Distal First Metatarsal Osteotomy: The Mitchell Procedure
Key Takeaway
The Mitchell osteotomy is a distal first metatarsal step-cut procedure designed to correct mild-to-moderate hallux valgus. By laterally displacing and plantarflexing the capital fragment, it reduces the intermetatarsal angle while decompressing the first metatarsophalangeal joint. Although largely superseded by modern techniques like the chevron osteotomy, mastering its biomechanical principles remains essential for orthopedic surgeons to understand deformity correction, manage complications such as transfer metatarsalgia, and execute precise capsulorrhaphy techniques.
INTRODUCTION TO DISTAL FIRST METATARSAL OSTEOTOMIES
The surgical management of hallux valgus encompasses a broad spectrum of osteotomies, soft tissue realignments, and arthrodesis techniques. Among the historical and foundational procedures is the Mitchell Osteotomy, a distal first metatarsal step-cut osteotomy first popularized in 1958. Designed to address mild-to-moderate hallux valgus deformities, the procedure achieves correction through a combination of medial eminence resection, lateral displacement and angulation of the capital fragment, and a meticulous medial capsulorrhaphy.
While the Mitchell osteotomy is currently less frequently utilized in developed countries—having been largely superseded by inherently more stable constructs such as the Austin/Chevron osteotomy—it remains a highly effective method when executed with precision. Furthermore, a profound understanding of the Mitchell procedure is mandatory for postgraduate orthopedic trainees (FRCS, AAOS) as it perfectly illustrates the critical biomechanical principles of first ray surgery, particularly the delicate balance between deformity correction, metatarsal length preservation, and the avoidance of transfer metatarsalgia.
Large retrospective reviews of the Mitchell operation in both adult and adolescent populations have demonstrated satisfactory clinical outcomes ranging from 74% to 94%. Nonunion rates are historically negligible when the osteotomy is correctly positioned within the vascular cancellous bone of the metatarsal neck, and recurrence of the valgus deformity is infrequent when the medial capsulorrhaphy is performed robustly.
INDICATIONS AND PATIENT SELECTION
The success of any distal metatarsal osteotomy relies heavily on stringent patient selection and precise preoperative radiographic analysis.
Primary Indications
- Mild to Moderate Hallux Valgus: Intermetatarsal angle (IMA) between 10° and 15°.
- Hallux Valgus Angle (HVA): Less than 30° to 35°.
- Congruent or Subluxated MTP Joint: Where lateral translation of the capital fragment can effectively restore articular congruity.
- Adolescent Hallux Valgus: Often utilized in juvenile populations where open physes (proximal first metatarsal) preclude proximal osteotomy techniques.
Contraindications
- Severe Deformity: IMA > 15° or HVA > 40°. Distal osteotomies cannot achieve sufficient lateral translation without compromising bone contact and stability.
- First Ray Hypermobility: Requires a proximal stabilization procedure (e.g., Lapidus arthrodesis).
- Degenerative Joint Disease: Hallux rigidus or advanced osteoarthritis of the first MTP joint is a contraindication for joint-sparing osteotomies.
- Short First Metatarsal: The Mitchell procedure inherently shortens the first ray by 5 to 6 mm; preexisting brachymetatarsia will severely exacerbate transfer lesions.
SURGICAL ANATOMY AND BIOMECHANICS
Vascular Supply to the Metatarsal Head
The most devastating complication of distal first metatarsal osteotomies is avascular necrosis (AVN) of the capital fragment. The primary blood supply to the first metatarsal head is derived from the first dorsal metatarsal artery and the plantar capsular arterial network.
Surgical Warning: Avoid aggressive stripping of the lateral capsule from the metatarsal head. The lateral capsular vessels are critical for the perfusion of the capital fragment once the medullary blood supply is interrupted by the osteotomy. The internervous midline medial incision is preferred to preserve this lateral vascular tether.
Biomechanics of the Step-Cut
The Mitchell osteotomy is a biplanar correction.
1. Lateral Translation: Shifting the capital fragment laterally reduces the 1-2 Intermetatarsal Angle (IMA). The width of the lateral bone spike dictates the magnitude of this translation.
2. Plantarflexion: Because the procedure inherently shortens the metatarsal (relaxing the adductor hallucis and lateral soft tissues), the capital fragment must be plantarflexed by approximately 10 degrees. This plantar displacement compensates for the functional shortening of the first ray, ensuring the first metatarsal head continues to bear its physiological share of forefoot loading during the terminal stance phase of gait.
PREOPERATIVE PLANNING: SIZING THE OSTEOTOMY
The geometric configuration of the Mitchell osteotomy must be templated preoperatively. The width of the lateral spike created depends entirely on the amount of correction required to relax the lateral soft tissues of the MTP joint and normalize the IMA.
- Mild Deformity (IMA 10° to 12°): A 3 to 4 mm lateral spike is sufficient.
- Moderate Deformity (IMA 13° to 15°): A 5 to 6 mm lateral spike is required to achieve adequate lateral translation.
SURGICAL TECHNIQUE: STEP-BY-STEP
1. Patient Positioning and Anesthesia
The patient is placed supine on the operating table. A regional ankle block or popliteal sciatic nerve block is highly recommended for postoperative analgesia, supplemented by monitored anesthesia care (MAC) or general anesthesia. A calf tourniquet is applied to provide a bloodless surgical field.
2. Skin and Capsular Incision
- Incision: Make the initial incision dorsomedially. Begin at the midshaft of the proximal phalanx, course dorsally over the medial eminence (bunion), and terminate approximately 3 cm proximal to the MTP joint on the medial aspect of the first metatarsal.
- Neural Protection: Carefully dissect the subcutaneous tissues. Avoid the terminal branches of the medial division of the superficial peroneal nerve when developing the dorsomedial flaps.
- Capsulotomy: Create a Y-shaped capsular incision.
> Clinical Pearl: Do not carry the arms of the Y-shaped capsular incision too far proximally. The capsular tissues become progressively thinner proximally, making the subsequent V-Y advancement and robust repair significantly more difficult.
3. Medial Eminence Resection
By sharp and blunt dissection, identify the medial eminence with its overlying capsule and bursa. Using an oscillating saw, resect the medial eminence. The cut should be conservative, starting at the parasagittal groove and directed slightly medially to preserve the articular cartilage and the tibial sesamoid articulation on the plantar aspect.
4. The Mitchell Osteotomy (The Double Cut)
This is the most technically demanding phase of the procedure. The osteotomy must be performed in the cancellous bone of the metatarsal neck.
Surgical Warning: Make the osteotomy no farther proximally than the anatomical neck. The critical cortical bone of the diaphyseal shaft takes significantly longer to heal than the cancellous neck. Furthermore, if the osteotomy is too far proximal, maintaining the toe in the desired corrected position becomes biomechanically difficult.
- First Cut (Distal): Using a fine oscillating saw blade, make an incomplete cut perpendicular to the metatarsal shaft. Leave the lateral cortex intact to form the lateral spike. The width of this spike (3-6 mm) is based on preoperative templating.
- Second Cut (Proximal): Make the second osteotomy in a similarly perpendicular direction to the metatarsal shaft, starting medially 3 to 4 mm proximal to the first cut. This proximal cut is a complete osteotomy and must pass entirely through the lateral cortex of the metatarsal.
- Bone Resection and Angulation: Remove the intervening 3 to 4 mm wafer of bone from the distal fragment.
> Critical Step: Diverge the two osteotomy cuts by approximately 10 degrees in a plantar direction. This trapezoidal bone resection facilitates the mandatory plantar flexion of the distal fragment upon closure of the osteotomy site.
5. Lateral Displacement of the Capital Fragment
- With the osteotomies completed and the lateral spike fashioned, manually shift the entire capital fragment laterally until the spike rests securely on the lateral cortex of the proximal fragment.
- Biomechanical Effect: This maneuver shortens the metatarsal by 5 to 6 mm, reduces the varus inclination of the first metatarsal, aligns the articular surface of the first metatarsal with that of the second, and effectively relaxes the adductor hallucis without requiring a separate lateral release.
6. Fixation
Historically, Mitchell utilized heavy suture fixation. Modern iterations often employ K-wires or small fragment compression screws, though the classic technique remains highly instructive.
* If using suture: Drill holes for the suture strictly perpendicular to the shaft. If drilled obliquely, they may communicate with the osteotomy site, leading to suture cut-out and loss of fixation.
* Protect the suture during the osteotomy, and tie it firmly but not roughly to avoid weakening the material.
* Positioning during fixation: Tie the suture (or place the hardware) while the capital fragment is held in approximately 10 degrees of plantar flexion.
7. Capsular Closure (Medial Capsulorrhaphy)
The soft tissue reconstruction is as critical as the bony work in preventing recurrence.
* Medial Flush: Before closing the capsule, inspect the medial aspect of the osteotomy. Resect any medial projection of bone on the proximal fragment so that it is perfectly flush with the medial edge of the displaced capital fragment.
* V-Y Advancement: Advance the V-shaped capsular flap into the straight limb of the Y-shaped incision.
* Tensioning: Perform this capsulorrhaphy while an assistant holds the hallux in 5 degrees of varus and slight plantar flexion. This overcorrection tensions the medial structures and acts as a dynamic checkrein against valgus recurrence.
COMPLICATIONS AND PITFALLS
While the nonunion rate is negligible and recurrence is infrequent, the Mitchell osteotomy is historically associated with specific, highly morbid complications if technical execution is flawed.
1. Transfer Metatarsalgia (The Most Troublesome Complication)
Transfer metatarsalgia to the lesser metatarsals (typically the second and third) is the most common and debilitating complication of the Mitchell procedure, as well as the related peg-in-hole procedure.
This occurs due to a failure to maintain the weight-bearing mechanics of the first ray, resulting from either:
1. Excessive Shortening: Resecting too large a bone wafer (>6 mm).
2. Dorsiflexion Malunion: Failure to diverge the osteotomy cuts by 10 degrees plantarward, or loss of fixation leading to dorsal angulation of the capital fragment.
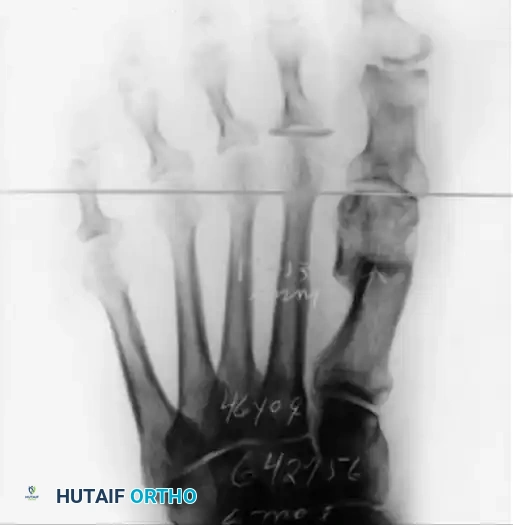
FIGURE 81-28 A: Anteroposterior weight-bearing radiograph demonstrating a failed Mitchell procedure. Note the excessive shortening of the first metatarsal, which has completely disrupted the metatarsal parabola, leading to severe transfer metatarsalgia beneath the second metatarsal head.
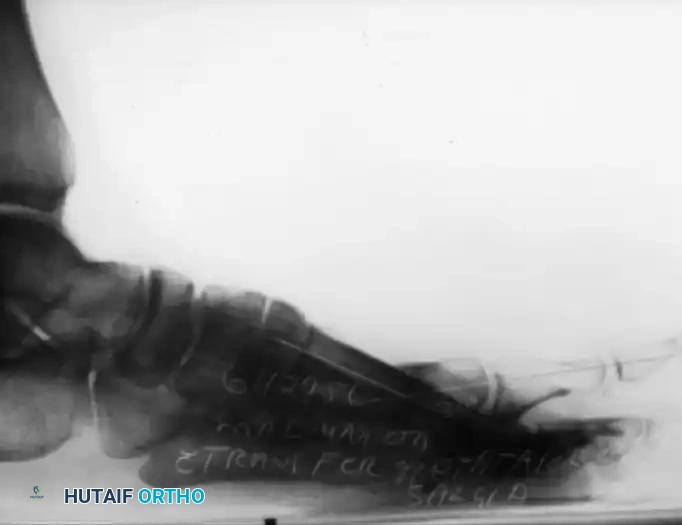
FIGURE 81-28 B: Lateral weight-bearing radiograph of the same patient. A dorsally angulated malunion of the capital fragment is clearly visible. This biplanar deformity (shortening plus dorsal elevation) completely unloads the first ray during the propulsive phase of gait. Correcting this iatrogenic biplanar deformity is surgically complex, often requiring a plantarflexing opening wedge osteotomy or structural bone grafting.
2. Avascular Necrosis (AVN) of the Metatarsal Head
As previously noted, stripping the lateral capsule destroys the terminal branches of the plantar and dorsal arterial networks. The surgeon must rely on the lateral soft tissue hinge for perfusion. AVN presents postoperatively as joint stiffness, pain, and radiographic sclerosis or collapse of the metatarsal head.
3. Instability and Displacement
- Asymmetrical Spike: Avoid creating an uneven or asymmetrical lateral spike on the distal fragment. A poorly fashioned spike fails to lock onto the proximal lateral cortex, resulting in rotational instability and displacement.
- Suture Failure: If the drill holes communicate with the osteotomy, the fixation will fail, leading to the aforementioned dorsal malunion.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol must protect the osteotomy while it consolidates, preventing dorsal displacement.
Historical Protocol (Mitchell's Original)
Mitchell originally recommended that padded tongue blades be placed plantar, medially, and dorsally, held in place with rolled gauze for the first 10 days after surgery. Following suture removal, a short-leg walking cast with a rigid toe plate was applied. The cast was worn until the osteotomy demonstrated radiographic healing, usually requiring 6 to 8 weeks. Great care was taken during casting to avoid angulating the distal fragment or displacing it dorsally.
Modern Protocol
Contemporary postoperative management typically involves:
* Weeks 0-2: Application of a bulky, compressive Jones dressing reinforced with a plaster splint. The patient is restricted to heel-weight-bearing only in a rigid postoperative shoe. Elevation is strictly enforced to minimize edema.
* Weeks 2-6: Sutures are removed at 14 days. The patient is transitioned to a short-leg walking cast with a toe plate, or a rigid pneumatic walker boot. Weight-bearing is gradually advanced based on radiographic evidence of callus formation.
* Weeks 6-8: Upon confirmation of clinical and radiographic union, the patient is transitioned to supportive athletic footwear. Aggressive first MTP joint range-of-motion exercises are initiated to prevent arthrofibrosis, focusing heavily on restoring active and passive dorsiflexion.
CONCLUSION
The Mitchell osteotomy remains a masterclass in the biomechanics of forefoot reconstruction. While modern rigid fixation techniques and inherently stable osteotomy geometries (like the Chevron) have reduced its routine application, the principles established by Mitchell et al. in 1958—meticulous preservation of blood supply, precise geometric bone resection, mandatory plantarflexion to prevent transfer metatarsalgia, and robust capsulorrhaphy—remain the foundational tenets of all successful hallux valgus surgery today.
You Might Also Like

