Minimally Invasive THA: Navigating Techniques, Benefits & Pitfalls

Key Takeaway
This article provides essential research regarding Minimally Invasive THA: Navigating Techniques, Benefits & Pitfalls. Minimally invasive THA refers to less invasive surgical approaches for total hip arthroplasty, aiming for optimum visualization with reduced invasiveness. These techniques typically use smaller incisions, often 10-12 cm or less. Two main categories exist: modified single-incision and two-incision approaches. Proper patient selection is crucial due to potential challenges and ongoing studies regarding long-term outcomes.
Introduction and Epidemiology
Total hip arthroplasty (THA) has developed into one of the most frequently performed, highly successful, and cost-effective procedures in orthopedic surgery. Although there have been numerous variations in implant design, bearing surfaces, and biomaterials over the past several decades, surgical approaches to the hip remained relatively unchanged until the turn of the 21st century. Recently, paralleling the development of minimally invasive techniques within other surgical subspecialties, orthopedic surgeons have demonstrated increased interest in less invasive approaches for THA. The primary objective of these techniques is to balance the absolute necessity for optimum visualization and precise component placement with the desire to minimize soft tissue trauma.
The definition of "minimally invasive" in the context of THA remains a subject of academic debate. Historically, the "mini-incision" utilized for these techniques is typically defined by a skin incision length of 10 cm or less, with some authors expanding the definition to include incisions up to 12 cm (Vail, 2005). However, contemporary orthopedic consensus emphasizes that true minimally invasive surgery (MIS) is defined not merely by the length of the cutaneous incision, but by the preservation of the underlying musculotendinous structures. As with any complex arthroplasty, the incision length should never be rigidly standardized; several variables dictate the exposure required to safely and correctly perform the THA. The final length of the incision depends heavily on the skill and experience of the operating surgeon, patient body habitus, local subcutaneous tissue depth, muscle mass, and individual osseous anatomy.
Two primary categories of minimally invasive THA have materialized over the last two decades. The first category includes modified single-incision approaches, which are essentially variations of the standard posterior, anterolateral, and direct anterior approaches. The second category is the two-incision approach, which utilizes separate micro-incisions for acetabular and femoral preparation. While MIS THA has generated significant attention, it is critical to acknowledge that the primary goal of any THA is the accurate reconstruction of hip biomechanics without compromising soft tissues or neurovascular structures. Short-term outcomes of MIS THA have shown benefits in early postoperative pain and rehabilitation milestones, but long-term survivorship ultimately depends on precise component positioning and restoration of joint kinematics.
Surgical Anatomy and Biomechanics
A profound understanding of periacetabular and proximal femoral anatomy is the cornerstone of minimally invasive THA. Because visualization is inherently restricted compared to extensile approaches, the surgeon must rely on precise anatomic landmarks and tactile feedback to navigate internervous and intermuscular planes safely.

Posterior Anatomy and the Sciatic Nerve
The minimally invasive posterior approach does not utilize a true internervous plane; rather, it involves a muscle-splitting dissection through the gluteus maximus (innervated by the inferior gluteal nerve). The critical deep structures include the short external rotators: the piriformis, superior gemellus, obturator internus, inferior gemellus, and quadratus femoris. In MIS techniques, preservation of the quadratus femoris and the piriformis is often attempted to enhance dynamic stability and protect the medial circumflex femoral artery (MFCA), which provides the primary blood supply to the femoral head and neck. The sciatic nerve, exiting the greater sciatic foramen typically inferior to the piriformis, lies in close proximity to the posterior acetabular column. Retractor placement during a mini-posterior approach must be meticulous to avoid compression or traction injuries to the sciatic nerve.
Anterior Anatomy and the Hueter Interval
The minimally invasive direct anterior approach (DAA) utilizes the Hueter interval, a true internervous and intermuscular plane. Superficially, the plane lies between the tensor fasciae latae (TFL), innervated by the superior gluteal nerve, and the sartorius, innervated by the femoral nerve. Deeply, the dissection passes between the rectus femoris (femoral nerve) and the gluteus medius (superior gluteal nerve). A critical vascular structure encountered in this approach is the ascending branch of the lateral circumflex femoral artery (LFCA), which must be identified and ligated to prevent postoperative hematoma. Additionally, the lateral femoral cutaneous nerve (LFCN) crosses the operative field anteriorly; careful fascial incision and medial retraction of the sartorius are required to prevent iatrogenic neuropraxia or neuroma formation.
Biomechanical Objectives
Regardless of the approach utilized, the biomechanical objectives of THA remain immutable. The surgeon must restore the center of rotation, optimize femoral offset, and equalize leg lengths. Failure to restore femoral offset can result in abductor weakness, increased joint reactive forces, and impingement. Minimally invasive techniques mandate that the surgeon achieve these biomechanical goals through a restricted window, heavily relying on preoperative templating and intraoperative fluoroscopy or navigation, particularly in the direct anterior and two-incision techniques.
Indications and Contraindications
When considering minimally invasive THA, rigorous patient selection is paramount. The primary objective is to avoid intraoperative difficulties with exposure that could ultimately compromise the safety of the procedure, lead to component malposition, or result in iatrogenic fracture. Surgeon inexperience or lack of specialized training in MIS techniques is a significant relative contraindication; the learning curve is steep, and the threshold to convert to a standard extensile approach must remain low.
Contraindications that assist with patient selection generally include complicated primary THA, revision surgery, severe hip dysplasia (Crowe grade III or IV), a body mass index (BMI) considerably higher than 30 kg/m², highly muscular patients, severely osteoporotic bone, and very stiff or ankylosed joints (Vail, 2005). Each case must be evaluated individually, balancing the theoretical benefits of rapid recovery against the risks of restricted visualization.
| Category | Operative Indications for MIS THA | Non Operative Management or Contraindications to MIS |
|---|---|---|
| Patient Factors | BMI < 30 kg/m², motivated for rapid rehab, standard primary osteoarthritis, avascular necrosis | BMI > 35 kg/m², extremely muscular habitus, severe osteoporosis, poorly controlled medical comorbidities |
| Anatomic Factors | Standard primary anatomy, mobile hip joint, mild to moderate deformity | Severe hip dysplasia (Crowe III/IV), protrusio acetabuli, prior complex pelvic trauma, severe joint stiffness |
| Surgical Factors | Primary arthroplasty, surgeon has surpassed the MIS learning curve (>50 cases) | Revision THA, hardware removal required, surgeon inexperience |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is non-negotiable in MIS THA. The restricted visual field diminishes the surgeon's ability to make large intraoperative adjustments based on gross anatomic landmarks.
Digital Templating Principles
Digital templating using calibrated anteroposterior (AP) pelvis and lateral hip radiographs is utilized to estimate the required acetabular component size, depth of reaming, and optimal position of the center of rotation. On the femoral side, templating determines the level of the femoral neck osteotomy, the anticipated stem size, offset options (standard vs. high offset), and the required head length to restore leg length and soft tissue tension. In MIS THA, the templated neck cut distance from the lesser trochanter serves as a critical intraoperative guide, as the entire proximal femur may not be simultaneously visible.

Patient Positioning and Operating Room Setup
Positioning dictates the surgical approach and the gravitational assistance required for soft tissue retraction.
For the minimally invasive single-incision posterior and anterolateral approaches, the patient is placed in the lateral decubitus position. Rigid pelvic fixation using peg boards or specialized clamp positioners is critical to ensure the pelvis remains orthogonal to the floor. Any unrecognized pelvic roll (anterior or posterior) during the procedure will directly translate to errors in acetabular cup version and inclination.
For the minimally invasive direct anterior approach, the patient is typically positioned supine. This can be performed on a standard radiolucent operating table, often utilizing a bump under the sacrum to extend the hips, or on a specialized orthopedic traction table (e.g., Hana table). The traction table allows for precise control of leg length, traction, and rotation, facilitating femoral elevation without the need for extensive soft tissue releases or multiple surgical assistants.

Detailed Surgical Approach and Technique
The single-incision techniques are essentially alterations to the standard posterior, anterolateral, and direct anterior approaches. These can be adopted on a graduated basis, with progressive reduction of incision length at a rate comfortable for the operating surgeon. Crucially, mini single-incision approaches allow for immediate extension into a standard extensile incision if necessary to gain additional exposure or manage an intraoperative complication.
Minimally Invasive Single Incision Posterior Approach
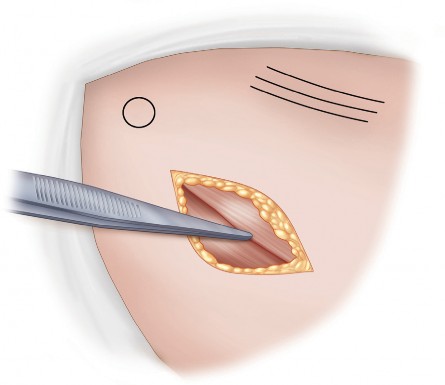
The patient is positioned in the lateral decubitus position. The incision is a short, oblique incision typically measuring 8 to 10 cm, centered over the posterior aspect of the greater trochanter and extending proximally toward the posterior superior iliac spine (PSIS). Alternatively, the surgeon may utilize the middle third of what would be the standard incision for the posterior approach.

Following the skin incision, the subcutaneous tissues are sharply dissected to expose the fascia lata and the gluteus maximus fascia. The fascia is incised in line with the skin incision. The gluteus maximus muscle fibers are bluntly split, taking care to coagulate any crossing vessels. A Charnley or similar self-retaining retractor is placed to maintain the fascial opening.
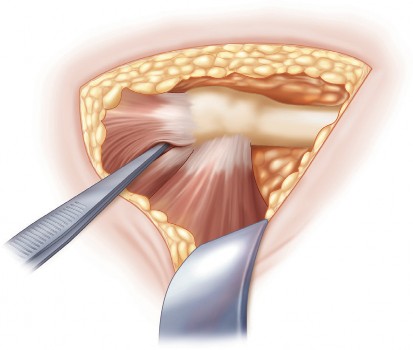
Deep dissection involves identifying the posterior border of the gluteus medius and retracting it anteriorly. The short external rotators (piriformis, superior gemellus, obturator internus, and inferior gemellus) are identified. In a tissue-sparing approach, an effort is made to preserve the piriformis and quadratus femoris if possible. The conjoint tendon of the short external rotators is sharply detached from its insertion at the piriformis fossa.
Clinical Pearl: Regardless of how this capsulotendinous flap is created, it is highly beneficial to tag it with heavy, non-absorbable sutures (e.g., #2 Ethibond or FiberWire) immediately upon detachment. This facilitates retraction during the procedure and ensures an anatomic, robust repair at the conclusion of the surgery, which is critical for minimizing the postoperative dislocation risk.
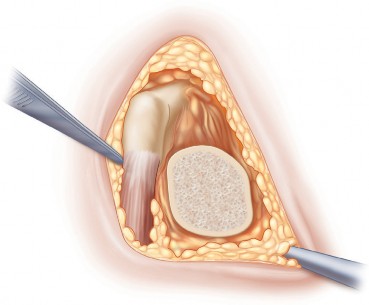
A posterior capsulotomy is performed, and the hip is gently dislocated through internal rotation, flexion, and adduction. Care must be taken to avoid excessive torsional forces that could result in an iatrogenic spiral fracture of the femoral shaft. The femoral neck osteotomy is performed according to preoperative templating.

Acetabular exposure is achieved using specialized MIS retractors. A Hohmann retractor is placed anteriorly over the anterior column, a second retractor is placed inferiorly beneath the transverse acetabular ligament, and a third is placed posteriorly to protect the sciatic nerve and retract the posterior capsule. The acetabulum is sequentially reamed to bleeding subchondral bone, and the hemispherical cup is impacted into place, targeting 40-45 degrees of inclination and 15-20 degrees of anteversion.
Femoral preparation requires anterior translation and internal rotation of the proximal femur. A calcar retractor is placed beneath the proximal femur to elevate it into the operative wound. The femoral canal is sequentially broached to achieve rotational stability and cortical contact. Following trial reduction and confirmation of stability, leg length, and offset, the definitive components are implanted. The tagged short external rotators and capsule are meticulously repaired to the greater trochanter through transosseous tunnels.
Minimally Invasive Direct Anterior Approach
The direct anterior approach (DAA) is performed with the patient supine. The incision typically begins 2-3 cm lateral and distal to the anterior superior iliac spine (ASIS) and extends distally for 8-10 cm, directed toward the lateral patella.
The superficial fascia is incised, and the TFL is identified. The fascia over the TFL is incised longitudinally, and the muscle belly is retracted laterally. This exposes the deeper layer of fascia covering the rectus femoris. The Hueter interval is developed bluntly. The ascending branches of the LFCA are consistently encountered crossing this interval; they must be isolated, clamped, and ligated or heavily cauterized to prevent postoperative bleeding.
The anterior capsule is exposed and either excised or incised via a T-shaped or H-shaped capsulotomy. Unlike the posterior approach, the hip is typically not dislocated prior to the neck cut. The femoral neck osteotomy is performed in situ using a dual-cut technique to remove a napkin-ring segment of the neck, facilitating the extraction of the femoral head using a corkscrew.
Acetabular preparation is highly direct, as the surgeon is looking straight down into the cup. Following cup insertion, femoral exposure represents the most challenging aspect of the DAA. The operative table is extended, and the leg is externally rotated and adducted. A specialized femoral elevator (e.g., a Mueller or hook retractor) is placed behind the greater trochanter to lift the proximal femur anteriorly. Sequential broaching is performed, taking care to avoid varus malalignment or fracture of the greater trochanter. Intraoperative fluoroscopy is frequently utilized to verify component positioning and sizing.
Minimally Invasive Two Incision Approach
The two-incision technique represents a drastically different paradigm for THA. It utilizes separate, distinct micro-incisions to insert the acetabular and femoral components independently.
The anterior incision, approximately 4-5 cm in length, is utilized exclusively for the preparation of the acetabulum and insertion of the acetabular cup. The approach utilizes the same Hueter interval as the DAA. Once the cup is seated, a second posterior incision, typically 3-4 cm in length, is made over the piriformis fossa under fluoroscopic guidance. This posterior portal is used to ream and broach the femoral canal and insert the femoral stem.
While theoretically minimizing soft tissue disruption to the greatest extent, the two-incision approach is technically demanding, heavily reliant on continuous fluoroscopy, and associated with a prolonged learning curve. Due to higher reported rates of complications, including proximal femoral fractures and component malposition in early series, this technique has largely fallen out of favor in mainstream orthopedic practice, though it remains a historically significant milestone in the evolution of MIS THA.
Complications and Management
The pursuit of smaller incisions must never compromise the execution of the arthroplasty. The restricted visualization inherent to MIS THA introduces unique risks, primarily related to spatial orientation and the forceful retraction of soft tissues. The learning curve for these procedures is widely documented, with complication rates significantly higher in a surgeon's first 50 cases.

| Complication | Incidence and Risk Factors | Salvage Strategy and Management |
|---|---|---|
| Intraoperative Periprosthetic Fracture | Higher in DAA (femoral shaft/calcar) and Two-Incision. Associated with osteoporotic bone and forceful femoral elevation. | Immediate extension of the incision. Cable cerclage for calcar cracks. Long-stem revision implants for distal extension fractures. |
| Component Malposition | Increased risk due to loss of visual anatomic landmarks. Acetabular retroversion or femoral varus are common. | Utilization of intraoperative fluoroscopy or navigation. Strict adherence to preoperative templating. Lower threshold to extend the incision. |
| Neurovascular Injury | LFCN neuropraxia in DAA (up to 10-15%). Sciatic nerve injury in posterior approach due to retractor pressure. | Protect LFCN by incising TFL fascia laterally. Ensure posterior retractors rest on bone, not soft tissue. Remove retractors periodically to relieve tension. |
| Wound Healing Complications | Skin edge necrosis due to excessive retractor tension on a small incision. | Avoid aggressive static retraction. Use mobile windows (moving the skin window dynamically). Ensure meticulous layered closure. |
| Infection (PJI) | Risk is comparable to standard THA, potentially elevated if tissue ischemia occurs from severe retraction. | Standard irrigation and debridement protocols. DAIR (Debridement, Antibiotics, and Implant Retention) for acute postoperative infections. |
Post Operative Rehabilitation Protocols
The primary driver for the adoption of minimally invasive THA is the potential for accelerated postoperative rehabilitation. MIS techniques are frequently paired with Enhanced Recovery After Surgery (ERAS) pathways. These multimodal protocols begin preoperatively with patient optimization and education, continue intraoperatively with regional anesthesia (e.g., spinal anesthesia) and periarticular local anesthetic infiltration, and culminate in aggressive postoperative physical therapy.

Patients are typically allowed to weight-bear as tolerated (WBAT) immediately following surgery. Mobilization often begins on postoperative day zero (POD 0), within hours of the procedure. The preservation of the abductor musculature (gluteus medius and minimus) in both the mini-posterior and direct anterior approaches facilitates early ambulation without the pronounced Trendelenburg gait often seen in traditional transgluteal (Hardinge) approaches.
Standard hip precautions are dictated by the specific approach utilized. For the mini-posterior approach, patients are traditionally instructed to avoid combined flexion greater than 90 degrees, adduction across the midline, and internal rotation to mitigate the risk of posterior dislocation. For the direct anterior approach, precautions are generally less restrictive but may include avoiding extreme extension and external rotation to protect the anterior capsule. Physical therapy focuses on gait normalization, abductor strengthening, and restoring active range of motion.
Summary of Key Literature and Guidelines
The academic literature regarding minimally invasive THA is extensive, characterized by a mix of enthusiastic early adoption and subsequent critical evaluation. It is important to realize that while short-term outcomes frequently demonstrate intended benefits, long-term survivorship data must be carefully scrutinized.
Early studies (e.g., Berger et al., Vail et al., 2005) highlighted the feasibility of MIS techniques, demonstrating reduced blood loss, shorter hospital stays, and faster return to independent ambulation in highly selected patient cohorts. However, subsequent large-scale registry data and randomized controlled trials have provided a more nuanced perspective.
Literature comparing the mini-posterior approach to the standard posterior approach generally shows a modest benefit in early pain scores and functional milestones at 2 to 6 weeks postoperatively. By 3 to 6 months, these differences largely equilibrate, with patients achieving similar functional outcomes regardless of incision length.
The direct anterior approach has shown statistically significant benefits in the immediate postoperative period regarding functional recovery and a lower risk of dislocation compared to traditional posterior approaches. However, this is counterbalanced by a higher incidence of early learning-curve complications, specifically periprosthetic fractures and LFCN neuropraxia.
Current guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the American Association of Hip and Knee Surgeons (AAHKS) do not definitively mandate one specific surgical approach over another. The consensus remains that the optimal approach is the one with which the operating surgeon is most experienced and comfortable. The ultimate success of a Total Hip Arthroplasty is dictated not by the length of the cutaneous incision, but by the precise execution of the bony cuts, accurate component positioning, and the meticulous restoration of hip biomechanics.
You Might Also Like


