Soft Tissue Procedures for Hallux Valgus: The Modified McBride Technique
Key Takeaway
The modified McBride procedure is a foundational soft tissue correction for mild to moderate hallux valgus. Ideal candidates are patients with a hallux valgus angle of 15 to 25 degrees, an intermetatarsal angle under 13 degrees, and no degenerative joint changes. This guide details the biomechanical principles, precise surgical steps, and postoperative protocols required to achieve optimal outcomes while minimizing risks such as iatrogenic hallux varus.
INTRODUCTION TO SOFT TISSUE PROCEDURES IN HALLUX VALGUS
The surgical management of the hallux valgus complex requires a profound understanding of first ray biomechanics, soft tissue balancing, and osseous alignment. While modern algorithmic approaches frequently favor osseous osteotomies for moderate to severe deformities, isolated soft tissue procedures remain a critical component of the orthopedic surgeon’s armamentarium when applied to meticulously selected patients.
The modified McBride procedure represents the gold standard of soft tissue correction for hallux valgus. Historically, this technique is a sophisticated amalgamation of foundational concepts. It combines the medial eminence resection and capsulorrhaphy described by Silver in 1923 with the lateral soft tissue release introduced by McBride in 1928. The procedure was subsequently refined by DuVries and widely popularized by Mann. When executed correctly in the appropriate demographic, the modified McBride procedure yields highly successful, reproducible outcomes.
PATIENT SELECTION AND INDICATIONS
The success of any soft tissue procedure for hallux valgus is entirely predicated on strict adherence to preoperative indications. Soft tissue balancing alone cannot overcome severe osseous malalignment or structural instability.
The quintessential candidate for a modified McBride procedure is a 30- to 50-year-old woman presenting with clinical symptoms (pain over the medial eminence, difficulty with footwear) and a history of conservative management failure (e.g., shoe modification, orthotics).
Strict Radiographic and Clinical Criteria:
* Hallux Valgus Angle (HVA): 15 to 25 degrees.
* Intermetatarsal Angle (IMA): Less than 13 degrees.
* Hallux Valgus Interphalangeus (HVIP): Less than 15 degrees.
* Joint Status: Absolutely no degenerative arthritic changes at the first metatarsophalangeal (MTP) joint.
* Joint Congruency: The articular surface of the metatarsal head must be appropriately positioned relative to the longitudinal axis of the first metatarsal (normal Proximal Articular Set Angle - PASA).

Surgical Warning: Performing a modified McBride procedure on a patient with an IMA greater than 13 degrees or significant first tarsometatarsal (TMT) hypermobility will almost universally result in deformity recurrence. In such cases, a proximal or distal metatarsal osteotomy is mandatory.
COMPREHENSIVE PREOPERATIVE EVALUATION
Clinical Assessment
Before bunion surgery is even considered, the patient's baseline physiological status must be thoroughly investigated. Inadequate vascularity or diminished sensibility (e.g., diabetic peripheral neuropathy) are absolute contraindications to elective soft tissue reconstruction of the forefoot.
The clinical examination must systematically evaluate the following ten biomechanical and anatomical factors:
1. Overall alignment and weight-bearing footprint.
2. Presence of Achilles or gastrocnemius contracture.
3. Pronation of the hallux, the first metatarsal, or both.
4. Presence of hallux valgus interphalangeus.
5. Arthritis and any limitation of motion at the first MTP joint.
6. Length of the first metatarsal relative to the lesser metatarsals (to avoid iatrogenic transfer metatarsalgia).
7. Excessive mobility or obliquity of the first metatarsomedial cuneiform (TMT) joint.
8. The size and morphology of the medial eminence (bunion).
9. The location and subluxation of the sesamoid apparatus.
10. Intrinsic and extrinsic muscle-tendon balance and synchrony.
Radiographic Evaluation
Standard preoperative imaging must include weight-bearing (standing) dorsoplantar and lateral views, a nonstanding lateral oblique view, and axial sesamoid views.

The HVA and the first-second IMA should be drawn on the standing dorsoplantar view by bisecting the shafts of the respective bones. The surgeon must maintain an acute awareness of normal anatomical ranges and measurement tolerances.

Clinical Pearl: Measurement Variability
While the HVA and IMA are the most frequently cited guidelines for treatment decisions, Donnelly et al. reported significant interobserver variability. Measurements of the HVA can vary by approximately 6 degrees, and the IMA by 4 degrees between observers. Potential errors in measurement must be factored into the surgical decision-making process. Do not rely solely on a single degree of measurement to dictate the surgical algorithm.
Dynamic Stress Views and TMT Stability
Stress view radiographs are an invaluable adjunct in determining whether a patient can be successfully treated with an isolated modified McBride procedure.
The surgeon should evaluate the medial side of the metatarsocuneiform joint on stress views. "Booking open" of this joint indicates incongruous motion, lateral impingement, loss of bony support, and a medial capsule that is acting as a spring on stretch. Osteotomy or arthrodesis (Lapidus procedure) is strictly indicated in patients demonstrating this medial wedged opening of the TMT joint.
Conversely, if a firm forefoot wrap congruously reduces the IMA to a normal value and decreases the HVA—rotating the base of the first metatarsal on the medial cuneiform without levering the joint open medially—the McBride procedure is biomechanically capable of correcting the deformity.
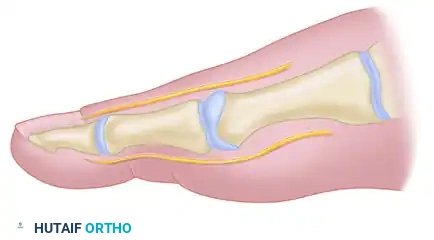
BIOMECHANICS OF THE SESAMOID APPARATUS
A core component of the modified McBride procedure is the lateral release, which addresses the deforming forces acting on the first MTP joint. In a hallux valgus deformity, the metatarsal head drifts medially, slipping off the sesamoid apparatus. The sesamoids, tethered by the transverse metatarsal ligament, remain in their anatomical position relative to the second metatarsal, appearing radiographically as though they have subluxated laterally.
Correction is significantly improved by the release of the adductor hallucis and the lateral head of the flexor hallucis brevis (FHB). In severe, non-reducible cases, excision of the fibular (lateral) sesamoid may be considered.
Biomechanical advantages of fibular sesamoidectomy:
* Releases the adductor hallucis and lateral head of the FHB, markedly reducing the valgus moment at the first MTP joint.
* Prevents the pull of the fibular sesamoid on the flexor hallucis longus (FHL) through its tendon sheath and pulley system, neutralizing another potent valgus-producing force.
Pitfall: Iatrogenic Hallux Varus
Excision of the fibular sesamoid carries a high risk of overcorrection, leading to a disastrous iatrogenic hallux varus. If the fibular sesamoid is excised, the medial capsule must be repaired with the hallux held in 5 to 10 degrees of valgus. This position must be rigidly maintained by a postoperative dressing for 3 to 4 weeks until capsular healing is complete. Modern practice generally favors a thorough lateral soft tissue release without sesamoidectomy whenever possible.
SURGICAL TECHNIQUE: THE MODIFIED MCBRIDE PROCEDURE
1. Anesthesia and Positioning
The procedure is typically performed under regional anesthesia (ankle block or popliteal block) with intravenous sedation. The patient is placed supine on the operating table. A calf or thigh tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying the delicate neurovascular structures and the internervous planes.
2. Incision and Exposure
A dorsomedial or direct medial incision is utilized. The direct medial incision is often preferred as it lies in an internervous plane, minimizing the risk of injury to the dorsal cutaneous nerves.

The incision extends from the mid-shaft of the first metatarsal to the mid-shaft of the proximal phalanx. Careful blunt dissection is carried out through the subcutaneous tissues. The dorsal and plantar medial cutaneous nerves must be identified and gently retracted.
3. Medial Capsulotomy
The medial capsule of the first MTP joint is exposed. A longitudinal capsular incision is made. It is critical to place this incision slightly plantar to the midline of the joint to ensure adequate tissue remains dorsally for the subsequent capsulorrhaphy.
The capsule is carefully elevated off the medial eminence via sharp dissection. The proximal attachment of the capsule on the metatarsal neck must be meticulously preserved to maintain the vascular supply to the capsular flaps and ensure a robust repair during closure.
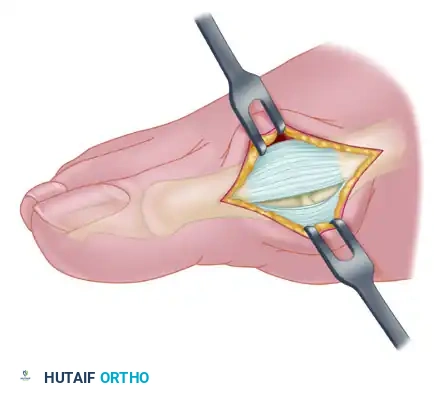
4. Medial Eminence Resection (Exostectomy)
With the capsule reflected, the medial eminence is fully visualized. The sagittal groove, which demarcates the medial extent of the functional articular cartilage, is identified.
Using an oscillating saw, the medial eminence is resected. The cut should be made in line with the medial border of the first metatarsal shaft, starting at the sagittal groove and exiting proximally at the metatarsal neck.
* Crucial Step: Avoid excessive resection. Removing too much of the metatarsal head compromises the medial articular support, leading to medial subluxation of the proximal phalanx and subsequent hallux varus.
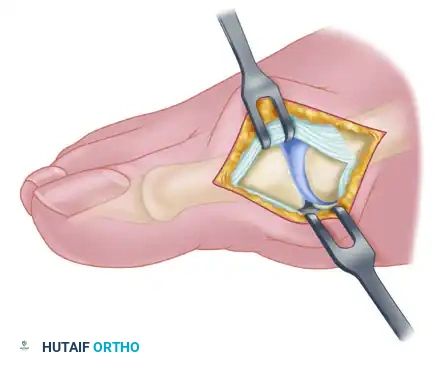
5. The Lateral Release
The lateral release is the most technically demanding portion of the modified McBride procedure. It can be performed transarticularly (through the MTP joint) or via a separate dorsal incision in the first web space.
Steps of the Lateral Release:
1. Release of the Suspensory Ligament: The lateral sesamoid suspensory ligament is incised, allowing the sesamoid apparatus to mobilize medially.
2. Release of the Deep Transverse Metatarsal Ligament: This ligament, connecting the first and second metatarsal heads, is sharply divided. Care must be taken to protect the underlying neurovascular bundle.
3. Adductor Hallucis Tenotomy: The conjoined tendon of the adductor hallucis is identified at its insertion on the base of the proximal phalanx and the lateral sesamoid. It is sharply detached.
4. Lateral Capsulotomy: If the joint remains tight, a vertical lateral capsulotomy is performed.
Following the lateral release, the surgeon should be able to manually reduce the hallux into a neutral or slightly varus position without resistance. The sesamoids should reduce anatomically beneath the metatarsal head.
6. Medial Capsulorrhaphy (Plication)
With the lateral deforming forces neutralized, the medial capsule is repaired to hold the toe in its corrected alignment.
The hallux is held in approximately 5 to 10 degrees of valgus and neutral dorsiflexion. The plantar and dorsal flaps of the medial capsule are advanced and imbricated (overlapped) to remove redundancy. The capsule is sutured using strong, absorbable sutures (e.g., 2-0 Vicryl) in an interrupted fashion.
Surgical Warning: Never plicate the capsule with the toe in neutral (0 degrees) or varus. The robust healing of the medial capsule will inevitably pull the toe further medially, resulting in a rigid, painful hallux varus. Always secure the repair with the toe in slight, physiological valgus.
7. Closure
Once the capsulorrhaphy is complete and the alignment is deemed satisfactory, the subcutaneous tissues are closed with 3-0 absorbable sutures. The skin is closed with non-absorbable monofilament sutures or a subcuticular stitch, depending on surgeon preference.

POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative dressing is as critical as the surgery itself. The dressing acts as an external splint, maintaining the soft tissue balance while the capsulorrhaphy heals.
- Immediate Postoperative Care: A bulky, compressive forefoot dressing is applied in the operating room. The hallux is splinted in the corrected position (5 to 10 degrees of valgus).
- Weight-Bearing: Patients are typically allowed heel-weight-bearing or flat-foot weight-bearing in a rigid postoperative shoe immediately following surgery.
- Dressing Changes: The initial dressing is maintained for 10 to 14 days, at which point sutures are removed. A new compressive wrap or a specialized bunion splint is applied.
- Immobilization Duration: The hallux must be maintained in the corrected position with taping or splinting for a total of 4 to 6 weeks to allow the medial capsule to fibrose and heal securely.
- Physical Therapy: Active and passive range of motion exercises for the MTP joint are initiated at 3 to 4 weeks to prevent joint stiffness. Return to normal footwear and high-impact activities is generally permitted at 8 to 12 weeks, depending on the resolution of edema.
COMPLICATIONS AND PITFALLS
While highly effective, the modified McBride procedure is not without risks. Meticulous surgical technique and strict patient selection are the primary defenses against complications.
- Hallux Varus: The most dreaded complication. Caused by excessive medial eminence resection, over-plication of the medial capsule, or aggressive lateral release (especially fibular sesamoidectomy). Treatment often requires soft tissue reconstruction (e.g., EHB tendon transfer) or MTP joint arthrodesis.
- Recurrence of Deformity: Typically occurs if the procedure is performed on a patient with an IMA > 13 degrees, unrecognized TMT hypermobility, or if the lateral release was inadequate.
- Avascular Necrosis (AVN) of the Metatarsal Head: Rare in isolated soft tissue procedures but can occur if the capsular stripping is overly aggressive, destroying the vascular plexus supplying the metatarsal head. Always preserve the proximal capsular attachments.
- Joint Stiffness: Prevented by precise capsular repair tensioning and early, controlled range of motion exercises.
CONCLUSION
The modified McBride procedure remains a cornerstone technique in operative orthopedics for the correction of mild to moderate hallux valgus. By respecting the intricate biomechanics of the first ray, performing a precise internervous approach, executing a thorough lateral release, and meticulously balancing the medial capsule, the orthopedic surgeon can achieve durable, pain-free, and functionally excellent outcomes for their patients. Strict adherence to radiographic parameters and dynamic clinical assessments ensures that this powerful soft tissue technique is utilized only in the appropriate clinical scenario, safeguarding against recurrence and overcorrection.
You Might Also Like

