Orthopedic With Answer Foot Review | Dr Hutaif Foot & A -...
14 Apr 2026
51 min read
97 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic With Answer Foot Review | Dr Hutai...
00:00
Start Quiz
Question 1High Yield
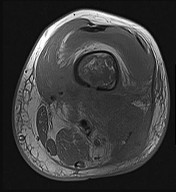
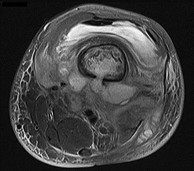
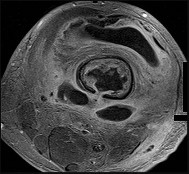
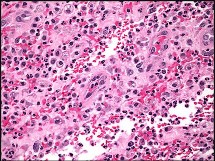
Figures 89a through 89g are the radiographs, MR images, and biopsy specimen of a 32-year-old man who has chronic left thigh and knee pain and recent knee swelling with no specific trauma or injury. The pain is exacerbated with activity but is also present at rest and at night. What is the most appropriate treatment?






Explanation
The radiographs show a lytic, destructive, poorly marginated femur lesion. MR imaging confirms the infiltrative nature of the lesion, a communication with the joint, and a substantial nonenhancing joint effusion. Biopsy confirms numerous polymorphonuclear neutrophils consistent with osteomyelitis with septic arthritis. The treatment of femur osteomyelitis with a septic knee includes aggressive debridement of all nonviable tissue, placement of antibiotic beads, and IV antibiotics. Surgical wide resection and endoprosthetic reconstruction would be considered only if the lesion were a low-grade malignancy. Aggressive curettage with allograft placement would be considered for benign tumors. Allograft placement is not appropriate in the setting of an infection. Chemotherapy followed by wide surgical resection and reconstruction is only appropriate for a high-grade malignancy.
RECOMMENDED READINGS
82. [Lew DP, Waldvogel FA. Osteomyelitis. Lancet. 2004 Jul 24-30;364(9431):369-79. Review. PubMed PMID: 15276398.](http://www.ncbi.nlm.nih.gov/pubmed/15276398)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15276398)
83. [Tetsworth K, Cierny G 3rd. Osteomyelitis debridement techniques. Clin Orthop Relat Res. 1999 Mar;(360):87-96. Review. PubMed PMID: 10101313.](http://www.ncbi.nlm.nih.gov/pubmed/10101313)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10101313)
84. [Karchevsky M, Schweitzer ME, Morrison WB, Parellada JA. MRI findings of septic arthritis and associated osteomyelitis in adults. AJR Am J Roentgenol. 2004 Jan;182(1):119-22. PubMed PMID: 14684523.](http://www.ncbi.nlm.nih.gov/pubmed/14684523)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14684523)
CLINICAL SITUATION FOR QUESTIONS 90 AND 91
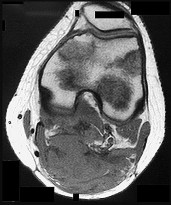
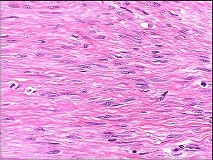
Figures 90a and 90b are the axial MR image and histology of a 27-year-old woman who has a firm lesion in the popliteal fossa. Figure 90c is the gross specimen after resection.
RECOMMENDED READINGS
82. [Lew DP, Waldvogel FA. Osteomyelitis. Lancet. 2004 Jul 24-30;364(9431):369-79. Review. PubMed PMID: 15276398.](http://www.ncbi.nlm.nih.gov/pubmed/15276398)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15276398)
83. [Tetsworth K, Cierny G 3rd. Osteomyelitis debridement techniques. Clin Orthop Relat Res. 1999 Mar;(360):87-96. Review. PubMed PMID: 10101313.](http://www.ncbi.nlm.nih.gov/pubmed/10101313)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10101313)
84. [Karchevsky M, Schweitzer ME, Morrison WB, Parellada JA. MRI findings of septic arthritis and associated osteomyelitis in adults. AJR Am J Roentgenol. 2004 Jan;182(1):119-22. PubMed PMID: 14684523.](http://www.ncbi.nlm.nih.gov/pubmed/14684523)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14684523)
CLINICAL SITUATION FOR QUESTIONS 90 AND 91
Figures 90a and 90b are the axial MR image and histology of a 27-year-old woman who has a firm lesion in the popliteal fossa. Figure 90c is the gross specimen after resection.
Question 2High Yield
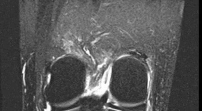
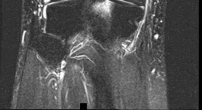
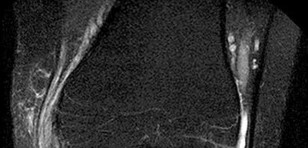
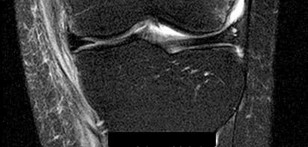
Figures 1 through 3 are the weight-bearing radiograph and MRI scans of a 27-year-old man who twisted his knee coming down awkwardly from a lay-up during a basketball game. He felt a sharp stabbing pain in the posterior aspect of his knee at the time of the injury. Physical examination reveals a trace effusion, full range of motion but pain with hyperflexion >90° degrees and tenderness over the affected joint line. What is the most appropriate treatment at this time?
---
---
---
---
---
---


Explanation
The MRI scan shows a posterior horn medial meniscus root avulsion with bony edema at the tibial root insertion. The radiograph shows no significant degenerative changes. If left untreated, posterior meniscal
root tears lead to progressive degenerative changes as a result of the altered tibiofemoral contact pressures and areas. Nonsurgical treatment including injections, physical therapy, and unloader braces are more _appropriate in the older patient with pre-existing advanced degenerative changes._
root tears lead to progressive degenerative changes as a result of the altered tibiofemoral contact pressures and areas. Nonsurgical treatment including injections, physical therapy, and unloader braces are more _appropriate in the older patient with pre-existing advanced degenerative changes._
Question 3High Yield
Slide 1
The structure on the side of the metatarsophalangeal joint of the second toe which is marked by the pointer is the:
The structure on the side of the metatarsophalangeal joint of the second toe which is marked by the pointer is the:
Explanation
The structure is the volar plate ligament. This ligament may assume a pathologic role in claw toe deformity and instability of the metatarsophalangeal joint.
Question 4High Yield
What measure of physiologic status best evaluates whether an injured patient is fully resuscitated and best predicts that perioperative complications will be minimized following definitive stabilization of long bone fractures?
Explanation
Serum lactate levels can be used to evaluate the effectiveness of the resuscitation of patients who have multiple injuries. Even after resuscitation, patients may have occult hypoperfusion as defined by a serum lactate level of greater than 2.5 mmol/L. The studies referenced indicate that these patients are at increased risk of perioperative complications such as organ failure or adult respiratory distress syndrome if definitive surgical fixation of the orthopaedic injuries is pursued prior to correction of the occult hypoperfusion. The other markers may be an indication of current physiology but have not been correlated with perioperative risks.
REFERENCES: Blow O, Magliore L, Claridge JA, et al: The golden hour and silver day: Detection and correction of occult hypoperfusion within 24 hours improves outcomes from major trauma. J Trauma 1999;47:964-977.
Crowl A, Young JS, Kahler DM, et al: Occult hypoperfusion is associated with increased morbidity in patients undergoing early femur fracture fixation. J Trauma 2000;48:260-267.
Shulman AM: Prediction of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:725-800.
REFERENCES: Blow O, Magliore L, Claridge JA, et al: The golden hour and silver day: Detection and correction of occult hypoperfusion within 24 hours improves outcomes from major trauma. J Trauma 1999;47:964-977.
Crowl A, Young JS, Kahler DM, et al: Occult hypoperfusion is associated with increased morbidity in patients undergoing early femur fracture fixation. J Trauma 2000;48:260-267.
Shulman AM: Prediction of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:725-800.
Question 5High Yield
The examination suggests a neurologic deficit of which nerve?
Explanation
- Common peroneal nerve
Question 6High Yield
Which of the following properties is false concerning articular cartilage:
Explanation
Important properties of articular cartilage include: Avascular (no blood vessels)
Aneural (no nerve fibers) Alymphatic (no lymphatic vessels)
Very low friction on cartilage on cartilage motion
Self-renewing (maintenance and restoration of extracellular matrix) With aging, loss of ability to maintain the extracellular matrix
C orrect Answer: Moderate friction on cartilage-on-cartilage motion
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
Aneural (no nerve fibers) Alymphatic (no lymphatic vessels)
Very low friction on cartilage on cartilage motion
Self-renewing (maintenance and restoration of extracellular matrix) With aging, loss of ability to maintain the extracellular matrix
C orrect Answer: Moderate friction on cartilage-on-cartilage motion
.v4b{border:2px solid #0984e3;background:#fff;color:#0984e3;padding:8px 20px;border-radius:25px;cursor:pointer;margin-right:10px;font-weight:bold;transition:0.3s;}
.v4b.active{background:#0984e3;color:#fff;}
.v4b:hover:not(.active){background:#e3f2fd;}
.mcq-v4-card{background:#fff;border-radius:15px;padding:35px;margin-bottom:40px;border:1px solid #e1e8ed;box-shadow:0 5px 15px rgba(0,0,0,0.04);}
.card-meta{color:#0984e3;font-weight:800;margin-bottom:20px;letter-spacing:1.5px;font-size:0.95rem;}
.q-stem{font-size:1.25rem;margin-bottom:30px;font-weight:500;line-height:1.7;color:#2d3436;}
.q-opt{display:flex;align-items:center;padding:15px;border:2px solid #f1f2f6;border-radius:12px;margin-bottom:15px;cursor:pointer;transition:all 0.2s ease-in-out;background:#fff;}
.q-opt:hover{border-color:#0984e3;background:#f0f7ff;transform:translateX(5px);}
.q-opt-circle{width:35px;height:35px;border:2px solid #ddd;border-radius:50%;display:flex;align-items:center;justify-content:center;margin-right:20px;font-weight:bold;background:#fafafa;flex-shrink:0;color:#636e72;}
.q-opt.correct{background:#e3fcef;border-color:#00b894;}
.q-opt.correct .q-opt-circle{background:#00b894;color:#fff;border-color:#00b894;}
.q-opt.wrong{background:#fff5f5;border-color:#ff7675;}
.q-opt.wrong .q-opt-circle{background:#ff7675;color:#fff;border-color:#ff7675;}
.q-opt.selected{border-color:#0984e3;background:#e3f2fd;}
.q-opt.selected .q-opt-circle{background:#0984e3;color:#fff;border-color:#0984e3;}
.q-feedback{margin-top:30px;padding:25px;background:#f8f9fa;border-left:6px solid #0984e3;border-radius:8px;}
.feedback-label{font-weight:bold;margin-bottom:15px;font-size:1.2rem;}
.explanation-text{line-height:1.7;color:#444;font-size:1.05rem;}
var v4E={
m:'study',r:new Map(),
setMode:function(m){this.m=m;document.getElementById('v4s').classList.toggle('active',m=='study');document.getElementById('v4e').classList.toggle('active',m=='exam');document.getElementById('v4xa').style.display=m=='exam'?'block':'none';this.reset();},
reset:function(){document.querySelectorAll('.q-opt').forEach(e=>{e.className='q-opt';e.style.pointerEvents='auto';});document.querySelectorAll('.q-feedback').forEach(e=>e.style.display='none');this.r.clear();this.up();},
up:function(){let s=0;this.r.forEach(v=>{if(v===true||v.s==v.c)s++;});const t=document.querySelectorAll('.mcq-v4-card').length;document.getElementById('v4sc').innerText=Math.round((s/t)*100)||0;},
reveal:function(c,s,k){const o=c.querySelectorAll('.q-opt');if(o[k-1])o[k-1].classList.add('correct');if(s!=k && o[s-1])o[s-1].classList.add('wrong');c.querySelector('.q-feedback').style.display='block';const fl=c.querySelector('.feedback-label');fl.innerHTML=s==k?' Correct Answer':' Incorrect';},
finish:function(){this.r.forEach((v,k)=>{this.reveal(document.getElementById('card-'+k),v.s,v.c);});document.querySelectorAll('.q-opt').forEach(e=>e.style.pointerEvents='none');window.scrollTo({top:0,behavior:'smooth'});}
};
document.querySelectorAll('.q-opt').forEach(el=>{
el.onclick=function(){
const q=this.dataset.q,k=this.dataset.correct,s=this.dataset.idx,p=this.closest('.mcq-v4-card');
if(v4E.m=='study') { if(v4E.r.has(q))return; v4E.r.set(q,s==k); p.querySelectorAll('.q-opt').forEach(o=>o.style.pointerEvents='none'); v4E.reveal(p,s,k); }
else { p.querySelectorAll('.q-opt').forEach(o=>o.classList.remove('selected')); this.classList.add('selected'); v4E.r.set(q,{s:s,c:k}); }
v4E.up();
};
});
Question 7High Yield
Which of the following is true regarding brace treatment for Scheuermann kyphosis:
Explanation
Brace treatment is effective for Scheuermann kyphosis. Unlike idiopathic scoliosis, permanent improvement of the deformity is the goal.
The Milwaukee brace is often indicated.
Brace treatment is ineffective for curves over 74°. The brace should be worn until skeletal maturity.
The Milwaukee brace is often indicated.
Brace treatment is ineffective for curves over 74°. The brace should be worn until skeletal maturity.
Question 8High Yield
..Figure 93 is the radiograph of a 72-year-old woman. Treatment includes fixation of the ulna. What options are recommended for the radius?

Explanation
- Radial head replacement to restore radiocapitellar contact
CLINICAL SITUATION FOR QUESTIONS 94 THROUGH 96
Figure 94 is the anteroposterior radiograph of a 75-year-old woman who has a 5-year history of progressive pain, crepitus, and loss of motion in her shoulder. She had a rotator cuff repair 10 years ago. Examination reveals 60 degrees of active forward elevation and 20 degrees of external rotation with her arm at her side. Passively she can be brought to 160 degrees of forward elevation and 90 degrees of external rotation with her arm at her side. A glenohumeral joint injection with local anesthetic eliminated pain, but there is no observed change in active motion.
CLINICAL SITUATION FOR QUESTIONS 94 THROUGH 96
Figure 94 is the anteroposterior radiograph of a 75-year-old woman who has a 5-year history of progressive pain, crepitus, and loss of motion in her shoulder. She had a rotator cuff repair 10 years ago. Examination reveals 60 degrees of active forward elevation and 20 degrees of external rotation with her arm at her side. Passively she can be brought to 160 degrees of forward elevation and 90 degrees of external rotation with her arm at her side. A glenohumeral joint injection with local anesthetic eliminated pain, but there is no observed change in active motion.
Question 9High Yield
A 23-year-old woman has had a 3-year history of snapping and pain in her left hip. She notes that the snapping started while marathon training and is only problematic about 15 minutes into a run. Examination is consistent with a negative Stinchfield, negative logroll, negative flexion abduction/external rotation test (FABER) of the hip; however, she has a positive Ober test as she has difficulty adducting her hip across the midline in the lateral decubitus position. Management consisting of nonsteroidal antiinflammatory drugs and stretching has failed to improve her snapping. What is the most reliable surgical treatment?
Explanation
DISCUSSION: The patient has external-type snapping hip (coxa saltans). It is not uncommon for patients to have a very long duration of symptoms that limit running or other sporting activities, and commonly affects the downward leg (usually the left leg when running on the left side of the road). The snapping causes a profound bursitis at the greater trochanter, and occasionally corticosteroid injections may be helpful. Her physical examination does not suggest an intra-articular process, and is not consistent with an internal-type snapping hip, usually caused by the iliopsoas tendon as it moves over the iliopectineal eminence. Stretching is the mainstay of treatment, as testing with a positive Ober signifies a tight iliotibial band as the thigh has difficulty crossing the midline with adduction. Various iliotibial band lengthening procedures have been described, including a Z-plasty near the proximal origin of the iliotibial band. Release at Gerdy’s tubercle has not been described.
REFERENCES: Provencher MT, Hofmeister EP, Muldoon MP: The surgical treatment of external coxa saltans (the snapping hip) by Z-plasty of the iliotibial band. Am J Sports Med 2004;32:470-476.
Faraj A A, Moulton A, Sirivastava VM: Snapping iliotibial band: Report of ten cases and review of the literature. Acta Orthop Belg 2001;67:19-23.
Brignall CG, Stainsby GD: The snapping hip: Treatment by Z-plasty. J Bone Joint Surg Br 1991 ;73:253-
254.
REFERENCES: Provencher MT, Hofmeister EP, Muldoon MP: The surgical treatment of external coxa saltans (the snapping hip) by Z-plasty of the iliotibial band. Am J Sports Med 2004;32:470-476.
Faraj A A, Moulton A, Sirivastava VM: Snapping iliotibial band: Report of ten cases and review of the literature. Acta Orthop Belg 2001;67:19-23.
Brignall CG, Stainsby GD: The snapping hip: Treatment by Z-plasty. J Bone Joint Surg Br 1991 ;73:253-
254.
Question 10High Yield
Figures 91a and 91b
Explanation
- Embryonic vascular interruption
Question 11High Yield
Figure 53 shows the radiograph of a 48-year-old man who has a left side periprosthetic femoral fracture around the femoral stem of a previous revision hip arthroplasty. What is the most appropriate treatment?

Explanation
DISCUSSION: In type B3 fractures, the proximal femur is so deficient that it cannot be treated with open reduction and internal fixation or support a new femoral component. In younger patients, the femur can be reconstructed with allograft prosthesis composite to restore bone stock. Removal of the distal stem with trephines would compromise fixation with cement. Elderly and low-demand patients can be treated more simply with a cemented segmental replacement prosthesis, such as that used for tumor reconstruction.
REFERENCES: Parvizi J, Tarity TD, Slenker N, et al: Proximal femoral replacement in patients with non- neoplastic conditions. J Bone Joint Surg Am 2007;89:1036-1043.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Lee SR, Bostrom MP: Periprosthetic fractures of the femur after total hip arthroplasty. Instr Course Lect 2004;53:111-118.
Figure 54
DISCUSSION: In type B3 fractures, the proximal femur is so deficient that it cannot be treated with open reduction and internal fixation or support a new femoral component. In younger patients, the femur can be reconstructed with allograft prosthesis composite to restore bone stock. Removal of the distal stem with trephines would compromise fixation with cement. Elderly and low-demand patients can be treated more simply with a cemented segmental replacement prosthesis, such as that used for tumor reconstruction.
REFERENCES: Parvizi J, Tarity TD, Slenker N, et al: Proximal femoral replacement in patients with non- neoplastic conditions. J Bone Joint Surg Am 2007;89:1036-1043.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Lee SR, Bostrom MP: Periprosthetic fractures of the femur after total hip arthroplasty. Instr Course Lect 2004;53:111-118.
Figure 54
Question 12High Yield
Figures 1 through 3 are the MRI scans of a 56-year-old woman in good health who reports a 6-month history of shoulder pain and external rotation weakness. Her radiographs are unremarkable. What is the diagnosis?
Explanation
31
The images reveal T2-weighted MRI sequences with edema isolated to the infraspinatus. In the absence of a tear in the infraspinatus tendon, the edema is most likely due to compression of the suprascapular nerve in the spinoglenoid notch. As this pathology persists, progressive muscle atrophy and fatty infiltration can result. Compression of the suprascapular nerve in the suprascapular notch would have resulted in edema and weakness in both the supra- and infraspinatus muscles. Compression is commonly caused by cysts from the joint secondary to labral tears. A rotator cuff tear of the infraspinatus is not identified on these images, and there is no history of trauma provided. There is no evidence of an anteroinferior labral tear, nor would this be expected to result in external rotation weakness or MRI abnormality of the infraspinatus. Quadrilateral space syndrome results in compression of the axillary nerve, which supplies the teres minor.
Correcr
The images reveal T2-weighted MRI sequences with edema isolated to the infraspinatus. In the absence of a tear in the infraspinatus tendon, the edema is most likely due to compression of the suprascapular nerve in the spinoglenoid notch. As this pathology persists, progressive muscle atrophy and fatty infiltration can result. Compression of the suprascapular nerve in the suprascapular notch would have resulted in edema and weakness in both the supra- and infraspinatus muscles. Compression is commonly caused by cysts from the joint secondary to labral tears. A rotator cuff tear of the infraspinatus is not identified on these images, and there is no history of trauma provided. There is no evidence of an anteroinferior labral tear, nor would this be expected to result in external rotation weakness or MRI abnormality of the infraspinatus. Quadrilateral space syndrome results in compression of the axillary nerve, which supplies the teres minor.
Correcr
Question 13High Yield
Which of the following most accurately approximates the estimated risk of a musculoskeletal allograft containing the human immunodeficiency virus (HIV) despite adequate screening?
Explanation
6,000,000
DISCUSSION: The calculated risk of a musculoskeletal allograft containing HIV despite adequate screening has been estimated to be approximately 1 in 1.6 million. This estimate is based on the risk of HIV in the population, projected population estimates, and current methods of donor screening.
REFERENCES: McAllister D, Joyce M, Mann B, et al: Allograft update: The current status of tissue regulation, procurement, processing, and sterilization. Am J Sports Med 2007;2148-2158.
Buck B, Malinin T: Human bone and tissue allografts: Preparation and safety. Clin Orthop Relat Res 1994;303:8 -
17.
Buck B, Malinin T, Brown M: Bone transplantation and human immunodeficiency virus: An estimate of risk of acquired immunodeficiency syndrome (AIDS). Clin Orthop Relat Res 1989;240:129-136.
_A i;___
Figure 92
6,000,000
DISCUSSION: The calculated risk of a musculoskeletal allograft containing HIV despite adequate screening has been estimated to be approximately 1 in 1.6 million. This estimate is based on the risk of HIV in the population, projected population estimates, and current methods of donor screening.
REFERENCES: McAllister D, Joyce M, Mann B, et al: Allograft update: The current status of tissue regulation, procurement, processing, and sterilization. Am J Sports Med 2007;2148-2158.
Buck B, Malinin T: Human bone and tissue allografts: Preparation and safety. Clin Orthop Relat Res 1994;303:8 -
17.
Buck B, Malinin T, Brown M: Bone transplantation and human immunodeficiency virus: An estimate of risk of acquired immunodeficiency syndrome (AIDS). Clin Orthop Relat Res 1989;240:129-136.
_A i;___
Figure 92
Question 14High Yield
A 31-year-old male presents with persistent foot pain 4 months after falling from a ladder. He was treated with an ankle brace for a suspected ankle sprain at the time of injury. On exam there is tenderness about the lateral hindfoot, no laxity on anterior drawer
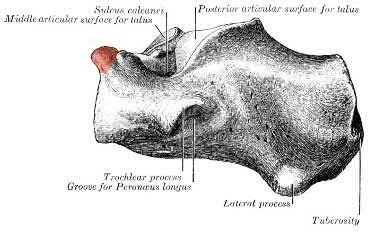
testing, and full eversion strength. Imaging demonstrates a nonunion of the anterior process of the calcaneus (Figure 1). Which of the following mechanisms and ligaments are involved?
testing, and full eversion strength. Imaging demonstrates a nonunion of the anterior process of the calcaneus (Figure 1). Which of the following mechanisms and ligaments are involved?

Explanation
The anterior process of the calcaneus is an attachment of the bifurcate ligament, which can be avulsed with excessive inversion and plantar flexion.
Calcaneal anterior process fractures are uncommon injuries that are easily missed at the initial presentation. They are prone to nonunion and may lead to long-term pain and disability. Three types have been described: Type I) nondisplaced avulsion, Type II) displaced avulsion not involving the calcaneocuboid articulation, and Type III) displaced involving the calcaneocuboid joint. The dorsal aspect of the process serves as an origin for the extensor digitorum brevis and the bifurcate ligament. The bifurcate ligament inserts on the dorsal navicular and cuboid and resists plantar flexion-inversion forces. This fracture is best identified using oblique radiographs of the foot or CT. Treatment is based on the degree of calcaneocuboid articular involvement and chronicity. Immobilization and non-weight bearing is the treatment of choice for acute nondisplaced fractures.
Trnka et al. reviewed fractures of the anterior superior calcaneal process. The authors noted that this injury is often missed and may lead to persistent pain distal to the sinus tarsi at the calcaneocuboid joint. Oblique foot radiographs should be carefully reviewed when patients present with pain about the lateral hindfoot. The mechanism most often implicated is an avulsion of the bifurcate
ligament during excessive inversion and plantar flexion. The authors conclude operative fixation should be considered earlier for type III fractures due to intraarticular involvement and risk of degenerative changes.
Berkowitz et al. reviewed process and tubercle fractures of the hindfoot. The authors highlight two potential mechanisms – avulsion from plantarflexion/inversion and shearing from forced dorsiflexion/eversion. On exam, tenderness and swelling will be approximately 2cm anterior and 1cm inferior to the ATFL. The authors noted successful treatment when approaching acute nondisplaced fractures with immobilization and non-weight bearing.
However, painful nonunions typically require either excision, ORIF, or arthrodesis. Surgical management should be considered acutely for fragments
>1cm in size and those with > 2mm intraarticular displacement. The authors conclude making the correct initial diagnosis is key to providing the best opportunity for complete recovery.
Figure 1 is a sagittal CT image of the hindfoot demonstrating a nonunion of the anterior process of the calcaneus.
Illustration A demonstrates the anterior process of the calcaneus, the origin of the bifurcate ligament.
Incorrect Answers
Answer 1: Inversion and dorsiflexion results places tension on the CFL. The CFL attaches to the lateral calcaneal body, not the anterior process.
Answer 3: Inversion and dorsiflexion injuries are associated with CFL tears. Additionally, as the name implies, the ATFL attaches to the dorsal talus, not the calcaneus.
Answer 4: Although the mechanism of an ATFL injury is an inversion and plantar flexion force, the ATFL attaches to the dorsal talus, not the calcaneus. Answer 5: The tibiocalcaneal ligament is one of four comprising the deltoid ligament, which can be injured with excessive eversion. However, these ligaments do not attach to the anterior process of the calcaneus.
Calcaneal anterior process fractures are uncommon injuries that are easily missed at the initial presentation. They are prone to nonunion and may lead to long-term pain and disability. Three types have been described: Type I) nondisplaced avulsion, Type II) displaced avulsion not involving the calcaneocuboid articulation, and Type III) displaced involving the calcaneocuboid joint. The dorsal aspect of the process serves as an origin for the extensor digitorum brevis and the bifurcate ligament. The bifurcate ligament inserts on the dorsal navicular and cuboid and resists plantar flexion-inversion forces. This fracture is best identified using oblique radiographs of the foot or CT. Treatment is based on the degree of calcaneocuboid articular involvement and chronicity. Immobilization and non-weight bearing is the treatment of choice for acute nondisplaced fractures.
Trnka et al. reviewed fractures of the anterior superior calcaneal process. The authors noted that this injury is often missed and may lead to persistent pain distal to the sinus tarsi at the calcaneocuboid joint. Oblique foot radiographs should be carefully reviewed when patients present with pain about the lateral hindfoot. The mechanism most often implicated is an avulsion of the bifurcate
ligament during excessive inversion and plantar flexion. The authors conclude operative fixation should be considered earlier for type III fractures due to intraarticular involvement and risk of degenerative changes.
Berkowitz et al. reviewed process and tubercle fractures of the hindfoot. The authors highlight two potential mechanisms – avulsion from plantarflexion/inversion and shearing from forced dorsiflexion/eversion. On exam, tenderness and swelling will be approximately 2cm anterior and 1cm inferior to the ATFL. The authors noted successful treatment when approaching acute nondisplaced fractures with immobilization and non-weight bearing.
However, painful nonunions typically require either excision, ORIF, or arthrodesis. Surgical management should be considered acutely for fragments
>1cm in size and those with > 2mm intraarticular displacement. The authors conclude making the correct initial diagnosis is key to providing the best opportunity for complete recovery.
Figure 1 is a sagittal CT image of the hindfoot demonstrating a nonunion of the anterior process of the calcaneus.
Illustration A demonstrates the anterior process of the calcaneus, the origin of the bifurcate ligament.
Incorrect Answers
Answer 1: Inversion and dorsiflexion results places tension on the CFL. The CFL attaches to the lateral calcaneal body, not the anterior process.
Answer 3: Inversion and dorsiflexion injuries are associated with CFL tears. Additionally, as the name implies, the ATFL attaches to the dorsal talus, not the calcaneus.
Answer 4: Although the mechanism of an ATFL injury is an inversion and plantar flexion force, the ATFL attaches to the dorsal talus, not the calcaneus. Answer 5: The tibiocalcaneal ligament is one of four comprising the deltoid ligament, which can be injured with excessive eversion. However, these ligaments do not attach to the anterior process of the calcaneus.
Question 15High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
A pathognomonic radiographic feature of this injury is a
---
---
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
A pathognomonic radiographic feature of this injury is a
---
---


Explanation
Coronal shear fractures of the distal end of the humerus are rare. Failure to recognize the fracture pattern can lead to poor patient outcomes secondary to poor surgical decision making. The double arc sign is considered a pathognomonic finding on the lateral elbow radiograph seen in Figure 2. This is created by the subchondral bone of the capitellum and lateral trochlear ridge. Excessive internal rotation of the fracture fragment or a subpar lateral radiograph can make recognition of this sign difficulty
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Question 16High Yield
Myositis ossificans is a recognized complication of contusion to the quadriceps muscle. During early rehabilitation, this condition is most likely to be exacerbated by
Explanation
Passive stretching is contraindicated during rehabilitation as it may potentiate the severity of the myositis ossificans. Electrical stimulation, iontophoresis, isometric exercise, and ice/heat contrast are not known to exacerbate this process.
REFERENCES: Brunet ME, Hontas RB: The thigh, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Cushner FD, Morwessel RM: Myositis ossificans traumatica. Orthop Rev 1992;21:1319-1326.
REFERENCES: Brunet ME, Hontas RB: The thigh, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Cushner FD, Morwessel RM: Myositis ossificans traumatica. Orthop Rev 1992;21:1319-1326.
Question 17High Yield
Compared with the medial parapatellar approach for total knee arthroplasty (TKA), quadriceps-sparing approaches are associated with
Explanation
Quadriceps-sparing approaches for TKA have shown higher risk of implant malalignment compared with the traditional medial parapatellar approach. No consistent clinically significant benefit to patient-reported outcomes has been demonstrated with quadriceps-sparing TKA, nor is there a significant improvement in postoperative quadriceps strength. Longer surgical and tourniquet times have been observed with “minimally invasive” approaches.
Question 18High Yield
A 19-year-old running back lands directly on his anterior knee after being tackled. He has mild anterior knee pain, a trace effusion, a 2+ posterior drawer, a grade 1A Lachman, no valgus laxity, and negative dial tests at 30° and 90°. What is the best treatment strategy at this time?
Explanation
This patient has likely sustained an isolated PCL injury. The examination is consistent with a grade II injury to the PCL. In patients with isolated PCL injuries, such as this scenario, the best initial option is nonsurgical treatment and return to play as symptoms subside and strength improves. Physical therapy and delayed PCL reconstruction is not the
ecause this patient can likely be treated without surgery. The absence of valgus laxity and negative dial testing findings suggest that an injury to the posteromedial and posterolateral corners has not occurred. Initial nonsurgical treatment is indicated for this patient. If he completes rehabilitation and experiences persistent disability with anterior and/or medial knee discomfort or senses the knee is "loose," PCL reconstruction should be considered at that time.
Correct answer : A
ecause this patient can likely be treated without surgery. The absence of valgus laxity and negative dial testing findings suggest that an injury to the posteromedial and posterolateral corners has not occurred. Initial nonsurgical treatment is indicated for this patient. If he completes rehabilitation and experiences persistent disability with anterior and/or medial knee discomfort or senses the knee is "loose," PCL reconstruction should be considered at that time.
Correct answer : A
Question 19High Yield
What condition favors pollicization in hypoplasia of the thumb?
Explanation
The decision to ablate and pollicize vs preserve and reconstruct is based on the stability of the carpometacarpal joint. A stable thumb is more easily used in prehension activities of grasping and pinching. All other responses are associated with surgical options for reconstruction of the thumb. The carpometacarpal joint is the “keystone” for thumb-to-hand attachment. Without a stable carpometacarpal joint, pollicization may be required. No other response necessitates pollicization.
RECOMMENDED READINGS
1. [McCarroll HR. Congenital anomalies: a 25-year overview. J Hand Surg Am. 2000 Nov;25(6):1007-37. Review. PubMed PMID: 11119659. ](http://www.ncbi.nlm.nih.gov/pubmed/11119659)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11119659)
2. [Manske PR, Goldfarb CA. Congenital failure of formation of the upper limb. Hand Clin. 2009 May;25(2):157-70. doi: 10.1016/j.hcl.2008.10.005. Review. PubMed PMID: 19380058.](http://www.ncbi.nlm.nih.gov/pubmed/19380058)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19380058)
38
RESPONSES FOR QUESTIONS 41 THROUGH 44
Match the patient and image with the treatment listed.
RECOMMENDED READINGS
1. [McCarroll HR. Congenital anomalies: a 25-year overview. J Hand Surg Am. 2000 Nov;25(6):1007-37. Review. PubMed PMID: 11119659. ](http://www.ncbi.nlm.nih.gov/pubmed/11119659)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11119659)
2. [Manske PR, Goldfarb CA. Congenital failure of formation of the upper limb. Hand Clin. 2009 May;25(2):157-70. doi: 10.1016/j.hcl.2008.10.005. Review. PubMed PMID: 19380058.](http://www.ncbi.nlm.nih.gov/pubmed/19380058)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19380058)
38
RESPONSES FOR QUESTIONS 41 THROUGH 44
Match the patient and image with the treatment listed.
Question 20High Yield
Structure responsible for the pivot shift phenomenon as it transitions to become a knee flexor from being a knee extensor, thereby causing tibial reduction
Explanation
- Figure 13b
Question 21High Yield
A tendon repair is thought to be weakest during which phase of tendon healing?
Explanation
**
Healing after a tendon repair or rupture has the following stages: inflammatory, cellular proliferation, and remodeling. During the inflammatory phase, neutrophils and macrophages migrate into the injury site and release chemotactic factors that recruit fibroblasts. A tendon is thought to be weakest
5 to 21 days after repair, which coincides with the inflammatory phase. During the proliferative phase, inflammatory cells secrete cytokines and growth
factors (platelet-derived growth factor, insulin-like growth factor, bone morphogenetic protein (BMP)-12 and BMP 13, and transforming growth factor- beta) that promote differentiation of fibroblasts. Fibrosis and decreased cellularity are the hallmarks of the remodeling stage.
Healing after a tendon repair or rupture has the following stages: inflammatory, cellular proliferation, and remodeling. During the inflammatory phase, neutrophils and macrophages migrate into the injury site and release chemotactic factors that recruit fibroblasts. A tendon is thought to be weakest
5 to 21 days after repair, which coincides with the inflammatory phase. During the proliferative phase, inflammatory cells secrete cytokines and growth
factors (platelet-derived growth factor, insulin-like growth factor, bone morphogenetic protein (BMP)-12 and BMP 13, and transforming growth factor- beta) that promote differentiation of fibroblasts. Fibrosis and decreased cellularity are the hallmarks of the remodeling stage.
Question 22High Yield
74
Figure 74 is the radiograph of a 31-year-old woman with a painful bunion deformity that has failed nonsurgical treatment.
Figure 74 is the radiograph of a 31-year-old woman with a painful bunion deformity that has failed nonsurgical treatment.
Explanation
- Distal first metatarsal chevron osteotomy
Question 23High Yield
What muscles are responsible for the most common deformity after antegrade intramedullary nailing for a subtrochanteric femur fracture?
Explanation
The most common deformity after antegrade nailing of a subtrochanteric femur fracture is varus and procurvatum (or flexion). This is caused by the hip abductors and iliopsoas pulling the proximal fragment into abduction and flexion, while the distal fragment is pulled into adduction from the adductors.
The reference by French et al is a review on 45 patients with subtrochanteric fractures treated with cephalomedullary interlocked nailing. Based on femoral neck-shaft angle, 61% of the fractures were reduced in at least 5º varus. The authors attributed this malalignment to failure to counteract muscle forces acting on the proximal fragment, combined with the adducted position of the distal femur during portal creation.
The reference by Ricci et al is a report of 403 femoral shaft fractures treated with intramedullary nailing. Patients with proximal femoral shaft fractures were found to have the highest incidence of malalignment. The most common deformity in this group was varus, followed by procurvatum (or flexion).
The reference by French et al is a review on 45 patients with subtrochanteric fractures treated with cephalomedullary interlocked nailing. Based on femoral neck-shaft angle, 61% of the fractures were reduced in at least 5º varus. The authors attributed this malalignment to failure to counteract muscle forces acting on the proximal fragment, combined with the adducted position of the distal femur during portal creation.
The reference by Ricci et al is a report of 403 femoral shaft fractures treated with intramedullary nailing. Patients with proximal femoral shaft fractures were found to have the highest incidence of malalignment. The most common deformity in this group was varus, followed by procurvatum (or flexion).
Question 24High Yield
A 7 5-year-old man who sustained an intertrochanteric hip fracture underwent open reduction and internal fixation with a sliding hip screw. Six months after the procedure, the patient has shortening and external rotation of the extremity and progressively severe groin pain with ambulation. Radiographs are shown in Figures 5a and 5b. What is the most appropriate management?

Explanation
DISCUSSION: The patient has an intertrochanteric fracture malunion with protrusion of the hardware and penetration into the acetabulum. To restore leg length and relieve pain, total hip arthroplasty is necessary. Valgus osteotomy is appropriate for fracture nonunion with an intact femoral head with no signs of osteonecrosis. Bipolar hemiarthroplasty with acetabular erosion will most likely lead to pain as will removal of the hardware with or without physical therapy.
REFERENCE: Said GZ, Farouk O, El-Sayed A, et al: Salvage of failed dynamic hip screw fixation of intertrochanteric fractures. Injury 2006;37:194-202.
Figure 6
DISCUSSION: The patient has an intertrochanteric fracture malunion with protrusion of the hardware and penetration into the acetabulum. To restore leg length and relieve pain, total hip arthroplasty is necessary. Valgus osteotomy is appropriate for fracture nonunion with an intact femoral head with no signs of osteonecrosis. Bipolar hemiarthroplasty with acetabular erosion will most likely lead to pain as will removal of the hardware with or without physical therapy.
REFERENCE: Said GZ, Farouk O, El-Sayed A, et al: Salvage of failed dynamic hip screw fixation of intertrochanteric fractures. Injury 2006;37:194-202.
Figure 6
Question 25High Yield
A series of axial T1-weighted MR images is shown in Figure 84. The postfracture MRI reveals tissue contamination by fracture hematoma. Based upon the MRI findings, which aspect of limb-sparing resection and reconstruction will be most challenging?
Explanation
- En bloc extra-articular resection of the knee joint_
Question 26High Yield
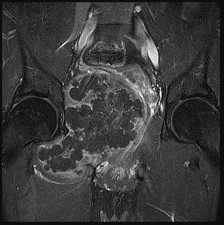
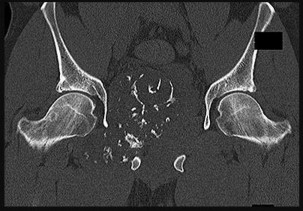
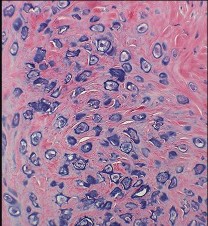
Figures 42a through 42d are the radiograph, CT scans, and biopsy specimen of a 38-year-old man who arrived at the emergency department with urinary retention. He has no other symptoms. What is the most appropriate treatment for this lesion?

Explanation
These images reveal a chondrosarcoma. On radiograph, chondrosarcoma is a fusiform, lucent defect with scalloping of the inner cortex and periosteal reaction. Extension into the soft tissue may be present, as well as punctate or stippled calcification of the cartilage matrix. Histologically, chondrosarcoma is differentiated from benign cartilage tumors by enlarged plump nuclei, multiple cells per lacunae, binucleated cells, and hyperchromic nuclear pleomorphism. Treatment of most chondrosarcomas is surgery only because adjuvant treatments are not effective.
RECOMMENDED READINGS
17. [Weber KL, Pring ME, Sim FH. Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res. 2002 Apr;(397):19-28. PubMed PMID: 11953591. ](http://www.ncbi.nlm.nih.gov/pubmed/11953591)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11953591)
18. [Rajani R, Gibbs CP. Treatment of Bone Tumors. Surg Pathol Clin. 2012 Mar 1;5(1):301-318. PubMed PMID: 22328909. ](http://www.ncbi.nlm.nih.gov/pubmed/22328909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22328909)
RECOMMENDED READINGS
17. [Weber KL, Pring ME, Sim FH. Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res. 2002 Apr;(397):19-28. PubMed PMID: 11953591. ](http://www.ncbi.nlm.nih.gov/pubmed/11953591)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11953591)
18. [Rajani R, Gibbs CP. Treatment of Bone Tumors. Surg Pathol Clin. 2012 Mar 1;5(1):301-318. PubMed PMID: 22328909. ](http://www.ncbi.nlm.nih.gov/pubmed/22328909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22328909)
Question 27High Yield
A 13-year-old girl with adolescent idiopathic scoliosis is otherwise healthy with a normal neurologic examination and she began her menstrual cycle 3 months ago. Standing radiographs show a high left thoracic curve from T1-T6 that measures 29 degrees, a right thoracic curve from T7-L1 that measures 65 degrees, and a left lumbar curve from L1-L5 that measures 31 degrees, correcting to 12, 37, and 10 degrees, respectively, on bending films. Her Risser sign is 1. What is the most appropriate management?
Explanation
The patient has typical adolescent idiopathic scoliosis with a right thoracic curve. This represents a Lenke-IB curve pattern; therefore, only treatment of the thoracic curve is required. The proximal thoracic and thoracolumbar curves are very flexible. The patient is Risser 1 and has just started her menstrual cycles; therefore, she is at significant risk for further curve progression. Bracing is not appropriate for a curve of this magnitude and will not halt the progression of this curve, nor will vertebral body stapling stop this curve. Vertebral body stapling is sometimes useful in small thoracic curves of less than 35 degrees and skeletally immature patients. Anterior and
14 • American Academy of Orthopaedic Surgeons
posterior spinal fusion is not required because the patient has no other risk factors, such as neurofibromatosis nor is she at risk for crankshaft. Anterior fusion is an option, but it is not listed.
REFERENCES: Lenke LG, Betz RR, Harmes J, et al: Adolescent idiopathic scoliosis: Anew classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 2001;83:1169-1181.
Lenke LG, Betz RR, Haher TR, et al: Multisurgeon assessment of surgical decision making in adolescent idiopathic scoliosis: Curve classification, operative approach, and fusion levels. Spine 2001;26:2347- 2353.
14 • American Academy of Orthopaedic Surgeons
posterior spinal fusion is not required because the patient has no other risk factors, such as neurofibromatosis nor is she at risk for crankshaft. Anterior fusion is an option, but it is not listed.
REFERENCES: Lenke LG, Betz RR, Harmes J, et al: Adolescent idiopathic scoliosis: Anew classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 2001;83:1169-1181.
Lenke LG, Betz RR, Haher TR, et al: Multisurgeon assessment of surgical decision making in adolescent idiopathic scoliosis: Curve classification, operative approach, and fusion levels. Spine 2001;26:2347- 2353.
Question 28High Yield
Figure 60a is the radiograph of an 18-year-old right-hand-dominant man who has pain and stiffness 3 months after sustaining an injury to his dominant ring finger while playing basketball. An examination reveals significant proximal interphalangeal (PIP) joint swelling with active and passive PIP joint motion of 15/40 degrees of flexion. What is the best next step?


Explanation
This patient has a subacute PIP joint dorsal fracture dislocation with involvement of 50% to 60% of the palmar articular surface of the base of P2. A “V sign” (Figure 60b) is evident, indicating
dorsal subluxation of the joint. In some cases, an ORIF is possible, but substantial comminution often precludes proper restoration of the critical volar buttress.
Therapy is not the answer because the joint is dorsally subluxated and must be corrected. Dynamic external fixation on its own would not result in a reduced joint. The hemi-hamate autograft has proven useful in this type of scenario and serves to restore the volar buttress of P2 using an osteochondral autograft harvested from the distal articular aspect of the hamate at its articulation with the fourth/fifth metacarpal bases. Intraoperative clinical photographs and a postsurgical radiograph are shown in Figures 60c through 60e.
RECOMMENDED READINGS
16. Calfee RP, Kiefhaber TR, Sommerkamp TG, Stern PJ. Hemi-hamate arthroplasty provides functional reconstruction of acute and chronic proximal interphalangeal fracture-dislocations. J Hand Surg Am. 2009 Sep;34(7):1232-41. doi: 10.1016/j.jhsa.2009.04.027. PubMed PMID: 19700071.
17. Frueh FS, Calcagni M, Lindenblatt N. The hemi-hamate autograft arthroplasty in proximal interphalangeal joint reconstruction: a systematic review. J Hand Surg Eur Vol. 2015 Jan;40(1):24-32. doi: 10.1177/1753193414554356. Epub 2014 Oct 22. Review. PubMed PMID: 25342651.
18. Williams RM, Hastings H 2nd, Kiefhaber TR. PIP Fracture/Dislocation Treatment Technique: Use of a Hemi-Hamate Resurfacing Arthroplasty. Tech Hand Up Extrem Surg. 2002 Dec;6(4):185-92. PubMed PMID: 16520599.
19. Williams RM, Kiefhaber TR, Sommerkamp TG, Stern PJ. Treatment of unstable dorsal proximal interphalangeal fracture/dislocations using a hemi-hamate autograft. J Hand Surg Am. 2003 Sep;28(5):856-65. PubMed PMID: 14507519.
dorsal subluxation of the joint. In some cases, an ORIF is possible, but substantial comminution often precludes proper restoration of the critical volar buttress.
Therapy is not the answer because the joint is dorsally subluxated and must be corrected. Dynamic external fixation on its own would not result in a reduced joint. The hemi-hamate autograft has proven useful in this type of scenario and serves to restore the volar buttress of P2 using an osteochondral autograft harvested from the distal articular aspect of the hamate at its articulation with the fourth/fifth metacarpal bases. Intraoperative clinical photographs and a postsurgical radiograph are shown in Figures 60c through 60e.
RECOMMENDED READINGS
16. Calfee RP, Kiefhaber TR, Sommerkamp TG, Stern PJ. Hemi-hamate arthroplasty provides functional reconstruction of acute and chronic proximal interphalangeal fracture-dislocations. J Hand Surg Am. 2009 Sep;34(7):1232-41. doi: 10.1016/j.jhsa.2009.04.027. PubMed PMID: 19700071.
17. Frueh FS, Calcagni M, Lindenblatt N. The hemi-hamate autograft arthroplasty in proximal interphalangeal joint reconstruction: a systematic review. J Hand Surg Eur Vol. 2015 Jan;40(1):24-32. doi: 10.1177/1753193414554356. Epub 2014 Oct 22. Review. PubMed PMID: 25342651.
18. Williams RM, Hastings H 2nd, Kiefhaber TR. PIP Fracture/Dislocation Treatment Technique: Use of a Hemi-Hamate Resurfacing Arthroplasty. Tech Hand Up Extrem Surg. 2002 Dec;6(4):185-92. PubMed PMID: 16520599.
19. Williams RM, Kiefhaber TR, Sommerkamp TG, Stern PJ. Treatment of unstable dorsal proximal interphalangeal fracture/dislocations using a hemi-hamate autograft. J Hand Surg Am. 2003 Sep;28(5):856-65. PubMed PMID: 14507519.
Question 29High Yield
Figures 1 and 2 are the radiographs of a 69-year-old man with a history of treated prostate cancer and hemodialysis-dependent end- stage renal disease who presents to the emergency department with progressively worsening right shoulder pain and stiffness. Laboratory tests reveal a white blood cell count of 17,000, erythrocyte sedimentation rate, 75, and CRP, 10.1. He has a draining sinus located along the anterior shoulder. What is the best next step?
33
33
Explanation
The patient's radiographs demonstrate bone loss of the medial humeral head. He has risk factors for both septic arthritis/osteomyelitis, and metastatic cancer, and it is important to understand the extent of his pathology before moving forward with surgical intervention. An MRI scan would assist in the diagnosis and demonstrate the extent of disease/tissue involvement. Administration of IV antibiotics prior to obtaining appropriate cultures would decrease the success rate of treatment in the setting of infection, and mistreat the pathology in the setting of metastasis. Similarly, obtaining cultures from the draining sinus tract would fail to account for the possible tumor diagnosis and may result in inaccurate culture results.
Question 30High Yield
A patient has a defined area of moderately increased activity in the femoral shaft consistent with a stress fracture (grade 2 by bone scan criteria). Which of the following is the corresponding finding on the magnetic resonance imaging scan:
Explanation
In 1995, Fredrickson and colleagues classified stress fractures into four grades based upon bone scans:
Grade 1     Small ill-defined cortical area of mildly increased activity Grade 2     Well-defined cortical area of moderately increased cortical                     activity
Grade 3Â Â Â Â Â Wide, cortical-medullary area of increased activity
Grade 4Â Â Â Â Â Transcortical area of intensely increased activity
C orrect Answer: High periosteal signal; normal marrow T1 signal; high marrow T2 signal
Grade 1     Small ill-defined cortical area of mildly increased activity Grade 2     Well-defined cortical area of moderately increased cortical                     activity
Grade 3Â Â Â Â Â Wide, cortical-medullary area of increased activity
Grade 4Â Â Â Â Â Transcortical area of intensely increased activity
C orrect Answer: High periosteal signal; normal marrow T1 signal; high marrow T2 signal
Question 31High Yield
A 56-year-old man sustained a nondisplaced extra-articular fracture of the proximal aspect of the third metatarsal after dropping a heavy object on his left foot. Management should consist of
Explanation
This injury pattern is one of a direct trauma to the mid aspect of the foot. Without additional forces involved, capsular ligamentous injury is not anticipated; therefore, the injury should be a stable pattern. Treatment should consist of protected weight bearing as tolerated in a walking boot or walking cast. Surgical intervention with open reduction and internal fixation, percutaneous pinning, or open reduction and internal fixation with primary tarsometatarsal joint fusion is not indicated with this pattern of injury. The use of external bone stimulation in this acute fracture setting is not indicated. With injuries to the midfoot area where the exact mechanism of injury is uncertain, there should be a high index of suspicion for an associated injury to the tarsometatarsal joint, and standing radiographs or stress radiographs should be obtained.
REFERENCES: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1265-1296.
Early JS: Fractures and dislocations of the midfoot and forefoot, in Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001,
pp 2181-2245.
REFERENCES: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1265-1296.
Early JS: Fractures and dislocations of the midfoot and forefoot, in Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001,
pp 2181-2245.
Question 32High Yield
A 17-year-old girl develops chronic posterolateral rotatory instability (PLRI) of the elbow following closed treatment of an elbow dislocation. Advanced imaging reveals incompetence of the lateral collateral ligament complex, and ligament reconstruction is planned. Examination under anesthesia is performed with the forearm in maximal supination and valgus force applied to the elbow, demonstrated in Video
Explanation
PLRI of the elbow is the most common form of chronic elbow instability. The mechanism occurs following a fall onto an outstretched hand, where a valgus force is applied to the elbow and the forearm rotates into progressive supination. This allows the radial head to translate posterior to the capitellum, with progressive injury from lateral to medial sides of the elbow. The pivot shift test is a useful examination maneuver to confirm the presence of PLRI. With the forearm in maximal supination and valgus stress applied to the elbow, the radial head is forced posterior to the capitellum as the elbow is brought into progressive extension, revealing a dimple on the lateral aspect of the elbow. This typically occurs at roughly 30° of flexion. As the elbow is flexed, the radial head reduces.
Question 33High Yield
Which of the following nerves is most commonly injured during revision surgery following a Bristow procedure?
Explanation
Because of the previously transferred bone block of coracoid and short arm flexors, the musculocutaneous nerve often scars along the anteroinferior glenohumeral capsule. Mobilization of this tissue places the nerve at greatest risk. The axillary nerve is also potentially at risk, but this is nonspecific to prior surgery, particularly the Bristow procedure.
REFERENCES: Norris TR: Complications following anterior instability repairs, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993,
pp 98-116.
Flatow EL, Bigliani LU, April EW: An anatomic study of the musculocutaneous nerve and its relationship to the coracoid process. Clin Orthop 1989;244:166-171.
REFERENCES: Norris TR: Complications following anterior instability repairs, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993,
pp 98-116.
Flatow EL, Bigliani LU, April EW: An anatomic study of the musculocutaneous nerve and its relationship to the coracoid process. Clin Orthop 1989;244:166-171.
Question 34High Yield
A 13-year-old right-hand dominant pitcher was treated for Little League shoulder. What finding increases his risk of recurrence?
Explanation
Little League shoulder is a physeal injury increasingly seen in young throwers. The primary treatment is refraining from throwing with rehabilitation, followed by a throwing program. The risk of recurrence is approximately 7%. The risk of recurrence is three times higher in athletes with glenohumeral internal rotation deficit. Hyperlaxity,
rotator cuff weakness, and increased height have not been shown to correlate with recurrent symptoms.
rotator cuff weakness, and increased height have not been shown to correlate with recurrent symptoms.
Question 35High Yield
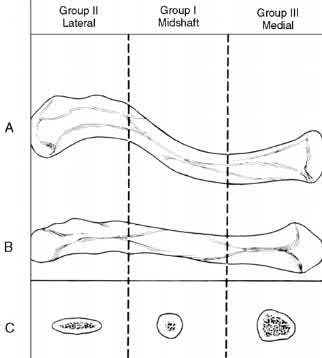
A 22-year-old healthy left hand dominant male presents to the ED with left shoulder pain after falling from an ATV. Figure A is the radiograph of his left clavicle. He is neurovascularly intact and there is no evidence of skin tenting or open fracture. Which of the following most predisposes this patient to nonunion?

Explanation
Displaced clavicle fractures are associated with higher rates of nonunion.
Nonunion occurs in roughly 5-6% of clavicle fractures and can result in slower functional return, poor cosmesis and muscle fatigability. Clavicle fractures can be sub-classified using the Allman classification into medial, diaphyseal, and lateral injuries (Illustration A). The Neer classification for diaphyseal injuries describes fractures as "nondisplaced" (less than 100% displacement) and "displaced" (greater than 100% displacement).
Robinson et al. performed a prospective cohort study to identify risk factors for nonunion after nonoperative management of clavicle fractures. The overall nonunion rate was 6.2% and was highest in lateral third fractures (11.5%).
Diaphyseal fractures had the lowest nonunion rate (4.5%). Additionally, the authors found that the risk for nonunion was increased by advancing age, female gender, fracture displacement, and comminution.
Jorgensen et al. performed a systemic review of the literature looking for predictors of non-union and malunion in mid shaft clavicle fractures treated non-operatively. They found fracture comminution, displacement, older age, female gender, and the presence of smoking to be his factors for non-union. Of these, displacement was the most likely factor that can be used to predict nonunion.
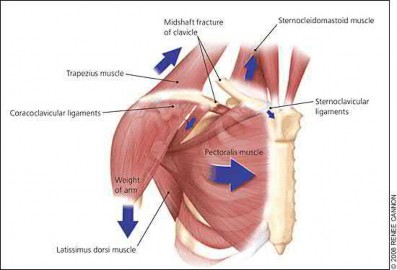
Figure A demonstrates a displaced left clavicle diaphyseal fracture. Note that the medial fragment is displaced superiorly by the deforming force of the sternocleidomastoid. Illustration A represents the Allman classification.
Illustration B demonstrates the deforming forces acting on the clavicle.
Incorrect Answers:
Answer 1: Diaphyseal fractures were demonstrated to have the lowest rate of nonunion when compared to lateral third fractures and medial clavicle fractures.
Answer 3: Advancing age was found to be an independent predictor of nonunion.
Answer 4: Female gender was found to be an independent predictor of nonunion.
Answer 5: Injury to the dominant hand was not found to be associated with an increased risk of non-union.
Nonunion occurs in roughly 5-6% of clavicle fractures and can result in slower functional return, poor cosmesis and muscle fatigability. Clavicle fractures can be sub-classified using the Allman classification into medial, diaphyseal, and lateral injuries (Illustration A). The Neer classification for diaphyseal injuries describes fractures as "nondisplaced" (less than 100% displacement) and "displaced" (greater than 100% displacement).
Robinson et al. performed a prospective cohort study to identify risk factors for nonunion after nonoperative management of clavicle fractures. The overall nonunion rate was 6.2% and was highest in lateral third fractures (11.5%).
Diaphyseal fractures had the lowest nonunion rate (4.5%). Additionally, the authors found that the risk for nonunion was increased by advancing age, female gender, fracture displacement, and comminution.
Jorgensen et al. performed a systemic review of the literature looking for predictors of non-union and malunion in mid shaft clavicle fractures treated non-operatively. They found fracture comminution, displacement, older age, female gender, and the presence of smoking to be his factors for non-union. Of these, displacement was the most likely factor that can be used to predict nonunion.
Figure A demonstrates a displaced left clavicle diaphyseal fracture. Note that the medial fragment is displaced superiorly by the deforming force of the sternocleidomastoid. Illustration A represents the Allman classification.
Illustration B demonstrates the deforming forces acting on the clavicle.
Incorrect Answers:
Answer 1: Diaphyseal fractures were demonstrated to have the lowest rate of nonunion when compared to lateral third fractures and medial clavicle fractures.
Answer 3: Advancing age was found to be an independent predictor of nonunion.
Answer 4: Female gender was found to be an independent predictor of nonunion.
Answer 5: Injury to the dominant hand was not found to be associated with an increased risk of non-union.
Question 36High Yield
Which structure is the primary stabilizer of the lesser metatarsophalangeal (MTP) joint?


Explanation
Synovitis of the second MTP occurs in association with instability of the joint. This can be idiopathic or secondary to an external deforming force (such as a hallux valgus or shoe wear causing a claw toe). The primary stabilizer of the MTP joint for translation in the vertical plane is the plantar plate. The flexor digitorum brevis flexes the MTP joint, and the flexor digitorum longus flexes
all joints of the toe. The collateral ligaments are primary stabilizers in the transverse plane and secondary stabilizers in the sagittal plane.
RECOMMENDED READINGS
[Deland JT, Sung IH. The medial crosssover toe: a cadaveric dissection. Foot Ankle Int. 2000 May;21(5):375-8. PubMed PMID: 10830654.](http://www.ncbi.nlm.nih.gov/pubmed/%2010830654)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2010830654)
[Suero EM, Meyers KN, Bohne WH. Stability of the metatarsophalangeal joint of the lesser toes: a cadaveric study. J Orthop Res. 2012 Dec;30(12):1995-8. doi: 10.1002/jor.22173. Epub 2012 Jun 13. PubMed PMID: 22696467. ](http://www.ncbi.nlm.nih.gov/pubmed/22696467)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22696467)
CLINICAL SITUATION FOR QUESTIONS 91 THROUGH 95
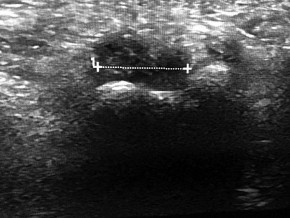
Figure 91a is the sagittal plane ultrasound of the second web space of a 48-year-old woman who has noted burning pain in the ball of her right foot for 2 years. The pain intermittently radiates into her second and the third toes. Figure 91b shows the surgical procedure and Figure 91c is the pathologic specimen.
A
B
C
all joints of the toe. The collateral ligaments are primary stabilizers in the transverse plane and secondary stabilizers in the sagittal plane.
RECOMMENDED READINGS
[Deland JT, Sung IH. The medial crosssover toe: a cadaveric dissection. Foot Ankle Int. 2000 May;21(5):375-8. PubMed PMID: 10830654.](http://www.ncbi.nlm.nih.gov/pubmed/%2010830654)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2010830654)
[Suero EM, Meyers KN, Bohne WH. Stability of the metatarsophalangeal joint of the lesser toes: a cadaveric study. J Orthop Res. 2012 Dec;30(12):1995-8. doi: 10.1002/jor.22173. Epub 2012 Jun 13. PubMed PMID: 22696467. ](http://www.ncbi.nlm.nih.gov/pubmed/22696467)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22696467)
CLINICAL SITUATION FOR QUESTIONS 91 THROUGH 95
Figure 91a is the sagittal plane ultrasound of the second web space of a 48-year-old woman who has noted burning pain in the ball of her right foot for 2 years. The pain intermittently radiates into her second and the third toes. Figure 91b shows the surgical procedure and Figure 91c is the pathologic specimen.
A
B
C
Question 37High Yield
A 24-year-old runner who underwent an allograft reconstruction of the anterior cruciate ligament (ACL) 3 years ago now reports anterior knee pain. Examination reveals no swelling or effusion, and the patient has full motion. A Lachman test and a pivot-shift test are negative. Palpation reveals tenderness on the patellar tendon and at the inferior pole of the patella. AP and lateral radiographs are shown in Figures 41a and 41b. Management should consist of**
Explanation
The radiographs show tunnel enlargement, which is seen after ACL reconstruction, particularly with allografts. Occasionally, there will be formation of an associated subcutaneous pretibial cyst. It has been proposed that the tunnel enlargement and cyst are the result of incomplete incorporation of allograft tissues within the bone tunnels. There may be residual graft necrosis, allowing synovial fluid to be transmitted through the tunnel to collect in the pretibial area, manifesting as a synovial cyst. In the absence of cyst formation, the presence of tunnel enlargement does not appear to adversely affect the clinical outcome. Based on studies by Fahey and associates, continued tunnel expansion does not occur. Victoroff and associates report good results with curettage and bone grafting of the tibial tunnel if a pretibial cyst is present. Because this patient does not have a pretibial cyst, observation with activity modification is the preferred treatment.
REFERENCES: Fahey M, Indelicato PA: Bone tunnel enlargement after anterior cruciate ligament replacement. Am J Sports Med 1994;22:410-414.
Victoroff BN, Paulos L, Beck C, Goodfellow DB: Subcutaneous pretibial cyst formation associated with anterior cruciate ligament allografts: A report of four cases and literature review. Arthroscopy 1995;11:486-494.
REFERENCES: Fahey M, Indelicato PA: Bone tunnel enlargement after anterior cruciate ligament replacement. Am J Sports Med 1994;22:410-414.
Victoroff BN, Paulos L, Beck C, Goodfellow DB: Subcutaneous pretibial cyst formation associated with anterior cruciate ligament allografts: A report of four cases and literature review. Arthroscopy 1995;11:486-494.
Question 38High Yield
A 17-year-old high school football player sustains a neck injury in a game. During the initial on-field
assessment, the team physician removes the player’s helmet, and the athlete is log-rolled to the supine position while the physician manually stabilizes his cervical spine. An examination demonstrates tenderness to palpation over the cervical spine and neurologic deficits in bilateral upper and lower extremities. Shoulder pads prohibit proper placement of a hard cervical collar, and the athlete is immobilized on a spine board and transported to the emergency department via ambulance. Comprehensive evaluation in the emergency department reveals a bilateral facet dislocation of C5 on C6. The on-field intervention most likely to cause a neurologic injury is
assessment, the team physician removes the player’s helmet, and the athlete is log-rolled to the supine position while the physician manually stabilizes his cervical spine. An examination demonstrates tenderness to palpation over the cervical spine and neurologic deficits in bilateral upper and lower extremities. Shoulder pads prohibit proper placement of a hard cervical collar, and the athlete is immobilized on a spine board and transported to the emergency department via ambulance. Comprehensive evaluation in the emergency department reveals a bilateral facet dislocation of C5 on C6. The on-field intervention most likely to cause a neurologic injury is
Explanation
Complete immobilization of the cervical spine is critical for athletes with a suspected cervical spine or spinal cord injury. The spinal cord in the subaxial spine is especially sensitive to motion, and removal of protective gear such as the helmet and shoulder pads presents an unacceptable risk for progressive neurologic injury in the setting of a potentially unstable cervical spine injury. Removal of the face mask alone is typically performed to improve access to an athlete's airway. Protective equipment often prevents
proper placement of a hard cervical collar, and the spine board offers a variety of options for safe cervical spine immobilization of helmeted athletes without a hard cervical collar. The log-roll and lift-and-slide techniques allow for the safe transfer of an athlete to a spine board while maintaining appropriate manual stabilization of the cervical spine.
proper placement of a hard cervical collar, and the spine board offers a variety of options for safe cervical spine immobilization of helmeted athletes without a hard cervical collar. The log-roll and lift-and-slide techniques allow for the safe transfer of an athlete to a spine board while maintaining appropriate manual stabilization of the cervical spine.
Question 39High Yield
A 6-year-old boy had a 4-day history of worsening atraumatic right thigh and knee pain. He was seen in the emergency department, where he had a temperature of 39.1°C. Laboratory studies reveal a white blood cell count of 15000 /µL (reference range, 4500-11000 /µL). He had a small knee effusion with range of motion 0 to 90 degrees and a swollen, painful, hot distal thigh. The knee effusion was aspirated, revealing a white blood cell (WBC) count of 2000 with negative gram stain (reference range < 2000 WBC/mL). The boy was admitted to the pediatric medical service and intravenous (IV) antibiotics were initiated. The next day, MR
imaging was obtained and orthopaedics was consulted. Based on Figures 8a and 8b, what is the most appropriate description of his condition?
imaging was obtained and orthopaedics was consulted. Based on Figures 8a and 8b, what is the most appropriate description of his condition?


Explanation
The MRI scans show an advanced distal femur osteomyelitis with a substantial subperiosteal abscess. This necessitates open drainage; by definition, an abscess is avascular, so antibiotics cannot be delivered to the area without drainage.
Figure 9a
Figure 9b
---|---
CLINICAL SITUATION FOR QUESTIONS 9 THROUGH 12
Figures 9a and 9b are the radiographs of a 9-year-old boy who fell from the monkey bars and sustained a closed fracture of the elbow.
Figure 9a
Figure 9b
---|---
CLINICAL SITUATION FOR QUESTIONS 9 THROUGH 12
Figures 9a and 9b are the radiographs of a 9-year-old boy who fell from the monkey bars and sustained a closed fracture of the elbow.
Question 40High Yield
Which of the following is most commonly associated with the use of bisphosphonates in the setting of
metastatic breast cancer?
metastatic breast cancer?
Explanation
Bisphosphonate therapy in breast cancer patients is indicated for the correction of hypercalcemia and the prevention of cancer treatment-induced bone loss. Bisphosphonates reduce metastatic bone pain in at least 50% of patients and can reduce the frequency of skeletal-related events by 30% to 40%. Osteonecrosis of the jaw could occur in up to 2.5% of breast cancer patients during longterm bisphosphonate therapy.
Question 41High Yield
Figure 1 is the radiograph of a 54-year-old man who has increasing weakness and numbness in his lateral arm. No prior surgery or injury is reported. What is the most appropriate next diagnostic test?
Explanation
22
The radiograph reveals a Charcot neuropathic shoulder. The atraumatic destruction of the humeral head is concerning for a neuropathic etiology and warrants MR imaging of the cervical spine to evaluate for the presence of a syrinx. Shoulder arthroplasty in the setting of a neuropathic joint is challenging given the local bone and soft-tissue loss, in addition to the loss of protective sensation. The scant literature on the use of shoulder arthroplasty in these challenging patients reports an improvement in pain but only modest improvements in shoulder function.
The radiograph reveals a Charcot neuropathic shoulder. The atraumatic destruction of the humeral head is concerning for a neuropathic etiology and warrants MR imaging of the cervical spine to evaluate for the presence of a syrinx. Shoulder arthroplasty in the setting of a neuropathic joint is challenging given the local bone and soft-tissue loss, in addition to the loss of protective sensation. The scant literature on the use of shoulder arthroplasty in these challenging patients reports an improvement in pain but only modest improvements in shoulder function.
Question 42High Yield
The humeral nonunion shown in Figure 27 is most likely to unite when using what method of treatment?
Explanation
The radiograph shows an atrophic nonunion of the humeral shaft. The management of humeral nonunions has been studied with compression plates and bone graft, as well as intramedullary nailing and bone graft. Compression plating with bone graft results in the highest rate of union. Compression plating by itself is not adequate, given the bone loss and lack of callous in this nonunion. Pulsed electromagnetic fields is a viable option for hypertrophic nonunions where there is inherent stability. Intramedullary nailing does not provide as much compression and stability as that achieved with compression plating.
REFERENCES: Pugh DM, McKee MD: Advances in the management of humeral nonunion.
J Am Acad Orthop Surg 2003;11:48-59.
McKee MD, Miranda MA, Riemer BL, et al: Management of humeral nonunion after the failure of locking intramedullary nails. J Orthop Trauma 1996;10:492-499.
REFERENCES: Pugh DM, McKee MD: Advances in the management of humeral nonunion.
J Am Acad Orthop Surg 2003;11:48-59.
McKee MD, Miranda MA, Riemer BL, et al: Management of humeral nonunion after the failure of locking intramedullary nails. J Orthop Trauma 1996;10:492-499.
Question 43High Yield
In rotator cuff tear arthropathy with pseudoparalysis, forward elevation of the humerus away from the body is prohibited because of
Explanation
The rotator cuff serves as a humeral head compressor that stabilizes the humeral head in the glenoid concavity, so that the deltoid can convert a vertical force into abduction and forward elevation. The deltoid functions normally in patients with chronic rotator cuff arthropathy, so no atony is present. Glenoid concavity can be lost over time as joint degeneration progresses, but this is not the primary mechanism for failure of elevation. The biceps tendon does not serve as a humeral head compressor and does not prevent proximal migration of the shoulder when it is present.
Question 44High Yield
A 72-year-old woman is scheduled to undergo right total hip arthroplasty. Her preoperative radiograph is shown in Figure
Explanation
The management of patients with proximal femoral deformity can be difficult. Appropriate implant selection and preoperative templating are critical. In this patient, it would be difficult to avoid increasing the combined offset by too much, which could contribute to the overtensioning of the soft tissues and trochanteric pain. By medializing the acetabular component (decreasing the combined offset), using a low offset femoral component or a cemented component placed more valgus (decreasing the combined offset), and making a longer neck cut (to avoid shortening of the lower extremity), restoration of the patient’s native offset and leg length can be achieved.
Question 45High Yield
C haracteristic histological features of malignant schwannoma are best described as:
Explanation
The histological features of malignant schwannoma have characteristic fusiform cells with neoplastic schwann cells and nerve fascicles.
Question 46High Yield
An 83-year-old man with a history of diabetes mellitus reports abdominal pain on postoperative day number three following a total hip arthroplasty. The patient reports having a bowel movement the prior evening. Examination reveals that the abdomen is distended but nontender. What is the next step in management?
Explanation
DISCUSSION: The patient has risk factors, symptoms, and signs of Ogilvie syndrome of acute colonic pseudo- obstruction. This unusual but potentially catastrophic complication is characterized by functional colonic obstruction without an associated mechanical blockage. This disorder has been associated with advanced age, male gender, the use of narcotic pain medications, and patients who have undergone hip arthroplasty. The first step in management of any complication is diagnosis, and the diagnosis is most rapidly made using radiographs that show dilation of the large intestine.
REFERENCES: Nelson JD, Urban JA, Salsbury TL, et al: Acute colonic pseudo-obstruction (Ogilvie syndrome) after arthroplasty in the lower extremity. J Bone Joint Surg Am 2006;88:604-610.
Clarke HD, Berry DJ, Larson DR: Acute pseudo-obstruction of the colon as a postoperative complication of hip
arthroplasty. J Bone Joint Surg Am 1997;79:1642-1647.
REFERENCES: Nelson JD, Urban JA, Salsbury TL, et al: Acute colonic pseudo-obstruction (Ogilvie syndrome) after arthroplasty in the lower extremity. J Bone Joint Surg Am 2006;88:604-610.
Clarke HD, Berry DJ, Larson DR: Acute pseudo-obstruction of the colon as a postoperative complication of hip
arthroplasty. J Bone Joint Surg Am 1997;79:1642-1647.
Question 47High Yield
..A 40-year-old right-hand-dominant construction worker has a 3-month history of right shoulder weakness secondary to a fall from a ladder at work. He underwent nonsurgical treatment with anti-inflammatory medication, cortisone injections, and therapy, with minimal relief of his symptoms. A subsequent MRI scan indicates a 1-cm full-thickness supraspinatus tendon tear. He has been referred to your clinic for discussion of surgical intervention. The patient's nurse case manager is concerned that he may not be able to return to his preinjury level of activity at work, even with surgical intervention. You tell the nurse case manager that, on average, the patient will
Explanation
- have significant functional improvement after rotator cuff repair that is less robust than that of patients without a Worker’s Compensation claim.
Question 48High Yield
Organisms survive on biosynthetiCsurfaces, such as total hips, because of:
Explanation
AntibiotiCresistance, the organismâs ability to form a glycocalyx or polysaccharide biofilm, and a slime layer enable the organism to survive on implants. This is one of the reasons why it is difficult to clear up an infection using only antibiotics
Question 49High Yield
A 9-year-old girl, who is an avid soccer player, has intermittent spontaneous snapping in her left knee that has worsened. There is no reported trauma or prior surgeries to her knee. Despite working with her trainer, she has developed anterior-based knee pain and lacks full extension. Her knee skin is unremarkable, but there is fullness to palpation on the lateral aspect of her knee. Her range of motion demonstrates a lack of 15° of terminal extension and ligamentous examination is unremarkable. Considering possible surgical treatments for this patient, what is the most appropriate surgical treatment?
Explanation
Surgical intervention of discoid meniscus is based on symptomatic patients. Complete discoid menisci are typically stable but are expected to have >4.5 times incidence of surgical intervention. Saucerization of symptomatic discoid meniscus is associated with better results with younger patients with increases of poor outcomes in adult-aged patients. Meniscal transplant may be an option, although long-term results _are unknown._
Question 50High Yield
A 20-year-old man has middle finger metacarpophalangeal (MP) joint pain with difficulty extending his MP joint. The skin is not injured, yet the digit seems to be slightly ulnar deviated. He can maintain extension but has difficulty extending his MP joint from full MP joint flexion. If surgery is recommended, which structure most likely needs to be repaired to restore active motion?
Explanation
This is an example of a closed sagittal band MP joint injury. The radial sagittal band ruptures , and the extensor tendon subluxes ulnarly . When the MP joint is flexed, it is difficult to fully extend it, but when the MP joint is held in full extension, active extension can maintain the position. In the setting of an extensor digitorum injury, extension cannot be maintained even if the MP joint is positioned in extension. The joint capsule is often injured when the sagittal band is injured, but repairing it will not restore extension. The radial collateral ligament of the MP joint is rarely injured with a sagittal band injury, and repairing it would not restore MP joint extension. When the MP joint is fully extended if the extensor tendon centralizes and full MP joint extension can be maintained, this injury usually is treated with a splint [yoke splint]) for 6 to 8 weeks. Surgery is recommended if the extensor tendon does not centralize with passive extension or if an injury is chronic. Surgery often is recommended for high-level athletes.
RECOMMENDED READINGS
16. Kleinhenz BP, Adams BD. Closed Sagittal Band Injury of the Metacarpophalangeal Joint. J Am Acad Orthop Surg. 2015 Jul;23(7):415-23. doi: 10.5435/JAAOS-D-13-00203. Review. PubMed PMID:
[26111875/. ](http://www.ncbi.nlm.nih.gov/pubmed/26111875)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26111875)
17. [Catalano LW 3rd, Gupta S, Ragland R 3rd, Glickel SZ, Johnson C, Barron OA. Closed treatment of nonrheumatoid extensor tendon dislocations at the metacarpophalangeal joint. J Hand Surg Am. 2006 Feb;31(2):242-5. PubMed PMID: 16473685. ](http://www.ncbi.nlm.nih.gov/pubmed/16473685)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16473685)
18. [Lin JD, Strauch RJ. Closed soft tissue extensor mechanism injuries (mallet, boutonniere, and sagittal band). J Hand Surg Am. 2014 May;39(5):1005-11. doi: 10.1016/j.jhsa.2013.11.018. Review. PubMed PMID: 24766832. ](http://www.ncbi.nlm.nih.gov/pubmed/24766832)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24766832)
RECOMMENDED READINGS
16. Kleinhenz BP, Adams BD. Closed Sagittal Band Injury of the Metacarpophalangeal Joint. J Am Acad Orthop Surg. 2015 Jul;23(7):415-23. doi: 10.5435/JAAOS-D-13-00203. Review. PubMed PMID:
[26111875/. ](http://www.ncbi.nlm.nih.gov/pubmed/26111875)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26111875)
17. [Catalano LW 3rd, Gupta S, Ragland R 3rd, Glickel SZ, Johnson C, Barron OA. Closed treatment of nonrheumatoid extensor tendon dislocations at the metacarpophalangeal joint. J Hand Surg Am. 2006 Feb;31(2):242-5. PubMed PMID: 16473685. ](http://www.ncbi.nlm.nih.gov/pubmed/16473685)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16473685)
18. [Lin JD, Strauch RJ. Closed soft tissue extensor mechanism injuries (mallet, boutonniere, and sagittal band). J Hand Surg Am. 2014 May;39(5):1005-11. doi: 10.1016/j.jhsa.2013.11.018. Review. PubMed PMID: 24766832. ](http://www.ncbi.nlm.nih.gov/pubmed/24766832)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24766832)
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon