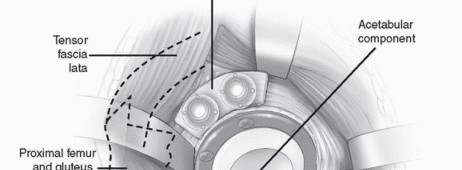
Recreate Hip Biomechanics: Modular Stems for Modular Solutions

Key Takeaway
This article provides essential research regarding Recreate Hip Biomechanics: Modular Stems for Modular Solutions. Modular stems modular femoral components are primarily indicated in primary total hip arthroplasty for conditions involving abnormal acetabular or femoral anatomy. This includes developmental dysplasia, severe deformities, or irregular femoral canal shapes. They provide varied options for offset, length, and version, helping restore normal biomechanics and soft tissue balance effectively.
Introduction and Epidemiology
Total hip arthroplasty (THA) is one of the most successful interventions in modern orthopedic surgery, providing predictable pain relief and functional restoration for patients with end-stage hip joint pathology. While the vast majority of primary THA procedures can be successfully executed using standard monolithic femoral components, a distinct subset of patients presents with complex proximal femoral anatomy or severe deformities that preclude the use of standard off-the-shelf implants. Modular femoral stems were developed specifically to address these challenging anatomic variations, allowing the surgeon to independently manage distal fixation, proximal fill, femoral offset, leg length, and femoral version.
The epidemiology of conditions requiring modular femoral stems is diverse. Elements of developmental dysplasia of the hip (DDH) and structural deformity occur frequently in the primary THA population. A comprehensive review of 75 hips with a diagnosis of idiopathic osteoarthritis revealed proximal femoral deformity in 40% of hips and acetabular dysplasia in 39% of hips. The variable shape of the femoral canal, often quantified by the canal flare index, can lead to a significant proximal/distal mismatch. This mismatch makes it exceedingly difficult to achieve simultaneous proximal and distal fit and fill with a standard monolithic femoral component. If a monolithic stem is sized to fit a narrow distal canal, it may fail to adequately fill a capacious proximal metaphysis, leading to instability, subsidence, or inadequate stress transfer. Conversely, sizing a monolithic stem to fill a large proximal metaphysis may result in distal cortical impingement, intraoperative periprosthetic fracture, or thigh pain due to distal load transfer.

Other frequent conditions producing distorted anatomy include prior surgical interventions (such as proximal femoral osteotomies), posttraumatic deformities, and secondary osteoarthritis arising from childhood conditions like Legg-Calve-Perthes disease, slipped capital femoral epiphysis (SCFE), and prior hip sepsis. Less common conditions that frequently necessitate modularity include exceptionally small femoral canals seen in juvenile rheumatoid arthritis, dwarfism, and spondyloperipheral dysplasia. Conversely, pathologically large femoral canals, such as those classified as Dorr Type C bone, or those altered by ankylosing spondylitis, rheumatoid arthritis, alcoholic bone disease, and Paget disease, also represent primary indications for modular femoral reconstruction.
Surgical Anatomy and Biomechanics
The primary goal of any THA is the recreation of normal hip biomechanics to optimize the abductor moment arm, minimize joint reaction forces, and ensure joint stability. The proximal femur is a complex three-dimensional structure characterized by its cervicodiaphyseal angle (neck-shaft angle), femoral version (anteversion of the neck relative to the transcondylar axis of the distal femur), and femoral offset (the perpendicular distance from the center of rotation of the femoral head to the anatomical axis of the femoral shaft).
Proximal Distal Mismatch and Canal Flare Index
The canal flare index (CFI) is defined as the ratio of the intracortical width of the femur at a point 20 mm proximal to the lesser trochanter to the canal width at the isthmus. Normal femurs typically exhibit a CFI between 3.0 and 4.7. A CFI greater than 4.7 indicates a "champagne flute" canal (highly tapered), while a CFI less than 3.0 indicates a "stovepipe" canal (cylindrical, often Dorr Type C). In cases of severe proximal/distal mismatch, modular stems allow the surgeon to select a distal stem diameter that achieves rigid diaphyseal fixation (either through cylindrical milling or tapered reaming) independently of the proximal body size required to fill the metaphysis and support the abductor musculature.
Independent Control of Biomechanical Parameters
Modular femoral components offer a large array of femoral offset, length, and version options. In a monolithic stem, altering the version inherently alters the position of the distal stem within the diaphysis, which may be constrained by the bow of the femur. Modularity, particularly at the metaphyseal-diaphyseal junction or the neck-body junction, allows the distal stem to be seated in its most stable, anatomically dictated position within the diaphysis. Subsequently, the proximal body or neck can be rotated to dial in the exact degree of anteversion required to achieve combined anteversion (typically targeting 25 to 35 degrees of combined acetabular and femoral version) for optimal stability.

Furthermore, modular necks or proximal bodies provide independent adjustment of leg length and horizontal offset. Restoring horizontal offset is critical for tensioning the abductor musculature, which decreases the required abductor muscle force during the single-leg stance phase of gait, thereby reducing the overall joint reaction force transmitted across the bearing surface. Failure to restore offset can lead to abductor weakness, a persistent Trendelenburg gait, and an increased risk of dislocation due to soft tissue laxity.

Indications and Contraindications
While useful in most hips requiring primary THA, modular femoral stems are specifically indicated in conditions with abnormal acetabular and/or femoral anatomy where standard implants would compromise biomechanical restoration or fixation.
Primary Indications
- Developmental Dysplasia of the Hip (DDH): Crowe Type III and IV DDH often present with excessive femoral anteversion, a narrow diaphysis, and a posteriorly displaced greater trochanter. Modular stems allow for distal fixation in the narrow canal and independent retroversion of the proximal body to correct the excessive native anteversion.
- Post-Traumatic Deformity: Malunions of intertrochanteric or subtrochanteric fractures often leave complex multi-planar deformities.
- Prior Osteotomy: Patients with a history of varus derotational osteotomies (VDRO) or valgus producing osteotomies present with distorted cervicodiaphyseal angles and retained hardware trajectories that dictate distal stem placement independent of proximal anatomy.
- Metabolic and Congenital Bone Diseases: Paget disease (characterized by severe anterolateral bowing), osteopetrosis, and dwarfism.

Contraindications
Contraindications to modular femoral stems are rare but must be strictly observed to prevent catastrophic failure.
1. Extreme Femoral Canal Deformity: In cases where the diaphysis is obliterated or the deformity is so severe that even a modular stem cannot bypass the apex of the deformity without cortical perforation, custom triflanged components, custom machined stems, or cemented fixation may be more easily and safely achieved.
2. Direct Anterior Approach (DAA): The direct anterior approach is generally contraindicated when using a modular femoral stem. The DAA often limits the ability to safely ream the distal diaphysis in a straight line without the risk of greater trochanteric fracture or anterior cortical perforation. Furthermore, assembling a modular metaphyseal-diaphyseal junction in vivo through the limited DAA window is technically demanding and risks inadequate taper engagement, which can lead to dissociation or accelerated corrosion.
3. Inadequate Bone Stock for Diaphyseal Fixation: If the diaphyseal cortices are paper-thin and cannot support the hoop stresses of a distally fixing modular stem, a cemented long stem may be preferable.
Operative vs Non Operative Management
The decision to proceed with modular THA versus non-operative management depends on the severity of symptoms and the progression of the underlying deformity.
| Clinical Scenario | Indications for Non-Operative Management | Indications for Operative Intervention (Modular THA) |
|---|---|---|
| Developmental Dysplasia (DDH) | Mild symptoms, preserved joint space, manageable with NSAIDs and physical therapy. | End-stage osteoarthritis, severe pain, progressive leg length discrepancy, abductor fatigue. |
| Post-Traumatic Malunion | Asymptomatic malunion, functional range of motion, acceptable compensatory gait. | Intractable pain, hardware failure, progressive secondary osteoarthritis, severe leg length discrepancy. |
| Legg-Calve-Perthes / SCFE | Pain controlled with conservative measures, minimal functional limitation. | Severe coxa brevis, impingement symptoms refractory to arthroscopy/osteoplasty, advanced joint space narrowing. |
| Paget Disease of Bone | Metabolically active disease without severe secondary joint destruction (treat with bisphosphonates). | End-stage secondary hip osteoarthritis, impending pathologic fracture, severe functional limitation. |
Pre Operative Planning and Patient Positioning
Detailed history, physical, and radiographic evaluation are mandatory for any patient undergoing primary THA, but they take on heightened importance when complex anatomy necessitates a modular stem.
Clinical Evaluation
The history should focus on prior treatments, surgeries, and complications. The exact nature of prior pediatric interventions (e.g., spica casting, osteotomies, epiphysiodesis) must be documented. The patient's disabilities, including subjective leg length discrepancy, fatigue, limp, and pain patterns, should be thoroughly discussed to align surgical goals with patient expectations.
Physical examination will often reveal abnormalities in size, range of motion (noting specific planes of stiffness or laxity), and prior surgical incisions. Prior incisions dictate the surgical approach to minimize the risk of skin necrosis. Surgeries to the contralateral limb must be noted. Leg lengths are objectively assessed by tape measure (anterior superior iliac spine to medial malleolus) and functionally assessed using calibrated blocks under the short limb to determine the exact discrepancy and to ascertain what length appears to best balance the pelvis and correct functional scoliosis. Thorough preoperative assessment of femoral and sciatic nerve function is essential, particularly in DDH patients requiring significant lengthening, as the sciatic nerve is at high risk for stretch neuropraxia.
Radiographic Evaluation and Templating
Plain radiographs must include an anteroposterior (AP) projection of the pelvis, an AP of the involved hip, and a Lauenstein (frog-leg) lateral x-ray. Radiographic magnification markers (typically a 25 mm or 30 mm sphere) taped to the involved hip at the level of the greater trochanter allow for an accurate estimate of x-ray magnification. This permits precise digital templating of the femoral canal.
Templating a modular stem is a sequential process:
1. Distal Fixation: The distal stem is templated first to ensure adequate cortical contact (typically 4-6 cm of scratch fit in the diaphysis) while bypassing any stress risers or deformity apices by at least two cortical diameters.
2. Proximal Fill: The proximal body is then templated to fill the metaphysis and reconstitute the medial calcar.
3. Offset and Length: The modular neck or proximal body geometry is selected to recreate the center of rotation, horizontal offset, and leg length.
Computer tomography (CT) scans are rarely indicated for routine THA but are invaluable in complex cases to provide a highly accurate assessment of native femoral anteversion, precise femoral canal dimensions, and acetabular bone stock. Scanograms or full-length standing AP radiographs of the lower extremities may be useful to more accurately assess true limb length inequalities and global coronal alignment.
Patient Positioning
The patient is positioned in the lateral decubitus position with the affected side up. Rigid pelvic fixation using peg boards or specialized pelvic positioners is critical to maintain true lateral positioning throughout the procedure, which is essential for accurate intraoperative assessment of version and leg length. The underlying leg is placed in flexion to reduce the degree of lumbar lordosis and to stabilize the pelvis against rolling. All bony prominences, particularly the common peroneal nerve at the fibular head of the down leg, must be meticulously padded.
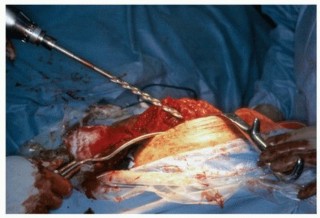
Detailed Surgical Approach and Technique
Given the contraindication of the direct anterior approach for most modular stem systems, the posterior or posterolateral approach is the workhorse for complex femoral reconstructions. It provides unparalleled, extensile access to the proximal femur and diaphysis.
Surgical Approach
An incision is made centered over the posterior aspect of the greater trochanter, extending proximally toward the posterior superior iliac spine and distally along the femoral shaft. The subcutaneous tissues are divided, and the fascia lata is incised in line with the skin incision. Proximally, the gluteus maximus is split bluntly in line with its fibers.
The Charnley retractor is placed to retract the gluteus maximus. The short external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus, and quadratus femoris) are identified. A tag stitch is placed in the conjoined tendon, and the rotators are taken down from their insertion on the greater trochanter and reflected posteriorly to protect the sciatic nerve. A complete capsulotomy is performed, and the hip is dislocated posteriorly with gentle flexion, adduction, and internal rotation. In cases of severe deformity or protrusio, an in situ femoral neck cut may be required prior to dislocation to prevent iatrogenic fracture.
Femoral Preparation
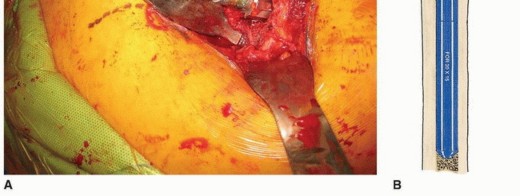
Following acetabular preparation and component insertion, attention is turned to the femur. The femur is elevated and mobilized. Adequate soft tissue release, including release of the gluteus maximus insertion on the linea aspera if necessary, is performed to allow straight-line access to the femoral canal.

The femoral canal is initially opened with a box osteotome or starter awl, ensuring lateralization into the greater trochanter to prevent varus malalignment of the stem.
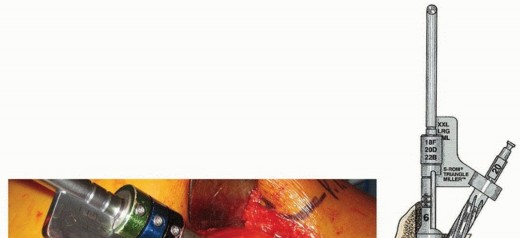
Distal Preparation: For modular stems utilizing diaphyseal fixation (typically fluted, tapered, or cylindrical distal stems), rigid straight reamers are utilized. Reaming is performed sequentially until cortical chatter is achieved, indicating rigid diaphyseal engagement. The depth of reaming is dictated by preoperative templating and the specific implant design.

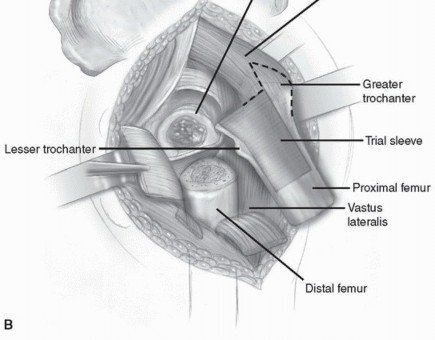
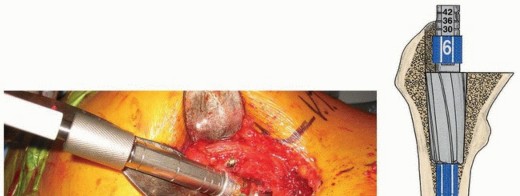
Proximal Preparation: Once the distal canal is prepared, a trial distal stem is inserted. Proximal preparation is then performed over the trial distal stem or a guide wire to ensure the proximal metaphysis is prepared coaxially with the distal diaphysis. Depending on the system, this involves sequential proximal milling or broaching. The proximal body size is selected to provide rotational stability and to fill the metaphyseal bone without causing cortical fracture.
Trialing and Assembly
With the distal trial and proximal trial body in place, trial necks and heads are applied. This is the critical juncture where the modularity is leveraged. The surgeon can independently rotate the proximal body or modular neck to set the femoral anteversion, independent of the distal stem's position in the diaphysis.

The hip is reduced, and a comprehensive stability examination is performed. The hip is taken through a full range of motion, checking for impingement, soft tissue tension, and tendency for dislocation in flexion/internal rotation (posterior instability) and extension/external rotation (anterior instability). Leg lengths are assessed by comparing the level of the medial malleoli or by intraoperative measurement from a fixed pelvic pin to a point on the femur.
Final Implantation
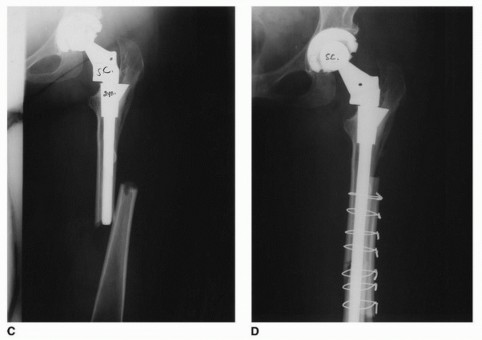
Once the optimal trial components are identified, the trials are removed. The final distal stem is impacted into the diaphysis until it achieves a rigid, rotationally stable interference fit.
Taper Assembly: The assembly of the modular junction (whether mid-stem or neck-body) is the most technique-sensitive portion of the procedure. The male and female tapers must be meticulously cleaned of all blood, fat, and bone debris, and completely dried. Contamination of the Morse taper junction significantly increases the risk of mechanically assisted crevice corrosion and subsequent failure.
The proximal body is applied in the exact version determined during trialing. The components are engaged using the manufacturer-specific impaction tool. Multiple firm strikes with a heavy mallet are required to achieve cold welding of the Morse taper.
The final femoral head is applied, and the hip is reduced. A final check of stability and leg length is performed before meticulous closure of the capsule, short external rotators, fascia, and skin.
Complications and Management
While modular stems provide elegant solutions to complex anatomic problems, the introduction of additional mechanical junctions introduces unique modes of failure and specific complications that the orthopedic surgeon must be prepared to manage.
Specific Complications of Modularity
- Mechanically Assisted Crevice Corrosion (MACC) and Fretting: Micro-motion at the modular junction can strip the passivating oxide layer of the titanium or cobalt-chrome alloy. This leads to a localized galvanic corrosion process, releasing metal ions into the surrounding tissue. This can result in an adverse local tissue reaction (ALTR) or aseptic lymphocyte-dominated vasculitis-associated lesion (ALVAL), presenting as pain, swelling, and pseudotumor formation.
- Component Dissociation: Inadequate impaction or soft tissue interposition during assembly can lead to failure of the Morse taper to engage, resulting in early postoperative dissociation of the stem.
- Stem Fracture: The modular junction acts as a stress riser. In patients with high BMI, high activity levels, or lack of proximal bony support (leading to cantilever bending forces), fatigue fracture of the stem at the modular junction can occur.

General THA Complications in Complex Anatomy
- Intraoperative Periprosthetic Fracture: The preparation of deformed, sclerotic, or osteoporotic bone carries a high risk of fracture. Prophylactic cable placement around the proximal femur prior to broaching is often recommended in high-risk cases.
- Subsidence: Failure to achieve adequate distal cortical engagement can lead to axial subsidence of the stem.
- Nerve Injury: Lengthening a chronically shortened limb (e.g., in high DDH) places the sciatic nerve at risk of stretch neuropraxia. Intraoperative somatosensory evoked potentials (SSEPs) or motor evoked potentials (MEPs) may be utilized.
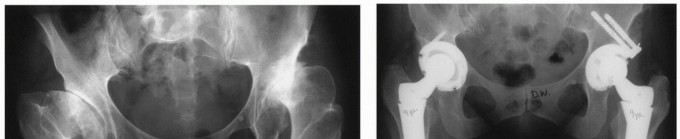
Table of Complications and Salvage Strategies
| Complication | Estimated Incidence in Complex THA | Management / Salvage Strategy |
|---|---|---|
| Intraoperative Calcar Fracture | 3 - 8% | Cerclage wiring or cabling; bypass fracture by 2 cortical diameters with the distal stem. |
| MACC / Pseudotumor (ALTR) | 1 - 5% (Design dependent) | Revision THA with debridement of necrotic tissue; conversion to monolithic stem if anatomy allows, or use of ceramic heads with titanium sleeves. |
| Modular Junction Dissociation | < 1% | Immediate open reduction, meticulous cleaning of tapers, and re-impaction. If tapers are damaged, component revision is required. |
| Stem Fatigue Fracture | < 1% | Extraction of distal segment (often requires extended trochanteric osteotomy or trephine reamers); revision to a larger diameter, robust modular or monolithic revision stem. |
| Sciatic Nerve Palsy | 1 - 3% (Higher in DDH) | Observation, ankle-foot orthosis (AFO) for foot drop. If recognized intraoperatively, release tension by shortening the construct. |

Post Operative Rehabilitation Protocols
Rehabilitation following THA with a modular stem is largely dictated by the complexity of the reconstruction and the quality of the bone-implant
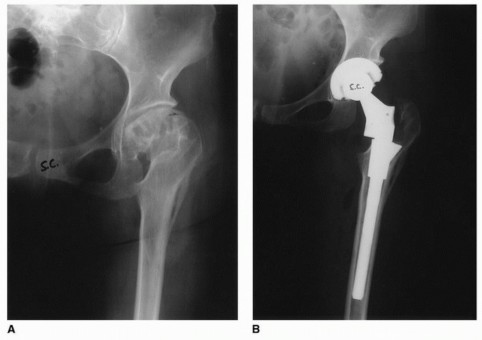
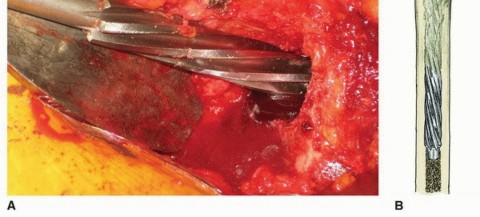
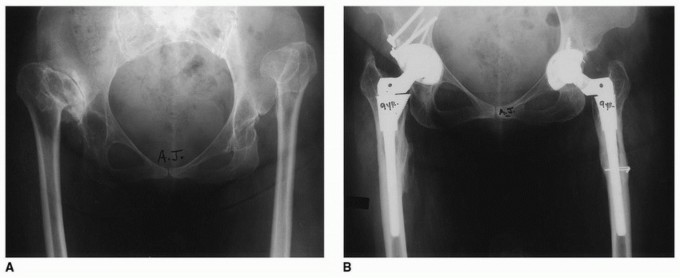
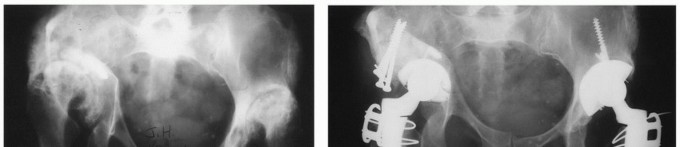
Clinical & Radiographic Imaging

You Might Also Like


