Ace FRCS Orthopaedics: Oxford University Press Adult Pathology Viva

Key Takeaway
Looking for accurate information on Ace FRCS Orthopaedics: Oxford University Press Adult Pathology Viva? Charcot arthropathy is a severe destructive joint disease occurring in patients with sensory disturbances, predominantly diabetic neuropathy (over 90% of UK cases). It involves rapid joint destruction, demineralization, and loss of normal foot architecture. Its pathophysiology combines neurotraumatic and neurovascular factors, leading to progressive deformity. This medical understanding is sourced from materials reproduced with permission from Oxford University Press.
A patient presents with this clinical photograph. Describe the pathology and the underlying principles of the management.
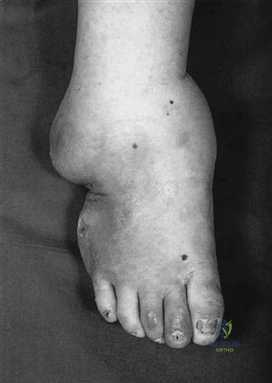
Candidate: This is a Charcot neuropathic arthropathy. It results from loss of protective sensation, most commonly due to diabetes. It involves bone destruction, fragmentation, and eventual collapse. Management includes early diagnosis, off-loading, and supportive bracing until consolidation occurs.
Candidates often forget to mention the differential diagnosis (e.g., osteomyelitis) or fail to describe the Eichenholz stages. They also frequently miss the critical nuance of avoiding rigid casts that can cause ulceration in insensate feet.
The candidate should structure the response: 1. Diagnosis: Charcot arthropathy (neurotraumatic/neurovascular etiology). 2. Pathophysiology: Loss of sensation leading to repetitive trauma and osteoclast overactivity. 3. Clinical Staging (Eichenholz): Collapse, Coalescence, Consolidation. 4. Management: High index of suspicion for early diagnosis; off-loading via total contact casting (monitoring skin integrity); and long-term protective orthotics after consolidation.
Describe the deformity shown here and outline the management based on the stage of the pathology.

Candidate: This is an adult-acquired flat foot deformity, likely due to Tibialis Posterior Tendon Dysfunction (TPTD). I would stage it using the Johnson & Strom classification and offer management accordingly, from orthotics in early stages to triple arthrodesis in fixed stages.
Failing to mention the "Too Many Toes" sign or neglecting the Achilles tendon (which must be assessed for contracture in stage 2 disease) are common omissions that signal a lack of clinical depth.
Structure by stages: Stage 1 (tenosynovitis): Conservative. Stage 2 (flexible deformity): Medial calcaneal sliding osteotomy + FDL transfer + possible Achilles lengthening. Stage 3 (fixed deformity): Subtalar or triple arthrodesis. Mentioning the Myerson Stage 4 (associated ankle valgus) demonstrates senior knowledge.
An elderly patient presents with hip pain and these radiographs. How would you classify this and what is your management strategy?

Candidate: This shows Avascular Necrosis (AVN) of the femoral head with subchondral collapse (crescent sign). This is Ficat/Arlet Stage 4. Management involves hip replacement.
Rushing to treatment without mentioning the underlying etiology (steroids, alcohol, trauma, sickle cell) or failing to acknowledge the "crescent sign" on the lateral view.
Classify using the Ficat/Arlet system (Stage 4). Discuss the multifactorial etiology (mnemonic: "PLASTIC RAGS"). Outline clear surgical decision-making: Core decompression for pre-collapse (Stage 1/2) vs. Total Hip Arthroplasty for collapse (Stage 3/4).
