Operative Management of Felons and Deep Subfascial Hand Space Infections
Key Takeaway
A felon is a closed-space infection of the distal digital pulp, characterized by intense throbbing pain due to pressure within fibrous septal compartments. Prompt surgical incision and drainage are critical to prevent ischemic necrosis and osteomyelitis. This guide details the pathoanatomy, precise surgical approaches—including midline volar and high lateral incisions—and postoperative protocols for managing felons and deep subfascial space infections of the hand.
INTRODUCTION TO DIGITAL AND HAND INFECTIONS
Infections of the hand and digits represent a critical category of orthopedic emergencies. The unique, highly compartmentalized anatomy of the hand dictates the pathophysiology, spread, and surgical management of these infections. Among the most common and potentially devastating localized infections is the felon—an abscess of the distal digital pulp. Furthermore, when infections breach superficial barriers or track along synovial sheaths, they may seed the deep subfascial spaces of the hand. A profound understanding of hand anatomy, precise surgical technique, and aggressive postoperative rehabilitation are mandatory to prevent catastrophic outcomes, including tissue necrosis, osteomyelitis, and permanent loss of hand function.
FELON: DISTAL PULP SPACE INFECTION
A felon is defined as a purulent abscess located within the subcutaneous tissues of the distal pulp of a finger or thumb. Due to the unique microanatomy of the fingertip, even minor accumulations of purulence can lead to disproportionately severe pain and rapid tissue ischemia.
Pathoanatomy and Biomechanics of the Distal Pulp
The distal digital pulp is not a single, homogenous subcutaneous space. It is meticulously divided into 15 to 20 tiny, discrete compartments by strong, inelastic fibrous septa. These septa traverse vertically from the volar skin to the periosteum of the distal phalanx.
Additionally, a dense transverse fibrous curtain is present at the level of the distal flexor finger crease. This curtain acts as a proximal barrier, effectively sealing the distal pulp space from the more proximal flexor tendon sheath. While this barrier is protective against the proximal spread of infection (preventing a primary felon from easily becoming a suppurative flexor tenosynovitis), it creates a rigid, closed-compartment system distally.
Because of these inelastic septa, any inflammatory swelling or purulent accumulation causes an immediate, exponential rise in compartmental pressure. This elevated pressure manifests clinically as intense, throbbing pain. More critically, the increased pressure rapidly exceeds capillary perfusion pressure, leading to microvascular compromise.
CLINICAL PEARL: The diaphysis of the distal phalanx derives its primary blood supply from terminal branches of the digital arteries that traverse the closed pulp space. Conversely, the epiphysis receives its blood supply proximal to the pulp space. Therefore, untreated compartment syndrome of the pulp (a felon) frequently leads to ischemic necrosis and osteomyelitis of the phalangeal diaphysis, while the epiphysis and the distal interphalangeal (DIP) joint are typically spared.
Etiology and Microbiology
Infection is most commonly inoculated via a penetrating injury. Common vectors include:
* Splinters, thorns, or glass fragments.
* Iatrogenic "finger sticks" for medical diagnostics (e.g., capillary blood glucose or hematocrit determinations), making diabetic patients particularly susceptible.
* Minor abrasions or neglected paronychia that track volarly.
Staphylococcus aureus is the most frequently isolated organism, with Methicillin-resistant S. aureus (MRSA) becoming increasingly prevalent. In cases involving human bites or dental contact, Eikenella corrodens must be suspected. Animal bites (cats/dogs) frequently yield Pasteurella multocida. In immunocompromised or diabetic patients, polymicrobial infections, including Gram-negative bacilli and anaerobes, are common.
Clinical Presentation and Diagnosis
Patients typically present with a history of a minor puncture wound followed by the rapid onset of severe, throbbing pain in the fingertip. The pain is often exacerbated by dependency and prevents sleep.
* Inspection: The distal pulp is erythematous, tense, and bulbous. A visible punctum or area of pointing purulence may be present volarly.
* Palpation: Exquisite tenderness is localized to the pulp. The tension is palpable.
* Imaging: Plain radiographs (AP, lateral, and oblique of the digit) are mandatory to rule out retained radiopaque foreign bodies and to assess for early signs of osteomyelitis or distal phalangeal osteolysis.
Operative Technique: Incision and Drainage of a Felon
Surgical intervention is indicated when there is a fluctuant abscess, visible pointing, or severe throbbing pain with extreme tension that does not rapidly respond to initial antibiotic therapy. The goal of surgery is to evacuate purulence, decompress the pulp space by dividing the fibrous septa, and obtain cultures, all while avoiding iatrogenic injury to the digital nerves and tactile surfaces.
Preoperative Preparation
- Anesthesia: A digital block using 1% plain lidocaine or 0.5% bupivacaine is administered at the base of the digit. Epinephrine should generally be avoided in the setting of a tense, ischemic felon to prevent irreversible digital ischemia.
- Tourniquet: A sterile Penrose drain or a commercial digital tourniquet is applied at the base of the finger to provide a bloodless surgical field.
Technique 75-3: Step-by-Step Surgical Approaches
The choice of incision depends entirely on the location of the abscess and the area of maximal fluctuance or pointing.
1. Volar Midline Incision (For Volar-Pointing Abscesses)
* Indication: When the abscess is in the distal pulp area pointing directly volarward toward the whorl of the fingerprint.
* Execution: If the overlying skin is already necrotic, the abscess is drained by sharply excising the necrotic skin ellipse. If the skin is intact, a vertical (longitudinal) incision is made precisely in the midline of the volar pad.
* Boundaries: The incision must begin distal to the distal interphalangeal skin crease to avoid violating the flexor tendon sheath.
* Rationale: A precise midline incision avoids the lateral branches of the digital nerve, which arborize laterally. It allows for direct drainage and heals with a minimal, non-tender scar.
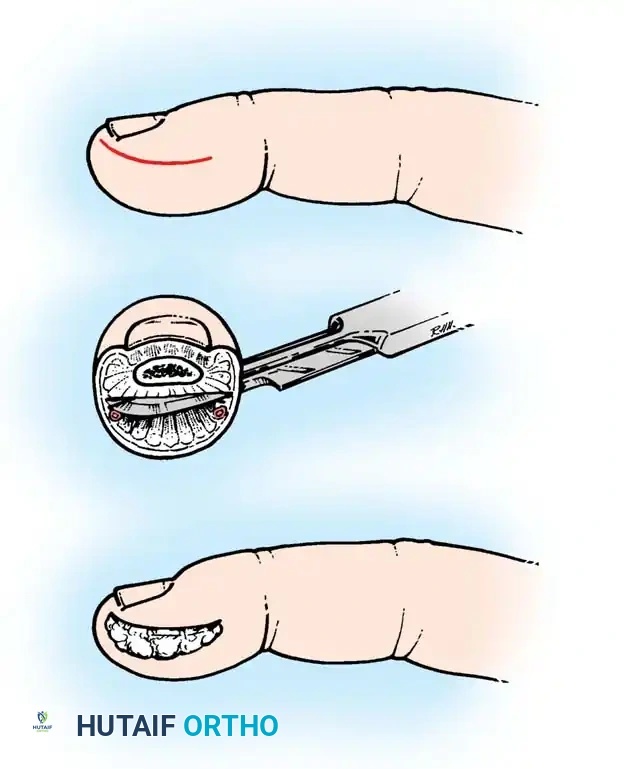
2. High Lateral or J-Shaped Incision (For Deep/Partitioned Abscesses)
* Indication: If the abscess is deep, involves multiple compartments, and is heavily partitioned by the septa without a clear volar pointing site.
* Execution: Make a longitudinal incision along the ulnar or radial aspect of the digit, usually away from the primary contact/pinch area of the finger (e.g., ulnar side of the index/middle fingers, radial side of the thumb/small fingers).
* Precision: This incision must be highly accurate. It must be placed dorsal to the tactile surface of the finger and not more than 3 mm from the distal free edge of the nail.
* Dissection: Once the skin is incised, use blunt dissection with the tip of small tenotomy scissors or a mosquito hemostat. Sweep the instrument across the pulp space to disrupt the fibrous septa and open all compartments. Avoid sharp dissection deep in the pulp to prevent severing nerve endings.
SURGICAL WARNING: If the lateral incision is placed too far volarly (palmar), the terminal branches of the digital nerve will be painfully transected, resulting in debilitating neuromas on the tactile surface.
PITFALL: Never utilize a "fish-mouth" incision (a continuous U-shaped incision around the entire fingertip). This approach is historically obsolete. It is notoriously slow to heal, devascularizes the volar pad, creates an unstable pulp, and results in severe, painful scarring. A simple lateral or J-shaped incision is entirely sufficient for adequate drainage.
Wound Management and Closure
- Following septal disruption and purulence evacuation, irrigate the wound copiously with sterile normal saline.
- Obtain deep tissue swabs or fluid aspirates for aerobic, anaerobic, and mycobacterial cultures.
- Leave the wound open. Pack the cavity loosely with a small wick of iodoform gauze or a sterile plain gauze strip to prevent premature skin closure and allow continuous drainage.
Postoperative Protocol and Rehabilitation
- Immediate Post-op: The finger is dressed with a bulky, non-restrictive dressing and splinted in a safe position (intrinsic plus) to protect the digit. Strict elevation above heart level is maintained to minimize edema.
- Wound Care: The initial packing and bandage are removed at approximately 48 hours postoperatively. Dressing changes are then initiated, often incorporating warm saline soaks (15-20 minutes, 2-3 times daily) to promote drainage and mechanical debridement. The wound is allowed to heal entirely by secondary intention.
- Rehabilitation: Active range-of-motion (ROM) exercises of all uninvolved joints and the affected digit (once pain permits) are emphasized early to prevent stiffness. Edema control and gradual reincorporation of the finger into activities of daily living are critical.
- Antimicrobial Therapy: Empirical antibiotic treatment with first-generation cephalosporins (e.g., cephalexin) is usually sufficient for community-acquired infections. However, therapy must be tailored based on the results of culture and sensitivity studies.
- Special Populations: Infections in patients with diabetes mellitus, peripheral vascular disease, or systemic immunosuppression can be exceptionally difficult to control. In these cohorts, progressive tissue necrosis or recalcitrant osteomyelitis may ultimately necessitate terminal amputation.
DEEP SUBFASCIAL SPACE INFECTIONS OF THE HAND
While superficial infections like felons and paronychia are common, infections of the potential spaces in the subfascial and deeper layers of the hand are infrequent but limb-threatening. These spaces are normally collapsed, containing only loose areolar tissue, but can rapidly expand to accommodate massive amounts of purulence. A high index of clinical suspicion is required for their early detection and surgical treatment.
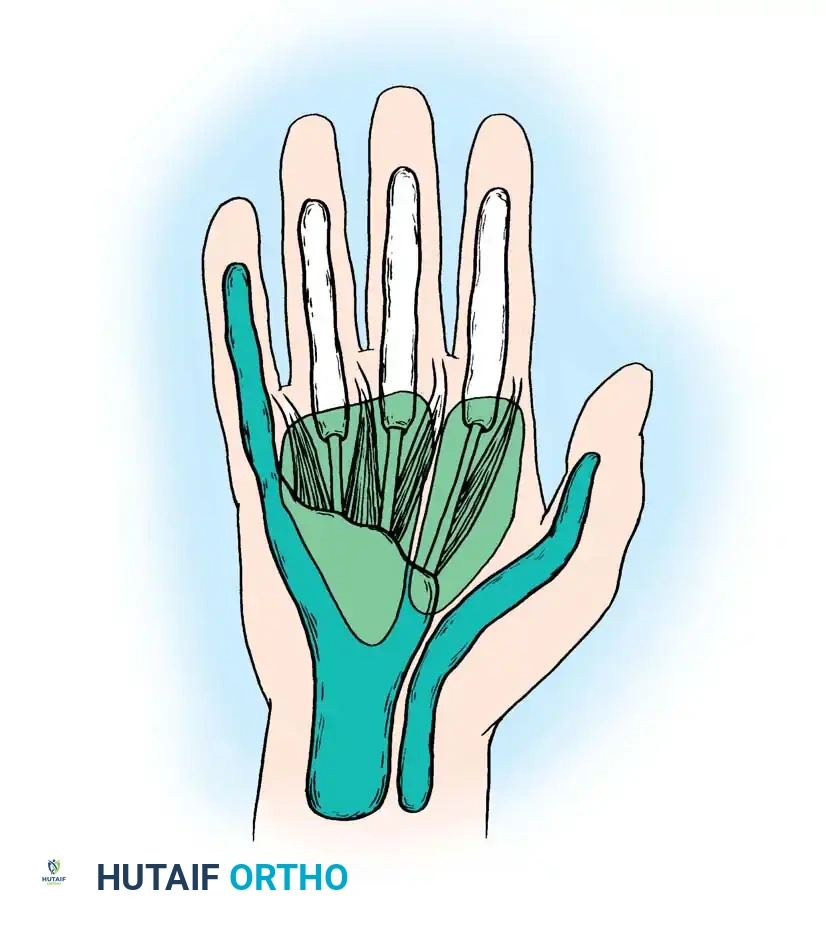
Applied Anatomy of the Deep Hand Spaces
The recognized deep spaces of the hand include:
- Interdigital Web Spaces: Located between the bases of the proximal phalanges. They contain the lumbrical muscles, neurovascular bundles, and loose connective tissue.
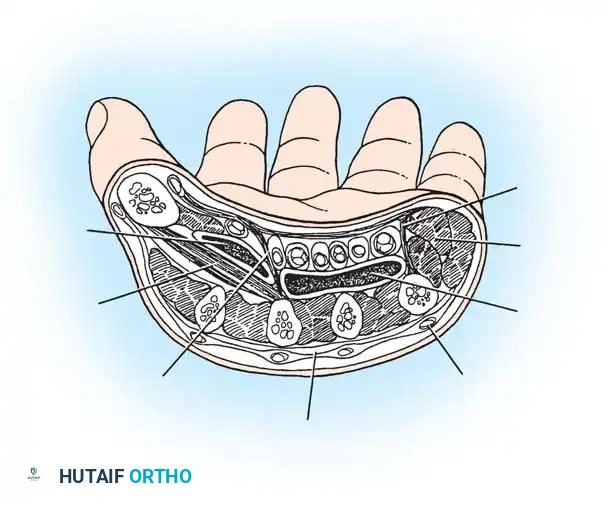
- Midpalmar Space: Deep to the flexor tendons and superficial to the fascia covering the interosseous muscles and the third, fourth, and fifth metacarpals. It is bounded radially by the midpalmar (oblique) septum, which attaches to the third metacarpal.
- Thenar Space: Located radial to the midpalmar septum. It lies deep to the flexor tendons of the index finger and the first lumbrical, and superficial to the adductor pollicis muscle.
- Hypothenar Space: A less well-defined space enveloping the hypothenar musculature, bounded by the hypothenar septum.
- Parona Space (Deep Forearm Space): Located in the distal volar forearm, deep to the flexor digitorum profundus tendons and superficial to the pronator quadratus. It communicates distally with the midpalmar space and the radial/ulnar bursae.
- Dorsal Subaponeurotic Space: Located on the dorsum of the hand, deep to the extensor tendons and superficial to the dorsal interosseous fascia.
Pathogenesis and Clinical Evaluation
Deep space infections typically arise from penetrating trauma, neglected superficial infections, or rupture of a purulent flexor tenosynovitis.
- Thenar Space Abscess: Presents with massive swelling of the thenar eminence and the thumb web space. The thumb is forced into abduction and extension. Flexion is exquisitely painful.
- Midpalmar Space Abscess: Presents with loss of the normal palmar concavity. The palm appears bulging and tense. The middle and ring fingers are often held in partial flexion, and passive extension causes severe pain.
- Web Space Infection (Collar Button Abscess): Often begins as a palmar blister or callus infection that tracks deep, bifurcating the transverse metacarpal ligament to present both volarly and dorsally (hourglass or collar-button shape). The adjacent fingers are abducted away from each other.
Operative Technique: Drainage of Deep Hand Spaces
Surgical drainage of deep spaces requires general anesthesia or regional block (axillary/supraclavicular), a proximal arm tourniquet, and meticulous dissection to avoid the dense network of palmar neurovascular structures.
Technique 75-4: Incision and Drainage
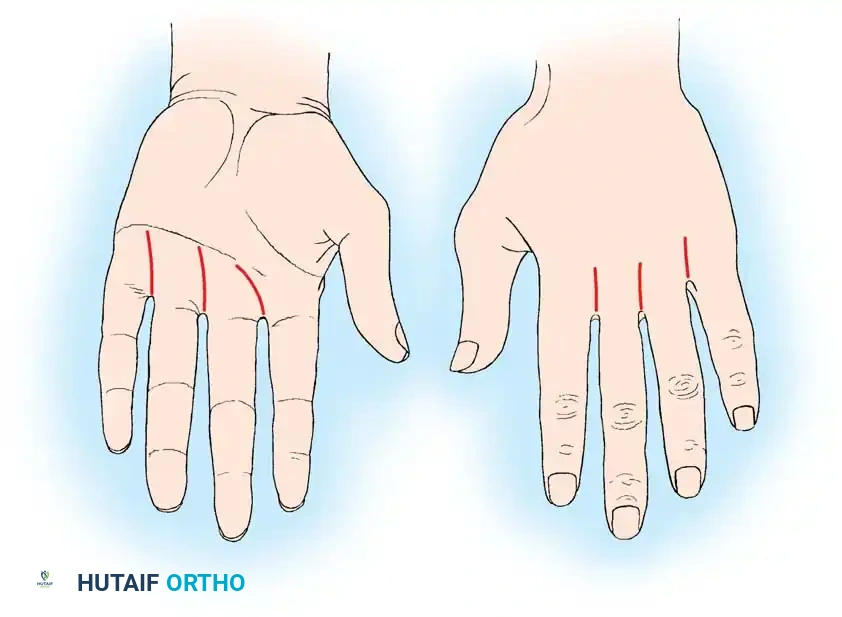
1. Web Space Abscess Drainage
* Approach: A combined approach is often necessary due to the "collar button" nature of the abscess.
* Palmar Incision: Make a longitudinal or slightly curved incision over the volar aspect of the affected web space, avoiding crossing the flexion creases at a right angle.
* Dorsal Incision: A longitudinal incision is made over the dorsal aspect of the web space, between the metacarpal heads.
* Dissection: Carefully dissect through the subcutaneous tissue. Protect the digital neurovascular bundles, which lie volar to the transverse metacarpal ligament. Establish communication between the dorsal and volar incisions to ensure complete evacuation of the hourglass abscess.
2. Midpalmar Space Drainage
* Approach: Drain the middle palmar space through a curved incision beginning at the level of the distal palmar crease. The incision should be in line with the axis of the long finger and extend ulnarward, terminating just inside the hypothenar eminence.
* Alternative Incisions: Other viable options include a longitudinal distal palm incision (placed between the rays to avoid the neurovascular bundles) or a transverse palm incision within the skin creases.
* Dissection: Incise the palmar fascia. Identify the neurovascular bundles and retract them safely. Enter the midpalmar space on either side of the long flexor tendon of the ring finger.
* Evacuation: Use a blunt instrument, such as a closed hemostat, to gently spread and enter the space. This blunt entry is critical to avoid iatrogenic injury to the deep palmar arch or the digital nerves.
* Drainage: Irrigate copiously. Leave a Penrose drain or a small silicone drain in place if the cavity is large or heavily loculated.
3. Thenar Space Drainage
* Approach: Can be drained via a dorsal or volar approach. A dorsal longitudinal incision over the first web space, parallel to the border of the first dorsal interosseous muscle, is highly effective and avoids palmar scarring.
* Dissection: Dissect bluntly volar to the adductor pollicis muscle to enter the thenar space. Avoid injury to the radial artery as it passes between the two heads of the first dorsal interosseous muscle.
Postoperative Management of Deep Space Infections
- Wound Care: Wounds are left open. Drains, if placed, are typically removed at 48 to 72 hours once output becomes serous and minimal. Wet-to-dry dressings or continuous irrigation systems may be utilized in severe cases.
- Immobilization: The hand is placed in a bulky compressive dressing and a volar splint. The wrist is extended to 20-30 degrees, metacarpophalangeal (MCP) joints flexed to 70-90 degrees, and interphalangeal (IP) joints fully extended (the intrinsic-plus or "safe" position) to prevent collateral ligament contracture.
- Elevation: Continuous strict elevation is mandatory to reduce profound hand edema, which can otherwise lead to intrinsic muscle fibrosis and a stiff, non-functional hand.
- Therapy: Aggressive hand therapy is initiated as soon as the acute inflammatory phase subsides. Active and passive ROM exercises are critical to prevent tendon adhesions and joint stiffness.
- Antimicrobials: Intravenous antibiotics are initiated empirically and transitioned to culture-directed oral therapy. The duration of treatment depends on the clinical response, extent of tissue necrosis, and presence of concurrent osteomyelitis.
You Might Also Like