Masterclass in Plantar Fascia and Nerve Release: Open and Endoscopic Techniques
Key Takeaway
Plantar fasciotomy and Baxter’s nerve release are definitive surgical interventions for recalcitrant plantar fasciitis and compressive neuropathy of the first branch of the lateral plantar nerve. This guide details both open and endoscopic techniques, emphasizing precise anatomical dissection, targeted fascial release, and meticulous nerve decompression. Proper patient selection and adherence to biomechanical principles are paramount for achieving optimal functional outcomes and preventing lateral column destabilization.
INTRODUCTION TO PLANTAR FASCIA AND NERVE PATHOLOGY
Recalcitrant heel pain is one of the most common presentations in orthopedic foot and ankle clinics. While the vast majority of patients respond to a rigorous regimen of conservative management—including Achilles and plantar fascia specific stretching, orthoses, night splints, and corticosteroid or orthobiologic injections—approximately 5% to 10% of patients will experience chronic, debilitating pain that necessitates surgical intervention.
The underlying pathology is rarely an acute inflammatory "-itis," but rather a chronic degenerative fasciosis characterized by microtears, collagen necrosis, and angiofibroblastic hyperplasia at the origin of the medial band of the plantar fascia on the medial calcaneal tuberosity. Furthermore, chronic thickening of the plantar fascia and hypertrophy of the abductor hallucis muscle can lead to secondary compressive neuropathy of the first branch of the lateral plantar nerve, commonly known as Baxter’s nerve.
Surgical intervention must therefore address both the mechanical tension of the plantar fascia and the potential neurogenic pain generated by Baxter's nerve entrapment. This comprehensive guide details the gold-standard open release (Schon technique) and the minimally invasive endoscopic plantar fasciotomy (EPF) (Barrett technique).
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of plantar biomechanics and local neurovascular anatomy is non-negotiable for the operating surgeon.
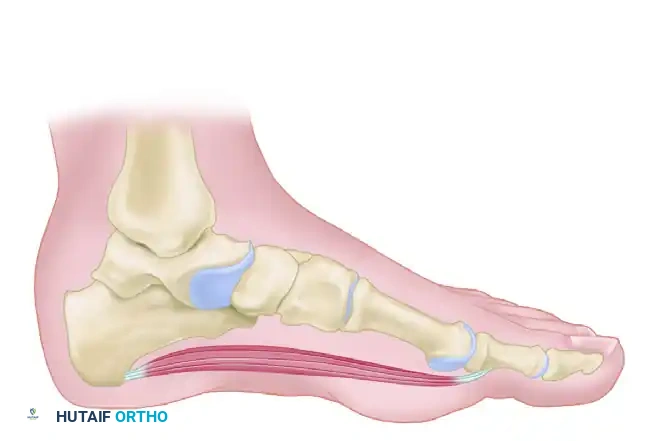
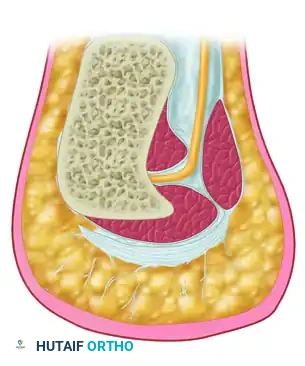
The Plantar Fascia and the Windlass Mechanism
The plantar fascia is a dense, fibrous aponeurosis divided into medial, central, and lateral bands. The central band is the thickest and most structurally significant, originating from the medial process of the calcaneal tuberosity and fanning out to insert into the base of the proximal phalanges via the plantar plates.
Biomechanically, the plantar fascia operates via the Windlass Mechanism (described by Hicks). Dorsiflexion of the metatarsophalangeal (MTP) joints during the terminal stance phase of gait winds the plantar fascia around the metatarsal heads, elevating the longitudinal arch and locking the midtarsal joints to create a rigid lever for propulsion.
Surgical Warning: Complete transection of the plantar fascia eliminates the Windlass mechanism, leading to arch collapse, midtarsal faulting, and severe lateral column overload. Surgical release must be strictly limited to the medial one-third to one-half of the fascia.
Baxter’s Nerve (First Branch of the Lateral Plantar Nerve)
Baxter’s nerve provides motor innervation to the abductor digiti minimi and sensory innervation to the calcaneal periosteum. It originates from the lateral plantar nerve and courses vertically between the deep fascia of the abductor hallucis muscle and the medial aspect of the quadratus plantae muscle.
Entrapment typically occurs at two distinct anatomical points:
1. As the nerve passes through the deep fascial leash of the abductor hallucis muscle.
2. As it passes anterior to the medial calcaneal tuberosity, where it can be compressed by a plantar calcaneal spur or a thickened plantar fascia.
PREOPERATIVE EVALUATION AND INDICATIONS
Indications for Surgery
- Failure of Conservative Treatment: A minimum of 6 to 12 months of documented, exhaustive conservative management.
- Severe Impact on Quality of Life: Pain that severely limits activities of daily living or occupational duties.
- Clinical Confirmation: Point tenderness at the medial calcaneal tubercle, positive Windlass test, and/or radiating pain along the course of Baxter's nerve (positive Tinel's sign over the abductor hallucis).
Differential Diagnosis to Exclude
- Tarsal tunnel syndrome (requires EMG/NCS for differentiation).
- Calcaneal stress fracture (requires MRI or bone scan).
- Systemic inflammatory arthropathies (e.g., Ankylosing Spondylitis, Reiter's syndrome).
- Plantar fibromatosis.
OPEN PLANTAR FASCIA AND NERVE RELEASE (SCHON TECHNIQUE)
The open technique allows for direct visualization of the plantar fascia, precise partial fasciotomy, and definitive neurolysis of Baxter's nerve. It is particularly indicated when neurogenic symptoms predominate or when a large, symptomatic calcaneal exostosis requires resection.
Patient Positioning and Anesthesia
- Anesthesia: General anesthesia, spinal anesthesia, or monitored anesthesia care (MAC) with a regional popliteal/saphenous nerve block.
- Positioning: Supine with a bump under the ipsilateral hip to externally rotate the leg, providing optimal access to the medial aspect of the heel.
- Preparation: Standard sterile prep and drape. Exsanguinate the foot with an Esmarch bandage and inflate a pneumatic thigh or calf tourniquet to 250-300 mmHg.
Step-by-Step Surgical Approach
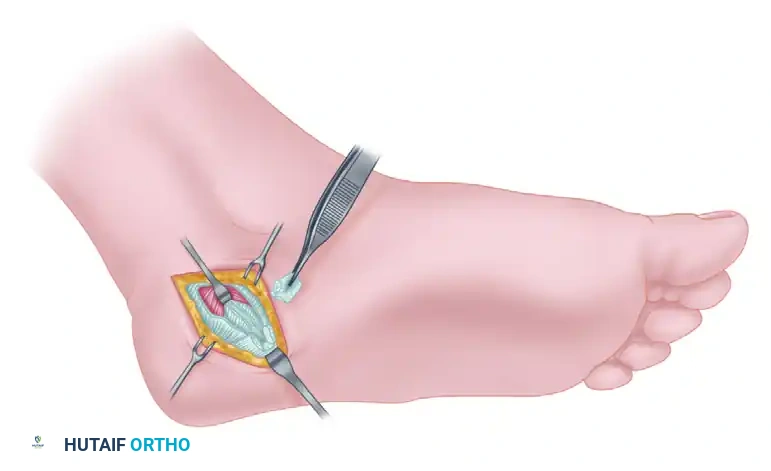
Step 1: Incision and Superficial Dissection
Make an oblique or slightly curved incision approximately 3 to 4 cm in length over the medial aspect of the heel. The incision should be centered over the anticipated course of the first branch of the lateral plantar nerve, just distal to the medial calcaneal tuberosity.
Carefully dissect through the subcutaneous fat. The heel pad is highly vascular and compartmentalized by fibrous septa; meticulous hemostasis is required.
Step 2: Release of the Superficial Fascia
Identify the superficial fascia overlying the abductor hallucis muscle. Incise this fascia longitudinally to expose the muscle belly.
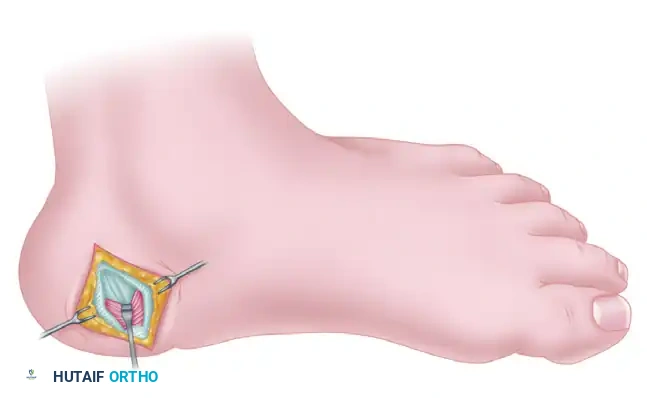
Step 3: Mobilization of the Abductor Hallucis
Using blunt dissection, free the abductor hallucis muscle from its fascial investments. Reflect the muscle belly proximally to expose the deep fascial layer.
Subsequently, retract the abductor hallucis muscle distally and plantarward. This maneuver exposes the deep fascia of the abductor hallucis and the underlying quadratus plantae muscle.
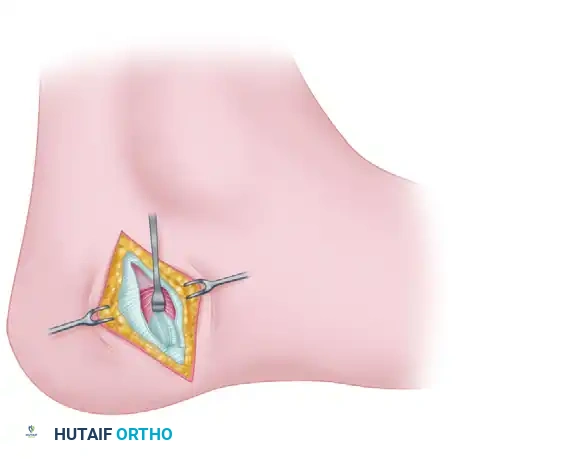
Step 4: Identification and Decompression of Baxter's Nerve
The critical step in neurolysis is the release of the deep fascia of the abductor hallucis. This fascia forms a sharp, unyielding edge that compresses the first branch of the lateral plantar nerve.
Carefully incise the deep fascia. You may visualize the nerve coursing vertically between the abductor hallucis and the quadratus plantae.
Clinical Pearl: Check the adequacy of the nerve release by placing a small, curved hemostat deep to the deep fascia of the abductor hallucis. Gently spread the tines and palpate for any remaining tight fascial bands. The instrument should pass freely without resistance.
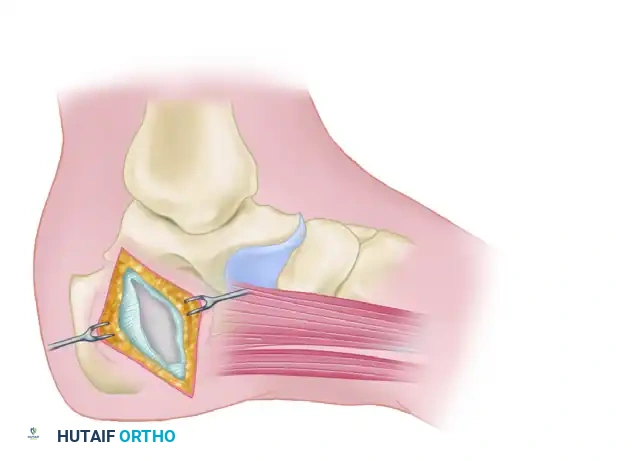
Step 5: Partial Plantar Fasciotomy
Identify the medial band of the plantar fascia at its insertion on the calcaneus. Resect a small rectangular block of the medial plantar fascia, measuring approximately 2 to 3 mm by 4 mm.
Note on Complete Fasciotomy: An entire plantar fasciotomy is rarely indicated but may be performed in select, strictly nonathletic, sedentary patients who exhibit intractable pain across the entire medial and lateral insertion. If required, insert a lamina spreader into the resected medial gap to place the remaining fascia under tension, then carefully divide the remaining fibers.
Step 6: Management of the Calcaneal Spur (Optional)
If a large, radiographically confirmed calcaneal spur is present and deemed a primary pain generator, it can be resected.
1. Gently reflect the origin of the flexor digitorum brevis off the exostosis.
2. Place a Freer elevator superior and inferior to the spur to protect surrounding soft tissues.
3. Transect the spur at its base using a 1/4-inch osteotome.
4. CRITICAL: Take extreme care not to damage Baxter's nerve, which lies immediately superior to the spur.
5. Remove the bony fragment with a rongeur and rasp the edges smooth. Apply bone wax or topical thrombin to the cancellous bone surface to prevent postoperative hematoma.
Step 7: Closure
Irrigate the wound copiously with sterile saline. Deflate the tourniquet and achieve meticulous hemostasis to prevent hematoma formation, which can lead to severe postoperative pain and delayed wound healing. Close the skin with 4-0 nylon mattress sutures.
Apply a robust compression dressing: 4 × 4-inch gauze sponges, a 4-inch Kerlix roll, a 4-inch Kling bandage, and a 4-inch elastic bandage (ACE wrap).
Open Technique Postoperative Care
- Weeks 0-2: The patient is strictly non-weight-bearing (NWB) in a posterior splint or controlled ankle motion (CAM) boot to allow soft tissue healing and prevent wound dehiscence.
- Week 2: Sutures are removed. The patient transitions to progressive weight-bearing to tolerance (WBAT) in a CAM boot.
- Weeks 3-6: Resumption of aggressive heel cord stretching. Transition to supportive athletic shoes with custom orthoses. Physical therapy focuses on intrinsic foot muscle strengthening.
ENDOSCOPIC PLANTAR FASCIOTOMY (EPF - BARRETT TECHNIQUE)
Endoscopic Plantar Fasciotomy (EPF) offers the advantage of a minimally invasive approach, resulting in less soft tissue trauma, reduced risk of painful heel scarring, and a faster return to weight-bearing. It is ideal for isolated plantar fasciitis without significant neurogenic symptoms requiring formal open neurolysis.
Equipment and Setup
The procedure utilizes specialized instrumentation, such as the Endotrac system (Instratek, Houston, TX), which includes:
* A blunt fascial elevator.
* A hook probe.
* A slotted obturator-cannula system.
* Disposable retrograde hook and triangle blades.
* A standard 4.0-mm, 30-degree arthroscope.
Step-by-Step Endoscopic Approach
Step 1: Medial Portal Placement
After administering IV sedation and a local anesthetic block (or general anesthesia), exsanguinate the foot and inflate the tourniquet.
Establish a reference point for the medial incision immediately anterior and inferior to the inferior aspect of the medial calcaneal tubercle, verified via a non-weight-bearing lateral fluoroscopic projection if necessary. Make a 5-mm vertical stab incision at this site.
Step 2: Creating the Working Channel
Bluntly dissect through the subcutaneous tissue to the level of the plantar fascia. Because direct visualization is impossible at this stage, tactile feedback is paramount.
1. Palpate the medial investment of the plantar fascia with the fascial elevator.
2. Create a transverse channel immediately inferior (plantar) to the plantar fascia using the elevator.
3. Introduce the slotted obturator-cannula system into this channel. Advance it firmly across the inferior surface of the plantar fascia toward the lateral aspect of the foot.
Step 3: Lateral Portal Placement
Palpate the tip of the advancing obturator on the lateral side of the foot. Make a corresponding 5-mm vertical incision over the tip, allowing the obturator and cannula to pass completely through the skin. Remove the obturator, leaving the slotted cannula in place spanning the width of the foot.
Step 4: Endoscopic Visualization
Introduce the 30-degree endoscope through the medial portal and the fascial probe through the lateral portal.
Visualize the entire inferior surface of the plantar fascia on the monitor. The cannula features internal reference marks:
* Double marks: Indicate the approximate location of the medial plantar fascia investment (typically 9 mm and 11 mm from the medial dermis).
* Single mark: Indicates the approximate location of the medial intermuscular septum (typically 13.5 mm from the midpoint of the first two marks).
* Note: These marks are based on cadaveric averages and must be correlated with direct visual and tactile feedback.
Step 5: Fascial Release
🔪 Surgical Technique 82-22: Endoscopic Release
While viewing the medial investment of the plantar fascia through the endoscope, use the lateral probe to palpate the taut fascial fibers.
1. Introduce the retrograde hook knife from the lateral portal to the medial anatomical reference point.
2. Engage the medial band of the plantar fascia and pull the blade laterally to sever the fibers.
3. The 180-Degree Perspective: Remove the instruments and swap portals—insert the endoscope laterally and the probe medially. This provides a reverse perspective to ensure complete release of the targeted medial band.
4. If residual tight fibers are palpated, introduce the triangle blade to carefully release them. You must visualize the underlying muscle belly (flexor digitorum brevis) through the fascial defect to confirm a full-thickness release.
Step 6: Closure
Irrigate the cannula with sterile saline to clear debris and remove the slotted cannula. Approximate the medial and lateral stab incisions with simple 5-0 Prolene or nylon sutures.
To minimize postoperative pain, infiltrate the surgical site with a mixture of 0.5% bupivacaine and 1 mL of dexamethasone. Apply a sterile compressive gauze dressing and deflate the tourniquet.
Endoscopic Technique Postoperative Care
- Immediate Post-op: Unlike the open technique, EPF patients are allowed full weight-bearing immediately after surgery as tolerated, though excessive ambulation should be avoided to prevent hematoma.
- Day 3: The bulky surgical dressings are removed, and sterile cloth adhesive bandages (e.g., Band-Aids) are applied to the portals.
- Weeks 1-4: The patient may transition into regular, supportive athletic shoes fitted with their preoperative orthotic appliances as soon as comfort allows. Physical therapy is initiated to restore normal gait mechanics.
COMPLICATIONS AND SURGICAL PITFALLS
While generally highly successful, plantar fascia release carries specific biomechanical risks that the surgeon must actively mitigate.
- Lateral Column Overload / Cuboid Syndrome: The most significant complication of over-resection. Releasing more than 50% of the plantar fascia severely compromises the longitudinal arch, shifting weight-bearing forces laterally. This can result in intractable lateral midfoot pain and cuboid stress fractures.
- Incomplete Nerve Release: Failure to adequately release the deep fascia of the abductor hallucis during the open procedure will result in persistent neurogenic heel pain.
- Plantar Nerve Injury: The medial and lateral plantar nerves, and specifically Baxter's nerve, are highly vulnerable during both open dissection and blind passage of the endoscopic cannula. The cannula must remain strictly plantar to the fascia.
- Infection and Wound Dehiscence: The heel pad has poor vascularity at the dermal level. Overly aggressive retraction or premature weight-bearing in open procedures can lead to wound breakdown.
- Painful Scarring: Hypertrophic scarring on the plantar weight-bearing surface can be as debilitating as the original fasciitis. Incisions must be placed carefully, avoiding the direct plantar weight-bearing axis.
📚 Medical References
- Plantar fascia release through a transverse plantar incision, Foot Ankle 20:364, 1999.
- Calder JD, Saxby TS: Surgical treatment of insertional Achilles tendinosis, Foot Ankle Int 24:119, 2003.
- Castro MD: Arthrodesis of the navicular, Foot Ankle Clin 9:73, 2004.
- Cavanaugh PR, Ae M: A technique for the display of pressure distributions beneath the foot, J Biomech 13:69, 1980.
- Chen HS, Chen LM, Huang TW: Treatment of
You Might Also Like
