Surgical Management of Radial and Ulnar Bursae Infections
Key Takeaway
Infections of the radial and ulnar bursae, alongside septic arthritis of the finger joints, represent acute orthopedic emergencies. Due to the anatomical communication between the thumb and little finger flexor sheaths, infections can rapidly propagate, forming a horseshoe abscess. Prompt diagnosis, aggressive surgical incision and drainage, and targeted antimicrobial therapy are paramount to prevent irreversible cartilage destruction, tendon necrosis, and profound functional loss in the hand.
INTRODUCTION TO DEEP SPACE INFECTIONS OF THE HAND
Deep space infections of the hand, particularly those involving the radial and ulnar bursae and the interphalangeal joints, are severe orthopedic emergencies that threaten the functional viability of the upper extremity. The complex synovial anatomy of the hand facilitates smooth tendon gliding but paradoxically provides a low-resistance pathway for the rapid proximal and distal dissemination of purulent exudate.
Failure to recognize and aggressively treat these infections results in catastrophic complications, including tendon necrosis, irreversible cartilage destruction, osteomyelitis, and profound stiffness. Management mandates a thorough understanding of hand anatomy, prompt clinical and laboratory diagnosis, and emergent surgical intervention combining meticulous incision, drainage, and targeted antimicrobial therapy.
ANATOMY AND PATHOMECHANICS
The Radial and Ulnar Bursae
The radial and ulnar bursae are specialized tenosynovial sheaths enveloping the flexor tendons at the level of the wrist and palm.
* Radial Bursa: This structure is the proximal prolongation of the flexor pollicis longus (FPL) tendon sheath. It extends from the distal phalanx of the thumb, passes through the carpal tunnel, and terminates proximally at the level of the pronator quadratus.
* Ulnar Bursa: This bursa is formed by the proximal continuation of the flexor tendon sheath of the little finger (digit V). It envelops the superficial and deep flexor tendons of the index, long, ring, and little fingers as they pass through the carpal tunnel. It extends from the proximal palmar crease to the distal forearm, also terminating near the pronator quadratus.
The "Horseshoe Abscess" and Parona's Space
In approximately 50% to 80% of individuals, the radial and ulnar bursae communicate with each other within the carpal tunnel. This anatomical variant is of profound clinical significance. An infection originating in the thumb (radial bursa) can easily track proximally into the wrist and subsequently spread distally into the little finger (ulnar bursa), or vice versa. This contiguous spread of purulence is classically termed a "horseshoe abscess."
Furthermore, if the proximal outpouchings of these bursae rupture, the infection enters Parona's space—a deep fascial space in the distal forearm located between the pronator quadratus fascia dorsally and the flexor digitorum profundus tendons volarly.
💡 Clinical Pearl: Parona's Space Involvement
When evaluating a suspected horseshoe abscess, always palpate the distal volar forearm. Swelling, induration, and erythema proximal to the wrist crease strongly suggest rupture of the bursae into Parona's space, necessitating proximal forearm extension of your surgical incisions.
CLINICAL EVALUATION AND DIAGNOSIS
Flexor Tenosynovitis and Bursal Infections
Patients typically present with a history of a penetrating injury, though hematogenous spread can occur. The diagnosis of flexor tenosynovitis relies heavily on Kanavel’s four cardinal signs:
1. Fusiform swelling of the entire digit.
2. Severe pain along the course of the flexor tendon sheath with passive extension.
3. The digit is held in a resting posture of slight flexion.
4. Tenderness to palpation along the entire course of the flexor tendon sheath.
In cases of radial or ulnar bursa involvement, swelling and tenderness will extend into the palm and the volar wrist.
Finger Joint Infections (Septic Arthritis)
Finger joint infections (septic arthritis) usually result from the direct spread of infection from adjacent structures (such as a ruptured flexor sheath), direct penetrating trauma (e.g., human bite wounds or "fight bites" at the metacarpophalangeal joints), and, less commonly, hematogenous spread. When hematogenous spread occurs, identifying the primary source (e.g., endocarditis, indwelling catheters) is mandatory.
Clinical Presentation:
* The involved joints are swollen, exquisitely tender, and warm.
* The finger is usually held in slight flexion to maximize joint volume and minimize capsular tension.
* Careful inspection and palpation may reveal a fluctuant joint effusion.
* Active and passive motions are severely restricted and painful.
Diagnostic Arthrocentesis:
In addition to a comprehensive history, physical examination, and radiographic evaluation (to rule out foreign bodies, fractures, or established osteomyelitis), definitive diagnosis is accomplished by joint aspiration.
* Gross Appearance: Fluid obtained from a septic joint is usually turbid, opaque, or grossly purulent.
* Cell Count: The joint fluid white blood cell (WBC) count is typically greater than 50,000/mm³.
* Differential: The polymorphonuclear (PMN) leukocyte count is usually greater than 75%.
* Chemistry: Synovial fluid glucose is typically 40 mg/dL or less (or significantly lower than serum glucose).
* Microbiology: Gram stain and aerobic/anaerobic cultures must be obtained. Staphylococcus aureus is the most frequently isolated organism from septic hand and wrist joints, though Streptococcus species and Gram-negative bacilli are also common depending on the mechanism of injury.
⚠️ Surgical Warning: Cartilage Destruction
Septic arthritis is a surgical emergency. Proteolytic enzymes released by bacteria and the host's polymorphonuclear leukocytes can cause irreversible articular cartilage destruction within 24 to 48 hours. Delayed treatment guarantees secondary osteoarthritis and potential osteomyelitis of the underlying phalanx.
SURGICAL MANAGEMENT: INCISION AND DRAINAGE OF RADIAL AND ULNAR BURSAE
The primary goal of surgery is the complete evacuation of purulence, thorough irrigation of the synovial sheaths, and decompression of the involved spaces to restore tendon nutrition and prevent necrosis.
Preoperative Preparation
- Anesthesia: General anesthesia or regional block (axillary or supraclavicular). Local anesthesia is contraindicated due to the risk of spreading the infection and inadequate pain control during deep dissection.
- Positioning: Supine with the arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic upper arm tourniquet is essential for a bloodless field. Exsanguination should be performed by elevation rather than an Esmarch bandage to prevent proximal milking of the infection.
Surgical Technique: Step-by-Step Approach
1. Distal Incision (Radial Bursa):
* To drain the radial bursa, first make a mid-axial lateral incision along the proximal phalanx of the thumb, or utilize a volar Brunner (zigzag) incision.
* Carefully dissect through the subcutaneous tissue, identifying and protecting the digital neurovascular bundles.
* Expose the A1 and A2 pulleys. Open the flexor tendon sheath (bursa) at its distal end, typically between the A1 and A2 pulleys, preserving the pulleys to prevent tendon bowstringing.
* Obtain cultures immediately upon entering the sheath.
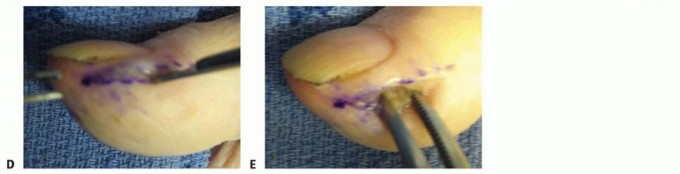
2. Proximal Propagation and Probe Placement:
* Introduce a blunt probe or a pediatric feeding tube into the distal opening of the sheath.
* Gently advance the instrument proximally along the flexor pollicis longus tendon toward the wrist.
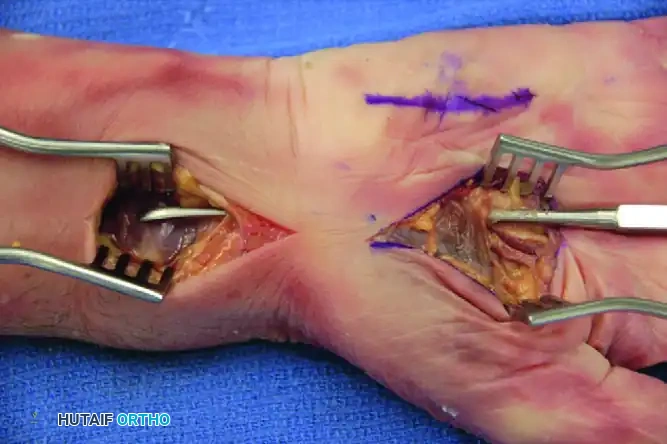
Figure 78-15: Passage of an instrument from the thenar space to the radial bursa in a cadaver specimen demonstrates how easily infections can propagate proximally. Notice the anatomical continuity allowing for the passage of the probe from the distal incision to the proximal wrist.
3. Proximal Incision and Decompression:
* Make a second incision over the proximal end of the probe at the volar wrist. This is typically an extended carpal tunnel incision, crossing the wrist crease obliquely to avoid flexion contractures.
* Release the transverse carpal ligament to decompress the carpal tunnel, as the swelling from the infected bursae frequently causes acute median nerve compression.
* Identify the proximal extent of the radial and ulnar bursae. If a horseshoe abscess is present, purulence will be evident surrounding the flexor tendons of the little finger as well.
4. Ulnar Bursa Drainage (If Involved):
* If the ulnar bursa is involved, make a mid-axial or Brunner incision over the little finger to open the distal extent of the ulnar bursa.
* Pass a catheter from the little finger proximally to the wrist incision to ensure patency and complete communication.
5. Irrigation and Catheter Placement:
* Copiously irrigate the sheaths from distal to proximal using normal saline.
* A 16-gauge pediatric feeding tube or a specialized irrigation catheter can be left in the sheath, exiting the distal incision, with a small drain left in the proximal incision. This allows for continuous or intermittent postoperative irrigation (typically 5-10 mL of saline every 2-4 hours for 24-48 hours).
SURGICAL MANAGEMENT: FINGER JOINT INFECTIONS (SEPTIC ARTHRITIS)
When pus has been identified in a finger joint, aggressive treatment with incision, drainage, and appropriate antibiotics must be pursued immediately to avoid cartilage destruction and osteomyelitis.
Surgical Technique: Joint Arthrotomy
1. Approach:
* DIP and PIP Joints: A dorsal approach is typically preferred. Make a dorsal longitudinal or gently curved incision over the joint.
* Split the extensor tendon longitudinally (for the PIP joint, between the central slip and lateral bands; for the DIP joint, splitting the terminal tendon) to access the joint capsule.
* MCP Joints: A dorsal longitudinal incision is made over the metacarpal head. The extensor hood is split longitudinally (usually on the ulnar side of the extensor digitorum communis tendon) to expose the joint capsule.
2. Arthrotomy and Synovectomy:
* Perform a generous arthrotomy. Send synovial fluid and tissue for aerobic, anaerobic, mycobacterial, and fungal cultures.
* Perform a thorough synovectomy, removing all fibrinous exudate and infected synovium.
* Inspect the articular cartilage. If the cartilage is intact, thoroughly irrigate the joint with several liters of normal saline.
3. Management of Advanced Destruction:
* If the joint and adjacent bone have been destroyed and require removal, simple irrigation is insufficient.
* Antibiotic Spacers: Antibiotic-impregnated polymethyl methacrylate (PMMA) spheres (beads) can be a useful adjunct. These beads deliver high local concentrations of antibiotics (typically Tobramycin or Vancomycin) to the dead space while systemic antibiotics are administered. This is a crucial step in preparing the site for delayed reconstruction, such as arthrodesis or bone grafting.
* Amputation: In severe cases where the joint is completely destroyed, osteomyelitis is extensive, and the soft tissue envelope is compromised, amputation may be required to salvage the hand and prevent systemic sepsis. Usually, little is lost by such an amputation because a chronically infected, stiff, and painful finger retains little to no useful function and acts as a mechanical hindrance to the rest of the hand.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Antimicrobial Therapy
- Empiric Therapy: Intravenous antibiotics should be initiated immediately after intraoperative cultures are obtained. Empiric coverage must include agents effective against MRSA (Methicillin-resistant Staphylococcus aureus) and Gram-negative organisms (e.g., Vancomycin and Ceftriaxone).
- Directed Therapy: Once culture and sensitivity results are finalized, antibiotic therapy is narrowed.
- Duration: Intravenous antibiotics are typically continued until clinical signs of infection (erythema, swelling, throbbing pain) significantly improve, followed by a transition to oral antibiotics. The total duration is usually 2 to 4 weeks for tenosynovitis and up to 6 weeks if osteomyelitis is present. In children, antibiotics, drainage, and splinting are continued longer than in adults in an attempt to salvage the hand and protect the growing physes.
Wound Care and Splinting
- Wounds are often left open to heal by secondary intention or loosely approximated to allow for continued drainage.
- The hand is initially immobilized in a bulky compressive dressing and a volar splint in the intrinsic-plus (safe) position: wrist extended 20-30 degrees, MCP joints flexed 70-90 degrees, and IP joints fully extended. This prevents collateral ligament contracture and subsequent stiffness.
Rehabilitation
- Early Active Motion: Once the acute infection is controlled (typically within 48 to 72 hours postoperatively) and irrigation catheters are removed, early active range of motion (ROM) is initiated under the guidance of a specialized hand therapist.
- Tendon gliding exercises are critical to prevent the formation of dense adhesions between the flexor tendons and the sheath, which is the most common complication of flexor tenosynovitis.
- Edema control through elevation, compressive wrapping (once wounds are stable), and retrograde massage is essential to restore normal hand biomechanics.
COMPLICATIONS AND SALVAGE PROCEDURES
Despite aggressive management, deep space infections of the hand carry a high risk of morbidity.
1. Tendon Rupture: Enzymatic degradation of the tendon and disruption of the vincula (the tendon's blood supply) can lead to spontaneous rupture. Salvage may require delayed tendon grafting or tendon transfer once the infection is completely eradicated.
2. Stiffness: Arthrofibrosis and tendon adhesions are nearly universal to some degree. Tenolysis or capsulotomy may be considered 6 to 12 months post-infection if functional deficits persist.
3. Osteomyelitis: Bone infection requires aggressive surgical debridement, prolonged intravenous antibiotics, and potential bone grafting or arthrodesis.
4. Systemic Sepsis: In immunocompromised or diabetic patients, localized hand infections can rapidly progress to systemic inflammatory response syndrome (SIRS) and sepsis, requiring intensive care management.
You Might Also Like