Deep Fascial Space Infections of the Hand: Operative Guide
Key Takeaway
Deep fascial space infections of the hand, including thenar, midpalmar, and hypothenar abscesses, are severe conditions requiring prompt surgical intervention. Often arising from neglected flexor tenosynovitis, these infections present with profound swelling and restricted digit mobility. This guide details the complex surgical anatomy, precise diagnostic criteria, and step-by-step operative techniques for effective drainage and eradication of deep palmar space infections.
INTRODUCTION TO DEEP FASCIAL SPACE INFECTIONS
Deep fascial space infections of the hand represent a critical orthopedic emergency. Historically, before the advent of broad-spectrum antibiotics, these infections frequently resulted in devastating morbidity, including ischemic necrosis, profound stiffness, and amputation. Today, primary infections within these deep anatomical compartments are relatively rare; less extensive superficial infections or localized abscesses are typically controlled by antimicrobial therapy before contiguous spread occurs.
When deep fascial space infections do arise, they are almost exclusively secondary to the proximal spread of infection from other regions of the hand. The most common etiology is neglected or fulminant purulent flexor tenosynovitis, penetrating trauma, or the rupture of a localized abscess into the deep palmar compartments. Prompt recognition, an intimate understanding of the complex fascial anatomy, and aggressive surgical decompression remain the cornerstones of limb-salvaging treatment.
SURGICAL ANATOMY AND BIOMECHANICS
The hand is compartmentalized by a complex network of fascial septa that dictate the potential pathways for the spread of purulence. Understanding these boundaries is paramount for accurate diagnosis and safe surgical drainage. The deep palmar fascial space lies strategically between the deep fascia covering the metacarpals and their contiguous interosseous muscles, and the superficial fascia dorsal to the flexor tendons.
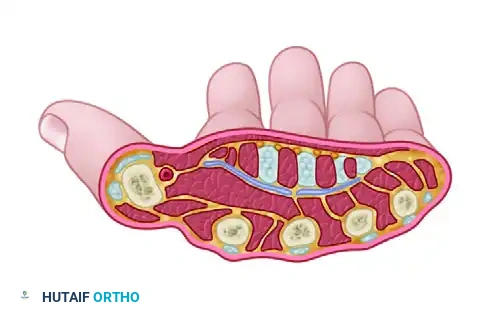
Cross-sectional anatomy demonstrating the relationships of the deep palmar spaces when not distended by pus.
The Oblique Fascial Septum
The central palmar space is not a single void but is divided into two distinct compartments—the middle palmar space and the thenar space—by a critical anatomical structure: the oblique fascial septum. This fibrous membrane passes obliquely from the shaft of the third metacarpal to the fascia dorsal to the flexor tendons of the index finger. This septum acts as a barrier, though virulent infections can occasionally breach it.
The Middle Palmar Space
- Radial Border: The oblique fascial septum.
- Ulnar Border: The fascia of the hypothenar muscles.
- Dorsal Floor: The fascia covering the third, fourth, and fifth metacarpals and the volar interosseous muscles.
- Volar Roof: The fascia dorsal to the flexor tendons of the middle, ring, and small fingers, along with the digital neurovascular bundles and lumbrical muscles.
The Thenar Space
- Radial Border: The fascia of the adductor pollicis and other thenar muscles.
- Ulnar Border: The oblique fascial septum.
- Dorsal Floor: The transverse head of the adductor pollicis muscle.
- Volar Roof: The flexor tendons of the index finger and the first lumbrical muscle.
The Hypothenar Space
The hypothenar space is a distinct, tightly enclosed compartment that rarely communicates with the central palmar spaces.
* Lateral Border: The hypothenar septum.
* Dorsal Border: The fifth metacarpal.
* Medial and Palmar Borders: The hypothenar muscle fascia.
The Space of Parona
Located in the distal forearm, the space of Parona is a potential space that can serve as a reservoir for massive purulent accumulation, particularly in cases of "horseshoe abscesses" where infection spreads via communicating radial and ulnar bursae.
* Dorsal Border: The pronator quadratus muscle.
* Lateral Border: The flexor pollicis longus (FPL).
* Medial Border: The flexor carpi ulnaris (FCU).
* Palmar Border: The deep surface of the flexor digitorum profundus (FDP) tendons.
CLINICAL PEARL: Abscess formation primarily originating in the space of Parona is exceedingly rare. When purulence is found here, the surgeon must meticulously evaluate the radial and ulnar bursae and the digital flexor sheaths of the thumb and small finger for the primary source of infection.
CLINICAL PRESENTATION AND DIAGNOSIS
The clinical presentation of deep fascial space infections is characterized by severe systemic toxicity, profound local pain, and distinct anatomical deformities based on the specific space involved. Because the palmar skin is thick and tightly bound by fascial septa, the massive edema associated with these infections often presents dorsally, driven by the rich dorsal lymphatic drainage network.
Middle Palmar Space Abscess
A middle palmar abscess generates a severe systemic inflammatory response. Patients present with exquisite local pain and tenderness localized to the central palm.
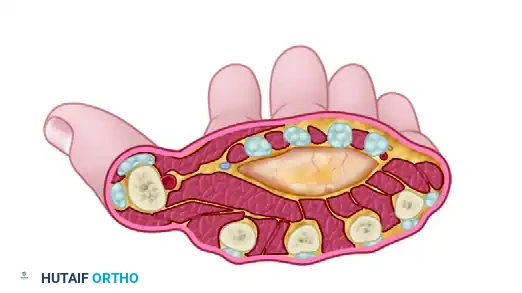
Cross-sectional representation of an abscess distending the middle palmar space.
Key Clinical Signs:
* Loss of Active Motion: The patient exhibits an inability to actively move the long and ring fingers due to severe pain and mechanical distension of the space surrounding the flexor tendons and lumbricals.
* The "Rubber Glove" Sign: The hand and fingers undergo generalized, massive swelling. The loss of the normal palmar concavity combined with profound dorsal edema gives the hand the appearance of an inflated rubber glove.
* Tenderness: Maximal point tenderness is elicited over the central palm, distal to the transverse carpal ligament and proximal to the metacarpophalangeal (MCP) joints.
Thenar Space Abscess
A thenar space abscess presents with symptoms similar in systemic severity to a midpalmar infection but with a distinctly different anatomical deformity.
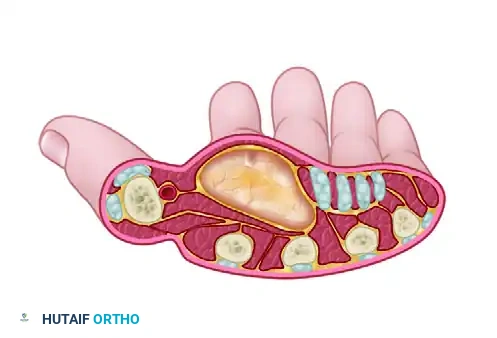
Cross-sectional representation of an abscess distending the thenar space, displacing the adductor pollicis.
Key Clinical Signs:
* Thumb Web Ballooning: The first web space becomes massively swollen and indurated, forcing the thumb into a position of abduction and extension.
* Index Finger Flexion: The index finger is characteristically held in a flexed posture to relieve tension on the distended thenar space roof.
* Impaired Motion: Active motion of both the index finger and the thumb is severely impaired due to pain and mechanical block.
SURGICAL WARNING: Do not mistake the profound dorsal edema associated with deep palmar space infections for a primary dorsal subcutaneous abscess. Incising the dorsum of the hand for a palmar infection will fail to drain the primary abscess and may introduce iatrogenic complications.
INDICATIONS FOR SURGERY
Surgical intervention is the definitive treatment for deep fascial space infections.
Absolute Indications:
* Clinical evidence of a fluctuant abscess within the thenar, midpalmar, or hypothenar spaces.
* Progression of symptoms (pain, swelling, erythema) despite 24 hours of appropriate intravenous antibiotic therapy.
* Concomitant purulent flexor tenosynovitis with suspected rupture into the deep spaces.
* Signs of systemic sepsis or impending compartment syndrome of the hand.
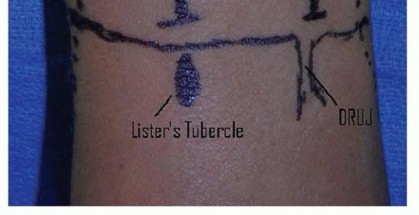
PREOPERATIVE PREPARATION AND POSITIONING
- Anesthesia: General anesthesia or a regional brachial plexus block is mandatory. Local infiltration is contraindicated due to the risk of spreading the infection and the inability to achieve adequate anesthesia in an acidic, infected environment.
- Tourniquet: A well-padded pneumatic arm tourniquet is essential for a bloodless surgical field. Exsanguination should be performed via arm elevation rather than an Esmarch bandage to prevent proximal milking of purulent material.
- Positioning: The patient is positioned supine with the affected arm extended on a radiolucent hand table.
- Antibiotics: Broad-spectrum intravenous antibiotics (covering MRSA, Streptococcus, and Gram-negative/anaerobic organisms if a bite or specific exposure is suspected) should be administered, ideally after intraoperative cultures are obtained, unless the patient is septic.
SURGICAL APPROACHES AND OPERATIVE TECHNIQUE
The goal of surgery is complete evacuation of purulence, thorough irrigation, and the establishment of dependent drainage while meticulously protecting neurovascular structures.
Drainage of the Middle Palmar Space
- Incision: Make a transverse or slightly oblique incision parallel to the distal palmar crease, directly over the area of maximal fluctuance. Alternatively, a longitudinal incision over the third or fourth metacarpal shaft can be utilized, ensuring it does not cross the flexion creases at a right angle.
- Dissection: Incise the skin and subcutaneous tissue. Identify and protect the digital neurovascular bundles, which lie superficial to the lumbrical muscles.
- Entering the Space: Longitudinally incise the deep palmar fascia. Retract the flexor tendons of the long and ring fingers laterally.
- Evacuation: Use a blunt hemostat to gently spread the tissues and enter the middle palmar space. A rush of purulent fluid will confirm entry.
- Irrigation: Obtain deep tissue and fluid cultures. Copiously irrigate the space with normal saline. Break up any loculations with blunt dissection.
Drainage of the Thenar Space
The thenar space can be approached via a palmar or a dorsal incision. The dorsal approach is often preferred as it avoids a painful palmar scar and reduces the risk of injury to the recurrent motor branch of the median nerve.
The Dorsal Approach

Lines demonstrating the dorsal incision for accessing the thenar space and web abscesses.
- Incision: Make a longitudinal incision on the dorsum of the first web space, running parallel to the radial border of the second metacarpal.
- Dissection: Deepen the incision through the subcutaneous tissue. Identify and protect the branches of the superficial radial nerve and the first dorsal interosseous muscle.
- Entering the Space: Bluntly dissect volar to the adductor pollicis muscle to enter the thenar space.
- Evacuation: Allow the purulence to drain, obtain cultures, and irrigate copiously.
The Palmar Approach

Lines demonstrating palmar incisions for web abscess drainage and volar access to the thenar space.
- Incision: Make a curved incision parallel to, but slightly radial to, the thenar crease.
- Dissection: Deepen the incision carefully.
- Nerve Protection: Crucial Step. Meticulously identify and protect the recurrent motor branch of the median nerve, which typically enters the thenar musculature at the proximal extent of this field.
- Entering the Space: Dissect bluntly between the adductor pollicis and the flexor tendons of the index finger to enter the abscess cavity.
PITFALL: Aggressive sharp dissection in the palmar thenar approach can easily sever the recurrent motor branch of the median nerve, leading to devastating loss of thumb opposition. Always use blunt spreading with a hemostat once the deep fascia is breached.
Drainage of Web Space Infections (Collar-Button Abscesses)
Web space infections often communicate between the palmar and dorsal aspects of the hand, forming a "collar-button" or hourglass-shaped abscess.
1. Palmar Incision: Utilize a zigzag or Brunner-type incision over the volar web space to avoid a scar contracture.
2. Dorsal Incision: Make a longitudinal incision over the dorsal web space between the metacarpal heads.
3. Communication: Pass a blunt instrument between the palmar and dorsal incisions, superficial to the deep transverse metacarpal ligament, to ensure both compartments of the abscess are fully communicating and drained.
Drainage of the Space of Parona
If infection has tracked proximally into the forearm:
1. Incision: Make a longitudinal incision on the volar-ulnar aspect of the distal forearm, just radial to the flexor carpi ulnaris (FCU).
2. Dissection: Retract the FCU and the ulnar neurovascular bundle medially. Retract the flexor digitorum profundus (FDP) tendons radially.
3. Evacuation: The space of Parona lies directly on the pronator quadratus. Evacuate the purulence, culture, and irrigate. Ensure communication with the carpal tunnel is clear if the infection originated from a flexor tenosynovitis.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management of deep fascial space infections is as critical as the surgical decompression itself.
Wound Management
- Drainage: Wounds are typically left open to heal by secondary intention, or loosely approximated over a Penrose drain or a continuous irrigation catheter.
- Dressing: Apply a bulky, non-compressive dressing.
- Splinting: The hand must be immobilized in the "safe position" (James position) to prevent contractures: wrist in 20-30 degrees of extension, MCP joints in 70-90 degrees of flexion, and interphalangeal (IP) joints in full extension. The thumb should be palmar abducted.
Medical Management
- Antibiotics: Intravenous antibiotics are continued postoperatively and tailored based on final intraoperative culture and sensitivity results. Transition to oral antibiotics is considered once clinical signs of infection (erythema, swelling, systemic symptoms) have significantly resolved.
- Elevation: Strict elevation of the affected extremity above the level of the heart is mandatory to reduce edema.
Rehabilitation
- Early Motion: Once the acute inflammatory phase subsides (typically 48 to 72 hours postoperatively), the splint is removed for supervised active and active-assisted range of motion (ROM) exercises.
- Hand Therapy: Formal occupational/hand therapy is essential to prevent tendon adhesions, joint stiffness, and complex regional pain syndrome (CRPS). Tendon gliding exercises and intrinsic muscle stretching are prioritized.
COMPLICATIONS
Failure to adequately diagnose and treat deep fascial space infections can lead to severe complications:
1. Stiffness and Contracture: The most common complication, resulting from prolonged edema, tendon adhesions, and capsular fibrosis.
2. Tendon Rupture or Necrosis: Prolonged purulent bathing of the flexor tendons can lead to ischemic necrosis and subsequent rupture.
3. Osteomyelitis or Septic Arthritis: Contiguous spread to the adjacent metacarpals or MCP joints.
4. Neurovascular Compromise: Digital ischemia or neuropathy secondary to compartment syndrome within the hand, or iatrogenic injury during surgical drainage.
By adhering to strict anatomical principles and executing timely, aggressive surgical decompression, the orthopedic surgeon can effectively eradicate deep fascial space infections and restore optimal hand function.
You Might Also Like