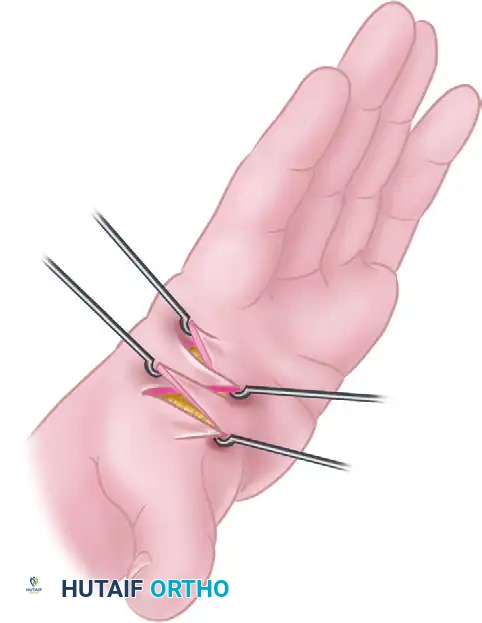
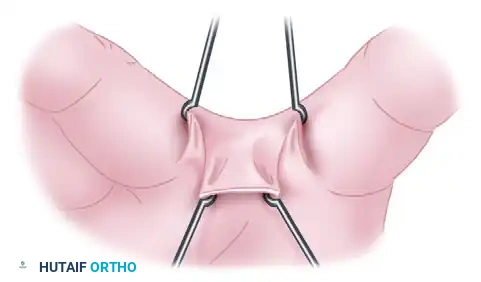
Surgical Technique: Four-Flap Z-Plasty (Figure 64-29)
- Preoperative Marking: The central limb of the Z-plasty is drawn directly over the crest of the linear scar contracture.
- Flap Outline: Four distinct flaps are outlined. The angles must be meticulously calculated to ensure adequate blood supply to the tips of the flaps. Broad-based flaps are essential to prevent distal necrosis.
- Incision and Elevation: The skin is incised down to the subcutaneous tissue. The flaps are elevated, taking care to preserve the subdermal plexus.
- Contracture Release: Once the flaps are elevated, any underlying fascial bands or fibrotic muscle fascia (e.g., over the adductor pollicis or first dorsal interosseous) must be released to allow full passive abduction of the thumb.
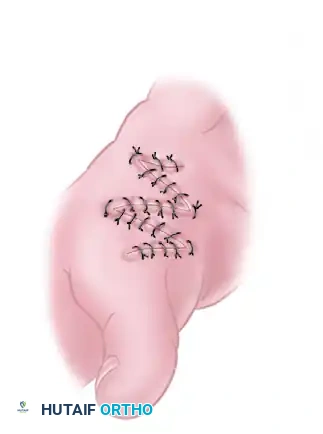
- Flap Transposition: The flaps are rotated and transposed into their new positions. The geometry of the four-flap system allows the tight linear scar to be broken up and the web space to be dramatically deepened.
- Closure: The flaps are sutured in place using fine non-absorbable sutures (e.g., 5-0 or 6-0 nylon) with minimal tension.
Second, Third, and Fourth Web Space Reconstruction
Linear contractures of the lesser web spaces (second, third, or fourth) restrict the independent spread of the fingers and can cause rotational deformities during flexion. When caused by a narrow scar, a dorsal flap technique is highly reliable.

Surgical Technique: Dorsal Flap Reconstruction (Figure 64-30)
- Assessment of the Contracture: The web space is evaluated under tension to identify the exact vector of the linear scar.
- Flap Design: A proximally based dorsal rectangular or trapezoidal flap is outlined over the dorsal aspect of the web space. Volar triangular flaps may also be designed to interdigitate with the dorsal flap.

- Elevation: The dorsal flap is elevated carefully. The dissection must remain superficial to the extensor paratenon and the dorsal sensory branches of the ulnar or radial nerves.
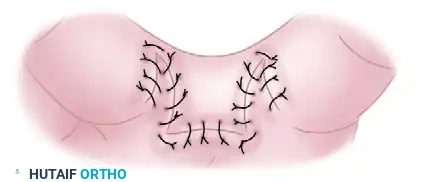
- Release and Rotation: The fibrotic bands causing the web contracture are excised. The natatory ligaments may require partial resection if they are involved in the fibrotic process. The dorsal flap is then advanced and rotated into the depth of the newly created web space.
- Suturing: The flaps are interdigitated and sutured. This breaks the linear line of tension and provides healthy, pliable skin at the deepest point of the commissure, preventing recurrence.
Postoperative Protocol for Web Space Reconstructions
Following web space reconstruction, the principles of postoperative care outlined earlier must be strictly enforced.
* Splinting: The hand is splinted with the web spaces maximally abducted (within the limits of skin tension) to prevent the flaps from contracting during the primary healing phase.
* Monitoring: Flap viability must be monitored closely. Any signs of venous congestion or arterial insufficiency warrant immediate intervention, which may include releasing a few sutures to relieve tension.
* Therapy: Once the flaps have healed (typically 2 to 3 weeks), aggressive active range of motion and the use of silicone elastomer web spacers are initiated to maintain the surgical correction and soften the maturing scar tissue.
By combining meticulous surgical technique with rigorous, evidence-based postoperative care, orthopaedic surgeons can ensure optimal functional recovery and high patient satisfaction in complex hand reconstructions.
You Might Also Like

