Mastering Hallux Valgus: Pathoanatomy and Surgical Strategies
Key Takeaway
Hallux valgus is a complex progressive deformity of the first ray characterized by lateral deviation of the great toe and medial deviation of the first metatarsal. This comprehensive guide details the pathoanatomy, biomechanics, and evidence-based surgical management of hallux valgus. It provides orthopaedic surgeons with step-by-step approaches for soft tissue balancing, metatarsal osteotomies, and arthrodesis, ensuring optimal functional outcomes and minimizing postoperative complications.
Disorders of the Hallux: A Comprehensive Surgical Guide
Hallux valgus, commonly referred to as a bunion, represents one of the most frequent and complex forefoot deformities encountered by the orthopaedic surgeon. It is not merely a cosmetic prominence of the medial eminence but a progressive, multiplanar subluxation of the first metatarsophalangeal (MTP) joint. Successful management requires a profound understanding of first ray biomechanics, meticulous clinical and radiographic evaluation, and the precise execution of soft tissue and bony reconstructive procedures.
This masterclass provides a postgraduate-level analysis of hallux valgus and related first ray disorders, detailing the pathoanatomy, surgical decision-making algorithms, and step-by-step operative techniques required to achieve durable, functional correction.
Pathoanatomy and Biomechanics of Hallux Valgus
The pathogenesis of hallux valgus is characterized by the progressive failure of the medial stabilizing structures of the first MTP joint, leading to a cascade of biomechanical derangements.

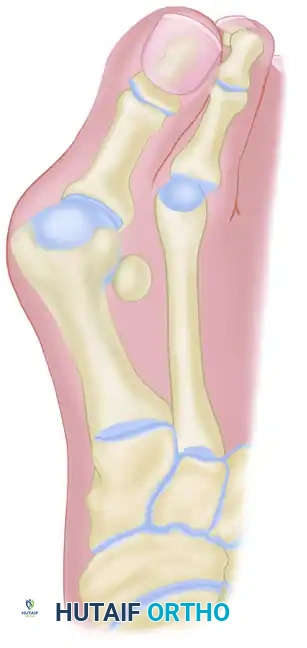
The essential lesion is often debated—whether it originates as metatarsus primus varus (medial deviation of the first metatarsal) or lateral deviation of the proximal phalanx. Current evidence suggests that in adults, lateral deviation of the great toe is typically the primary event, followed by secondary medial angulation of the first metatarsal. Conversely, in juvenile and adolescent populations, metatarsus primus varus may be the primary structural anomaly.
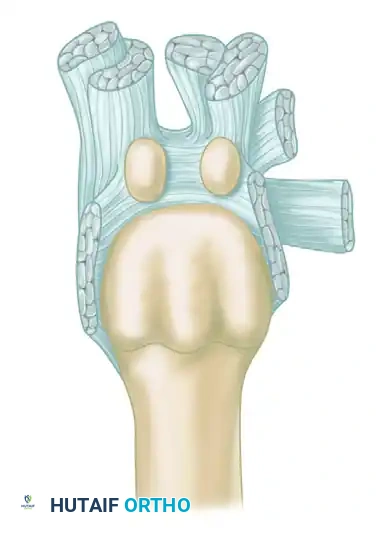
The Intrinsic Muscle Imbalance
As the proximal phalanx deviates laterally, the anatomical alignment of the intrinsic and extrinsic musculature is profoundly altered:
* Abductor Hallucis: Normally a medial stabilizer, the abductor hallucis tendon slides plantarward beneath the metatarsal head. It loses its abducting moment and becomes a deforming force, contributing to the pronation and flexion of the hallux.
* Adductor Hallucis: Unopposed by the abductor hallucis, the adductor hallucis pulls the proximal phalanx further laterally.
* Extensor Hallucis Longus (EHL) and Flexor Hallucis Longus (FHL): As the MTP joint subluxates, these powerful extrinsic tendons bowstring laterally across the joint, acting as a bowstring that exponentially exacerbates the valgus deformity.

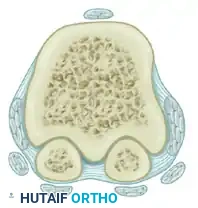

The Sesamoid Apparatus
The sesamoids are embedded within the plantar plate and the tendons of the flexor hallucis brevis (FHB). They do not actively subluxate laterally; rather, the first metatarsal head drifts medially off the sesamoid apparatus.
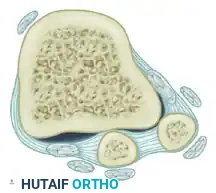
As the metatarsal head moves medially, the sesamoid sling apparatus becomes a valgus deforming force, and the metatarsal rotates (pronates) on its longitudinal axis. The crista, which normally separates the medial and lateral sesamoid grooves, is eroded, leading to intractable pain and osteoarthritis if left uncorrected.
Clinical Pearl: Hypertrophy of the medial eminence is largely an illusion. Recent 3D imaging studies confirm that true bony proliferation is minimal. The prominence is primarily the uncovered medial aspect of the metatarsal head resulting from metatarsus primus varus and lateral phalangeal deviation.
Etiology and Clinical Presentation
The etiology of hallux valgus is multifactorial. While unphysiologically designed footwear (narrow toe box, high heels) is a major extrinsic exacerbating factor in modern societies, intrinsic genetic predisposition plays a paramount role.
Other contributing anatomical factors include:
* Pronated flatfoot deformity (pes planus).
* Hypermobility of the first tarsometatarsal (TMT) joint.
* Increased obliquity of the first metatarsomedial cuneiform joint.
* An abnormally long first ray.
* Achilles tendon contracture, which drives forefoot overload.
Clinical Evaluation
Patients typically present with pain over the medial eminence, difficulty with footwear, and cosmetic concerns. The valgus posture of the great toe frequently causes a crossover or hammer toe deformity of the second toe due to spatial crowding.
A comprehensive physical examination must assess:
1. First MTP Joint Range of Motion: Assess for crepitus or pain indicative of concurrent hallux rigidus (osteoarthritis).
2. First Ray Mobility: Evaluate the first TMT joint for hypermobility in the sagittal plane.
3. Lesser Toe Deformities: Check for metatarsalgia, plantar callosities, and second MTP joint instability.
4. Achilles Tendon: Perform the Silfverskiöld test to identify isolated gastrocnemius tightness versus Achilles contracture.
Preoperative Radiographic Evaluation
Standard weight-bearing anteroposterior (AP), lateral, and sesamoid axial radiographs are mandatory. Surgical decision-making relies heavily on precise angular measurements.

Key Radiographic Parameters
- Hallux Valgus Angle (HVA): The angle between the longitudinal axes of the first metatarsal and proximal phalanx. Normal is < 15°.
- Intermetatarsal Angle (IMA): The angle between the longitudinal axes of the first and second metatarsals. Normal is < 9°.
- Distal Metatarsal Articular Angle (DMAA): The angle between the articular surface of the first metatarsal head and the longitudinal axis of the metatarsal shaft. Normal is < 10°. An increased DMAA indicates a congruous joint in a valgus position, necessitating a specific intra-articular or extra-articular corrective osteotomy.



Surgical Warning: Failure to recognize an abnormal DMAA will lead to undercorrection or early recurrence. If a standard proximal osteotomy is performed without addressing the valgus articular orientation, the joint will remain congruous in valgus, and the deformity will persist.
Surgical Decision Making: The Algorithm
With over 130 operations described for hallux valgus, procedure selection must be tailored to the severity of the deformity, the presence of arthritis, and the stability of the first TMT joint.
- Mild Deformity (HVA < 30°, IMA < 13°): Distal metatarsal osteotomy (e.g., Chevron) with lateral soft tissue release.
- Moderate Deformity (HVA 30°–40°, IMA 13°–20°): Diaphyseal osteotomy (e.g., Scarf) or proximal metatarsal osteotomy (e.g., Ludloff, Crescentic) combined with a distal soft tissue procedure.
- Severe Deformity (HVA > 40°, IMA > 20°): Proximal metatarsal osteotomy or First TMT joint arthrodesis (Lapidus procedure), especially if hypermobility is present.
- Degenerative Joint Disease: Arthrodesis of the first MTP joint.
Operative Techniques
1. Soft Tissue Procedures (Modified McBride)
Historically, the McBride procedure involved excision of the fibular sesamoid. This is now largely abandoned due to the high risk of iatrogenic hallux varus. The modified McBride involves a lateral soft tissue release and medial capsulorrhaphy without sesamoidectomy.
Surgical Steps:
* Approach: A dorsal first web space incision is made.
* Release: The adductor hallucis tendon is detached from the base of the proximal phalanx and the fibular sesamoid. The deep transverse metatarsal ligament is transected.
* Medial Capsulorrhaphy: A medial longitudinal incision exposes the medial eminence. The redundant medial capsule is excised, and the capsule is imbricated to realign the toe.
Note: Soft tissue procedures alone are rarely sufficient for durable correction and are almost always combined with a bony osteotomy.
2. Osteotomy of the Distal First Metatarsal (Chevron)
The Chevron osteotomy is the workhorse for mild to moderate hallux valgus. It is an inherently stable, V-shaped osteotomy of the metatarsal head.
Surgical Steps:
* Positioning: Supine with a bump under the ipsilateral hip. Ankle or calf tourniquet applied.
* Approach: A medial midline incision is made over the first MTP joint.
* Capsulotomy: An inverted L-shaped or V-shaped capsulotomy is performed.
* Exostectomy: The medial eminence is resected parallel to the medial border of the foot, preserving the sagittal groove to avoid staking the metatarsal head.
* Osteotomy: A 60-degree V-cut is made with the apex centered in the metatarsal head, pointing distally. The plantar arm should exit proximal to the sesamoids to avoid avascular necrosis (AVN).
* Translation: The capital fragment is translated laterally by 4 to 5 mm (up to 50% of the bone width).
* Fixation: The osteotomy is secured with a single headless compression screw or K-wire.
* Closure: The medial capsule is tightly repaired to hold the toe in neutral alignment.
* Postoperative Protocol: Heel-weight-bearing in a rigid postoperative shoe for 4 to 6 weeks.
3. Osteotomy of the Proximal First Metatarsal
For moderate to severe deformities with a high IMA, a proximal osteotomy provides a greater arc of correction. Common techniques include the Crescentic, Ludloff, and proximal opening/closing wedge osteotomies.
Surgical Steps (Crescentic Osteotomy):
* Approach: A dorsal longitudinal incision over the proximal first metatarsal.
* Osteotomy: A crescentic saw blade is used to make a dome-shaped cut 1 cm distal to the first TMT joint, with the concavity facing proximally.
* Correction: The distal fragment is rotated laterally to reduce the IMA.
* Fixation: Secured with a specialized plate or crossed compression screws.
* Postoperative Protocol: Strict non-weight-bearing or heel-weight-bearing in a cast/boot for 6 weeks, as proximal osteotomies are less inherently stable than distal ones.
4. Proximal Phalangeal Osteotomy (Akin)
The Akin osteotomy is a medially based closing wedge osteotomy of the proximal phalanx. It does not correct the IMA or the primary MTP subluxation. It is strictly an adjunctive procedure used to correct residual hallux valgus interphalangeus or an abnormal distal articular set angle (DASA).
Surgical Steps:
* Approach: Medial incision over the proximal phalanx.
* Osteotomy: A medially based wedge of bone is removed from the metaphyseal flare, leaving the lateral cortex intact as a hinge.
* Fixation: Closed and secured with a staple, suture, or headless screw.
5. Arthrodesis of the First Metatarsophalangeal Joint
Arthrodesis is the gold standard for severe hallux valgus, recurrent deformities, rheumatoid arthritis, and hallux rigidus. It provides predictable, permanent pain relief and deformity correction.
Surgical Steps:
* Preparation: The articular cartilage of the metatarsal head and proximal phalanx is denuded using cup-and-cone reamers to expose bleeding subchondral bone.
* Positioning (CRITICAL): The hallux must be fused in:
* 10° to 15° of valgus.
* 15° of dorsiflexion relative to the first metatarsal (or neutral to the floor).
* Neutral rotation.
* Fixation: A dorsal contoured locking plate combined with an interfragmentary lag screw provides the most robust biomechanical construct.
Special Populations
Juvenile and Adolescent Hallux Valgus (10 to 19 Years Old)
Adolescent hallux valgus is characterized by a strong familial predisposition, a high incidence of metatarsus primus varus, and an increased DMAA.
* Surgical Timing: Surgery should be delayed until physeal closure if possible to prevent growth arrest.
* Procedure Selection: Distal osteotomies are often required to correct the DMAA, frequently combined with a proximal osteotomy to correct the severe IMA (double osteotomy).
Hallux Valgus in Cerebral Palsy
Patients with spasticity present a unique challenge. Muscle imbalance (spastic adductor hallucis) leads to rapid recurrence if standard osteotomies are used. First MTP arthrodesis is the procedure of choice in the adult cerebral palsy patient to ensure definitive correction.
Complications After Surgery for Hallux Valgus
1. Recurrent Deformity
Recurrence is the most common complication, often resulting from inadequate initial correction (e.g., performing a distal osteotomy for a severe deformity), failure to recognize an abnormal DMAA, or unaddressed first TMT hypermobility. Revision surgery typically requires a proximal osteotomy or Lapidus procedure.
2. Acquired Hallux Varus
Hallux varus (medial deviation of the toe) is a disastrous complication caused by:
* Over-resection of the medial eminence ("staking the head").
* Excessive lateral soft tissue release (especially excision of the fibular sesamoid).
* Over-plication of the medial capsule.
Treatment: Mild, flexible cases may respond to EHL transfer (extensor hallucis brevis tenodesis). Rigid or arthritic cases require MTP arthrodesis.
3. Avascular Necrosis (AVN) of the Metatarsal Head
AVN is a risk following distal osteotomies, particularly if an extensive lateral soft tissue release is performed simultaneously, disrupting the extraosseous blood supply. Surgeons must preserve the plantar-lateral capsular attachments during the Chevron procedure.
4. Complications of Resection Arthroplasty (Keller)
The Keller procedure (resection of the base of the proximal phalanx) is historically used for elderly, low-demand patients. Complications include "cock-up" deformity (loss of intrinsic flexor power), transfer metatarsalgia, and a flail toe. It has largely been superseded by MTP arthrodesis.
Hallux Rigidus
Hallux rigidus is osteoarthritis of the first MTP joint, characterized by dorsal osteophyte formation and restricted, painful dorsiflexion.
Nonoperative Treatment
Management begins with rigid Morton extensions, rocker-bottom shoes, and intra-articular corticosteroid injections.
Operative Treatment
- Cheilectomy: For early-stage disease (Grades 1 and 2). Involves resection of the dorsal 30% of the metatarsal head and removal of dorsal osteophytes to decompress the joint and restore dorsiflexion.
- Arthrodesis: The definitive treatment for end-stage (Grade 3 and 4) hallux rigidus.
Sesamoid Injuries of the Hallux
The sesamoids function to absorb weight-bearing forces and increase the mechanical advantage of the FHB. Injuries include acute fractures, stress fractures, and sesamoiditis.
Treatment
- Conservative: Offloading with dancer's pads, stiff-soled shoes, or cast immobilization.
- Operative: If conservative measures fail after 6 months, partial or complete excision of the affected sesamoid may be indicated. Excision of both sesamoids must be avoided, as it inevitably leads to a cock-up deformity or hallux varus/valgus depending on the remaining muscular imbalance.
Surgical Pearl: When excising a sesamoid, meticulous repair of the plantar plate and FHB tendon defect is mandatory to prevent postoperative toe destabilization.
This guide synthesizes the foundational principles and advanced surgical techniques required for the mastery of hallux valgus correction. Adherence to strict biomechanical principles, precise radiographic analysis, and meticulous soft-tissue handling will optimize patient outcomes and minimize the risk of complex revision scenarios.
You Might Also Like

