Eponychial Marsupialization and Advanced Surgical Management of Paronychia
Key Takeaway
Eponychial marsupialization is a highly effective surgical intervention for recalcitrant chronic paronychia. By excising a crescentic wedge of proximal eponychial skin, the technique facilitates drainage, eradicates fibrotic tissue, and restores the physiological barrier of the nail fold. When combined with targeted antibiotic therapy and meticulous postoperative care, this procedure yields excellent clinical outcomes with minimal recurrence rates.
Introduction to Perionychial Infections
Infections of the fingertip and perionychium represent some of the most common pathologies encountered in hand surgery. While acute paronychia is typically a straightforward bacterial infection amenable to simple drainage and antibiotics, chronic paronychia presents a more complex therapeutic challenge. It is characterized by persistent inflammation, fibrosis, and the loss of the protective cuticle barrier, often driven by a combination of mechanical irritation, fungal colonization (predominantly Candida albicans), and mixed bacterial flora.
When conservative measures—such as avoidance of moisture, topical corticosteroids, and antifungal agents—fail, surgical intervention becomes mandatory. Eponychial marsupialization, originally described by Keyser and Eaton and later modified by Bednar and Lane, remains the gold standard for recalcitrant chronic paronychia. More recently, alternative tissue-sparing approaches, such as the "Swiss roll" technique described by Pabari et al., have expanded the armamentarium of the orthopedic hand surgeon.
This comprehensive guide details the surgical anatomy, biomechanics, and step-by-step operative execution of these advanced techniques, alongside the management of concurrent deep space infections such as pulp abscesses (felons).
Surgical Anatomy and Pathomechanics
A profound understanding of fingertip anatomy is prerequisite for executing perionychial surgery without causing iatrogenic nail dystrophy.
The Perionychium
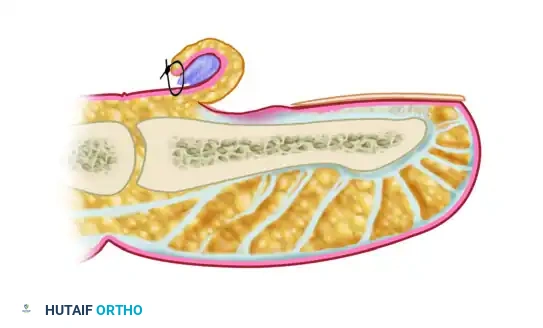
The perionychium comprises the nail bed and the surrounding soft tissues (paronychium). The nail bed is divided into the germinal matrix (proximal, responsible for 90% of nail plate generation) and the sterile matrix (distal, responsible for nail adherence and thickness). The eponychium is the proximal nail fold, and its distal extension forms the cuticle, which creates a vital waterproof seal between the skin and the nail plate.
In chronic paronychia, this cuticular seal is destroyed. The resulting dead space allows debris, moisture, and pathogens to accumulate beneath the eponychial fold, leading to chronic induration, fibrosis, and hypertrophy of the proximal nail fold.
The Digital Pulp and Fibrous Septa
The volar aspect of the distal phalanx is uniquely structured to withstand compressive forces during pinch and grasp. The subcutaneous tissue of the distal pulp is partitioned into tiny, semi-rigid compartments by strong fibrous septa that traverse vertically from the dermis to the periosteum of the distal phalanx. A transverse fibrous curtain is also present at the distal flexor finger crease, effectively isolating the distal pulp from the proximal digital spaces.
Clinical Pearl: Because of these unyielding fibrous septa, any inflammatory swelling or purulence within the pulp causes an immediate, exponential rise in compartmental pressure. This localized compartment syndrome results in severe, throbbing pain that is the hallmark of a felon.
Infection in this space is typically inoculated via a penetrating injury, such as a splinter, thorn, or iatrogenic "finger sticks" for medical reasons (e.g., hematocrit and blood glucose determinations). Staphylococcus aureus is the organism most commonly isolated from these fingertip infections.
If left untreated, the pressure necrosis and enzymatic degradation within a pulp abscess (felon) can extend along multiple pathways:
1. Deeply into the periosteum, causing osteomyelitis of the distal phalanx.
2. Dorsally around the nail bed, causing a subungual abscess or secondary paronychia.
3. Proximally through the transverse fibrous curtain into the flexor tendon sheath, resulting in purulent flexor tenosynovitis.
4. Superficially through the skin, leading to spontaneous rupture and skin necrosis.
Eponychial Marsupialization
The principle of eponychial marsupialization is to excise the diseased, fibrotic tissue of the proximal nail fold, thereby decompressing the infected space, promoting aerobic conditions, and allowing the wound to heal by secondary intention. This process regenerates a healthy, tight cuticular seal.
Indications
- Chronic paronychia refractory to 6–8 weeks of conservative management.
- Hypertrophic, indurated eponychial fold with recurrent acute exacerbations.
- Presence of severe nail plate irregularities secondary to chronic matrix inflammation.
Preoperative Preparation
- Positioning: The patient is positioned supine with the affected hand extended on a radiolucent hand table.
- Anesthesia: A standard digital block is administered using 1% lidocaine and 0.5% bupivacaine. Ensure profound anesthesia before proceeding, as the perionychium is highly innervated.
- Preparation: The hand is prepped with a standard antiseptic solution (chlorhexidine or povidone-iodine) and draped appropriately. A sterile digital tourniquet (e.g., a Penrose drain or rolled glove finger) is applied to the base of the digit to ensure a bloodless surgical field.
Surgical Technique: Step-by-Step
Step 1: Incision and Excision
Using a #15 or #11 scalpel blade, carefully map out a crescent-shaped wedge of skin over the proximal nail fold. The excision should be approximately 3 mm wide at its apex, running parallel to the eponychium, and extending from the radial to the ulnar borders of the nail fold.

Step 2: Depth of Dissection
The depth of the excision is a critical point of technical divergence in the literature:
* The Keyser and Eaton Technique: Advocates for the aggressive removal of all thickened, fibrotic tissue from the skin down to the level of the proximal nail plate, ensuring complete eradication of the diseased bursa.
* The Bednar and Lane Modification: Recommends a more conservative approach, excising the skin but leaving the underlying subcutaneous fat intact. Bednar and Lane found this modification equally effective in curing patients of chronic paronychia while potentially reducing the risk of iatrogenic injury to the underlying germinal matrix.
Surgical Warning: Extreme caution must be exercised to avoid penetrating the germinal matrix, which lies immediately deep to the proximal nail fold. Damage to the germinal matrix will result in permanent, irreversible nail dystrophy.
Step 3: Management of the Nail Plate
Evaluate the nail plate. If significant nail irregularities, ridging, or subungual debris are present, the nail plate must be removed. Bednar and Lane noted that in the presence of nail dystrophy, removing the nail leads to optimal healing without recurrence, as it removes the colonized substrate and allows the matrix to regenerate a new, healthy plate.
Step 4: Dressing and Marsupialization
The wound is not closed. Instead, it is allowed to heal by secondary intention (marsupialization). Cover the excised crescentic defect with a non-adherent, antimicrobial dressing, such as petroleum/bismuth tribromophenate–impregnated gauze (Xeroform).
* Crucial Step: If the nail plate was removed, a strip of this Xeroform gauze must be carefully tucked beneath the proximal nail fold to prevent synechiae (adhesions) between the eponychium and the germinal matrix during the early healing phase.
The "Swiss Roll" Technique
Described by Pabari, Iyer, and Khoo, the "Swiss roll" technique offers an innovative alternative for the treatment of both acute and chronic paronychia.
Rationale and Advantages
The primary cited advantages of the Swiss roll technique include:
* Retention of the nail plate: Avoids the morbidity and prolonged recovery associated with total nail avulsion.
* Avoidance of a skin defect: Unlike marsupialization, no tissue is excised, preventing a permanent contour defect of the finger.
* Rapid healing: By preserving tissue and utilizing a tension-free retraction method, the local microenvironment normalizes rapidly.
Surgical Technique: Step-by-Step
Step 1: Exposure and Irrigation
Following digital block and tourniquet application, the eponychial fold is carefully elevated off the underlying nail plate using a periosteal elevator or a flat McDonald dissector. This exposes the inflamed germinal matrix and the infected sub-eponychial space. The area is thoroughly irrigated with sterile saline to remove purulence and debris.

Step 2: The "Swiss Roll" Retraction
A small roll of nonadherent dressing (such as Mepitel or a tightly rolled piece of Xeroform) is prepared. The elevated proximal nail fold is then reflected proximally over this nonadherent dressing, effectively rolling the skin back like a "Swiss roll."
Step 3: Securing the Fold
The rolled eponychial fold is secured to the dorsal skin of the distal phalanx using a nonabsorbable suture (e.g., 4-0 or 5-0 Prolene). The suture passes through the proximal skin, over the rolled fold, and anchors it in a retracted position. This keeps the sub-eponychial space open for continuous drainage and aeration without excising any tissue.
The suture and dressing are typically removed in the clinic after 7 to 10 days, once the acute inflammation has subsided and the space has sterilized.
Management of Concurrent Pulp Abscess (Felon)
Because chronic paronychia can occasionally be complicated by, or misdiagnosed as, a deep space infection of the distal pulp, the surgeon must be prepared to manage a felon.
The diagnosis of a pulp abscess is primarily clinical. While early cellulitis presents with swelling and redness, the presence of an abscess is highly likely if severe, throbbing pain has persisted for 12 hours or longer, accompanied by tense, fluctuant swelling of the volar pad.
Surgical Drainage of a Felon
Treatment consists of prompt surgical incision and drainage combined with systemic antibiotics.
1. Incision Placement: The incision must divide the fibrous septa to adequately decompress the pulp. A high lateral (mid-axial) incision is generally preferred as it avoids the tactile volar pad and prevents painful scarring.
2. Decompression: A hemostat is bluntly spread through the fibrous septa across the pulp space. Care must be taken not to violate the distal flexor crease (to avoid flexor tenosynovitis) or the tendon sheath itself.
3. Wound Care: The wound is loosely packed with a small wick or allowed to drain freely, followed by warm soaks and healing by secondary intention.
Postoperative Protocol and Rehabilitation
Meticulous postoperative care is arguably as critical as the surgical execution in preventing recurrence of chronic paronychia.
Antimicrobial Therapy
- Empiric Coverage: Therapy with an oral antibiotic targeting Staphylococcus aureus and common skin flora (such as cephalexin or erythromycin) is initiated immediately postoperatively.
- Duration: Antibiotics should generally be continued for a full 2 weeks to ensure eradication of deep-seated micro-abscesses.
- Culture-Directed Adjustments: Intraoperative swabs should always be sent for aerobic, anaerobic, and fungal cultures. If the culture results return negative, or if the pathology is proven to be purely inflammatory/fungal, antibacterial antibiotics can be safely discontinued in 3 to 5 days. If Candida is isolated, oral fluconazole may be indicated.
Local Wound Care
- Initial Dressing: The bulky surgical dressing is left intact for the first 48 to 72 hours.
- Daily Regimen: Beginning on postoperative day 3, the patient is instructed to remove the dressings and begin a rigorous soaking regimen. The affected finger should be soaked in a dilute solution of hydrogen peroxide and washed with a chlorhexidine gluconate skin cleanser (Hibiclens) three times daily.
- Progression: These daily washings are continued meticulously until all purulent or serous drainage ceases and the wound bed demonstrates healthy granulation tissue.
Pitfall: Premature cessation of daily soaks allows crusting and premature closure of the marsupialized edge, recreating the closed dead space and leading to immediate recurrence of the paronychia.
Complications and Outcomes
When performed correctly, eponychial marsupialization and the Swiss roll technique yield excellent outcomes with high patient satisfaction. However, potential complications include:
- Nail Dystrophy: The most feared complication, resulting from iatrogenic injury to the germinal matrix during excision or overly aggressive debridement.
- Recurrence: Usually secondary to inadequate excision of the fibrotic bursa, failure to remove a colonized/dystrophic nail plate, or poor patient compliance with the postoperative soaking regimen.
- Osteomyelitis: A risk if a concurrent deep space infection (felon) was missed or inadequately decompressed, allowing the infection to penetrate the periosteum of the distal phalanx.
By adhering strictly to the anatomical boundaries, selecting the appropriate surgical technique based on the presence of nail dystrophy, and enforcing a strict postoperative hygiene protocol, the orthopedic surgeon can reliably eradicate chronic perionychial infections and restore both the function and aesthetics of the digit.
📚 Medical References
You Might Also Like
