Medial Epi Condyle Fracture: Expert Guide to Healing & Stability

Key Takeaway
For anyone wondering about Medial Epi Condyle Fracture: Expert Guide to Healing & Stability, A medial epi condyle fracture is an injury to the apophysis on the elbow's medial aspect, where the flexor-pronator muscle mass and ulnar collateral ligament attach. These fractures commonly occur as an avulsion from a fall on an outstretched arm, with muscle tension or ligament disruption causing the injury. Direct blows or associated elbow dislocations are also possible causes.
Introduction and Epidemiology
Fractures of the medial epicondyle represent a distinct spectrum of elbow injuries, often observed in both pediatric and adult populations, with significant implications for elbow stability and function. This injury involves the apophysis of the medial epicondyle, a critical anatomical landmark serving as the origin for the common flexor-pronator muscle mass and the ulnar collateral ligament (UCL). While less common than lateral condyle fractures in some pediatric series, medial epicondyle fractures are frequently associated with elbow dislocations, underscoring their importance in the context of elbow trauma and instability.
Epidemiologically, these fractures demonstrate a bimodal distribution. In pediatric patients, they typically occur between ages 9 and 14, often associated with sports-related trauma, particularly in throwing athletes. The unossified apophysis remains a cartilaginous weak point until fusion, making it susceptible to avulsion forces. In adults, medial epicondyle fractures are generally less common as an isolated injury, but can occur with high-energy trauma or severe elbow dislocations. The incidence is higher in athletes participating in overhead or throwing sports, where repetitive valgus stress and acute tensile forces can lead to avulsion injuries or chronic apophysitis, famously known as Little League elbow. The consequences of untreated or inadequately managed displaced medial epicondyle fractures can be profound, leading to chronic valgus instability, ulnar neuropathy, and persistent functional deficits, particularly for individuals with high-demand upper extremity activities.
Surgical Anatomy and Biomechanics
Medial Epicondyle Apophysis and Ossification
The medial epicondyle is a distinct bony prominence on the distal humerus, positioned posteromedially to the trochlea. In skeletally immature individuals, this region consists of a cartilaginous apophysis, which serves as a secondary ossification center. Ossification typically begins around 5 to 7 years of age in males and 4 to 6 years in females, with fusion to the metaphysis occurring between 14 and 16 years of age. This cartilaginous physis represents a relative weak point, predisposing it to avulsion injuries before skeletal maturity. In adults, the medial epicondyle is a robust bony structure, and fractures typically involve an osteochondral fragment.

Flexor Pronator Mass Origins
The medial epicondyle serves as the primary origin for the superficial and deep flexor-pronator musculature of the forearm. These muscles originate from the medial epicondyle and its surrounding fascial investments. Key muscles originating directly or indirectly from this region include:
* Pronator Teres (humeral head): A powerful forearm pronator and elbow flexor.
* Flexor Carpi Radialis (FCR): A wrist flexor and radial deviator.
* Palmaris Longus: A weak wrist flexor, variably present.
* Flexor Digitorum Superficialis (FDS): Primarily a flexor of the proximal interphalangeal joints, also contributes to wrist flexion.
* Flexor Carpi Ulnaris (FCU, humeral head): A powerful wrist flexor and ulnar deviator, with a crucial fascial investment providing a roof for the ulnar nerve.
The collective action of these muscles contributes significantly to forearm pronation and wrist/finger flexion, and their forceful contraction or sudden stretch can generate substantial tension on the medial epicondyle, leading to avulsion.

Ulnar Collateral Ligament Complex
The ulnar collateral ligament (UCL) complex is the primary static stabilizer of the elbow against valgus stress. It originates from the anteroinferior aspect of the medial epicondyle and inserts onto the sublime tubercle of the ulna. The UCL is comprised of three distinct bundles:
* Anterior Bundle: The strongest and most important component, providing primary valgus stability from 30 to 90 degrees of flexion. It consists of anterior and posterior bands.
* Posterior Bundle: Thickening of the joint capsule, less distinct, and provides secondary stability at extreme flexion.
* Transverse Bundle (Cooper's ligament): Connects the coronoid and olecranon, with little contribution to elbow stability.
In medial epicondyle fractures, especially avulsion types, the UCL typically remains attached to the fractured fragment. Disruption of the UCL's bony attachment significantly compromises elbow valgus stability.
Neurovascular Structures
The medial epicondyle region is in close proximity to vital neurovascular structures:
* Ulnar Nerve: The most critical neural structure, courses in the cubital tunnel posterior to the medial epicondyle. It is highly susceptible to injury during the fracture event, surgical approach, or as a late complication from fibrous scarring or hardware prominence.
* Medial Antebrachial Cutaneous Nerve (MACN): Branches of this sensory nerve cross the operative field and are at risk during skin incision and subcutaneous dissection, potentially leading to dysesthesias or paresthesias in the medial forearm.
* Superior Ulnar Collateral Artery: Courses with the ulnar nerve and can be a source of bleeding during deep dissection.
Biomechanical Considerations in Pathogenesis
Medial epicondyle fractures commonly result from an avulsion mechanism rather than a direct blow. A fall on an outstretched arm with simultaneous valgus stress to the elbow and contraction of the flexor-pronator mass creates significant tensile forces across the medial epicondyle. This mechanism is particularly common in associated elbow dislocations, where the valgus moment during dislocation or spontaneous reduction exerts extreme tension on the UCL and attached flexor-pronator muscles. The avulsed fragment may then become incarcerated within the joint during spontaneous reduction of an elbow dislocation, a critical factor influencing management. Overuse in throwing athletes can lead to chronic microtrauma, apophysitis, or stress fractures, sometimes progressing to acute avulsion.
Indications and Contraindications
The decision-making process for the management of medial epicondyle fractures is nuanced, relying on factors such as fracture displacement, associated injuries, patient age, skeletal maturity, and functional demands. Open Reduction and Internal Fixation (ORIF) is typically reserved for cases where non-operative management is unlikely to yield a stable, functional outcome.
Indications for Operative Intervention (ORIF)
- Significant Displacement: Generally, displacement exceeding 2 mm to 5 mm, depending on the patient's age and activity level. For skeletally immature patients and high-demand athletes, even 2 mm of displacement may be considered an indication due to concerns for nonunion or malunion and associated instability.
- Articular Incarceration: A fractured medial epicondyle fragment that is displaced and entrapped within the elbow joint, preventing concentric reduction of the elbow or leading to mechanical impingement. This is a common occurrence with associated elbow dislocations.
- Elbow Instability: Clinically demonstrable valgus instability of the elbow, particularly if associated with UCL disruption or an avulsed medial epicondyle fragment that includes the UCL origin. This can manifest as recurrent dislocations or chronic subjective instability.
- Open Fractures: Any open fracture warrants surgical debridement and fixation to prevent infection and facilitate healing.
- Multiple Trauma: In polytrauma patients, early stable fixation can aid in overall patient management and early mobilization.
- Delayed Presentation of Displaced Fractures: If a significantly displaced fracture is diagnosed late and non-operative management has failed or is contraindicated.
- High-Demand Athletes: Especially throwing athletes, where optimal anatomical reduction and stable fixation are paramount for restoring valgus stability and achieving pre-injury performance levels.
- Failure of Non-Operative Management: Progressive displacement or persistent instability despite an initial trial of conservative care.
Contraindications for Operative Intervention
- Minimally Displaced Fractures: Displacement less than 2 mm, provided the elbow is stable and there is no evidence of intra-articular incarceration.
- Non-Displaced or Stable Fractures: These are appropriately managed with immobilization and early rehabilitation.
- Severe Comminution: Extensive comminution of the fragment that precludes stable fixation may necessitate alternative strategies, although this is rare for the medial epicondyle.
- Active Infection: Absolute contraindication to elective internal fixation; requires infection control prior to definitive fracture management.
- Severe Medical Comorbidities: Patients with medical conditions that significantly increase the risks of general anesthesia and surgical intervention, outweighing the potential benefits of ORIF.
- Non-Ambulatory or Low-Demand Patients: In older, low-demand patients, if conservative management yields acceptable function, even moderate displacement may be tolerated.
Operative vs Non Operative Indications
| Feature | Operative Management (ORIF) | Non-Operative Management |
|---|---|---|
| Displacement | > 2-5 mm (varies by age/activity) | < 2 mm |
| Intra-articular Fragment | Present | Absent |
| Elbow Stability | Valgus instability present | Elbow stable to valgus stress |
| Associated Injuries | Associated elbow dislocation (especially irreducible) | Isolated fracture without significant ligamentous injury |
| Patient Profile | High-demand athlete, pediatric patient with potential for growth | Low-demand patient, non-dominant arm, skeletally mature |
| Fracture Type | Open fracture, avulsion with significant soft tissue involvement | Simple, closed, stable fracture |
| Ulnar Nerve Symptoms | Acute onset ulnar neuropathy potentially related to displacement | Mild, transient symptoms not clearly related to fragment |
Pre Operative Planning and Patient Positioning
Thorough pre-operative planning is paramount for successful outcomes in medial epicondyle fractures, encompassing comprehensive imaging review, patient optimization, and meticulous surgical setup.
Imaging Modalities
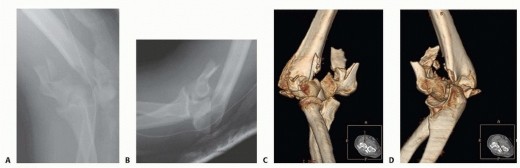
- Plain Radiographs: Standard anteroposterior, lateral, and oblique views of the elbow are essential. The AP view is crucial for assessing medial displacement, while the lateral view helps identify posterior displacement or rotation. Oblique views, particularly the internal oblique, can provide better visualization of the fragment and its relationship to the joint.
- Computed Tomography (CT) Scan: Indicated for complex fracture patterns, significant displacement, or suspicion of intra-articular incarceration, especially when plain films are equivocal. CT provides detailed information on fragment size, comminution, and precise location within the joint, aiding in surgical strategy.
- Magnetic Resonance Imaging (MRI): While not routine, MRI can be valuable for assessing associated soft tissue injuries, such as UCL tears, collateral ligament integrity, or chondral damage, particularly in cases of chronic instability or when surgical exploration of the ligaments is anticipated. It can also differentiate between acute fracture and chronic apophysitis.
Patient Preparation and Assessment
A comprehensive medical evaluation is necessary to address any comorbidities. Hand dominance and the patient's activity level (e.g., throwing athlete) must be considered when discussing prognosis and functional goals. A detailed neurological examination, focusing on the ulnar nerve, is critical pre-operatively to document any pre-existing deficits and establish a baseline. Assessment of skin integrity and any signs of impending compartment syndrome should also be performed.
Patient Positioning and Surgical Setup
The patient is typically positioned supine on the operating table, with the involved arm draped free onto a hand table. Alternatively, a lateral decubitus position may be utilized to allow for easier access to the medial aspect of the elbow.
* Tourniquet Application: A pneumatic tourniquet is applied high on the upper arm for a bloodless field, typically inflated to 250-300 mmHg.
* Arm Preparation: The entire arm, from the shoulder to the hand, is prepped and draped to allow for full range of motion of the elbow during surgery, essential for assessing stability and reduction.
* Fluoroscopy: A C-arm fluoroscope should be readily available and positioned to allow for intraoperative imaging in multiple planes (AP, lateral, oblique) without repositioning the patient.
* Ulnar Nerve Protection: Pre-operative padding of the ulnar nerve at the contralateral elbow and careful positioning of the affected arm to prevent iatrogenic nerve compression are crucial.
* Instrumentation: A small fragment screw set, mini-fragment set, K-wires, suture anchors, and standard orthopedic surgical instruments should be prepared.
Detailed Surgical Approach and Technique
The goal of surgical intervention for medial epicondyle fractures is anatomical reduction of the fragment, stable internal fixation, restoration of valgus stability, and preservation of ulnar nerve function.
Anesthesia and Incision
General anesthesia or regional blockade (e.g., supraclavicular block) can be employed. The preferred incision is a longitudinal or slightly curvilinear incision centered over the medial epicondyle.
* Incision: Typically, a 5-8 cm longitudinal incision starts proximal to the medial epicondyle, curves anteriorly around the epicondyle, and extends distally along the medial forearm. This allows for adequate exposure and facilitates identification and protection of the ulnar nerve and its branches.
* Superficial Dissection: The skin and subcutaneous tissues are incised. Careful attention is paid to identifying and protecting branches of the medial antebrachial cutaneous nerve, which cross the field and are highly susceptible to iatrogenic injury. These small sensory nerves should be gently retracted or carefully dissected and ligated if absolutely necessary, though preservation is preferred.
Ulnar Nerve Identification and Management
The ulnar nerve is the most critical structure to identify and protect during this approach.
* Identification: The cubital tunnel, located posterior to the medial epicondyle, is palpated. The ulnar nerve typically courses between the medial epicondyle and the olecranon. It is crucial to identify the nerve early in the dissection, tracing it proximally and distally. The roof of the cubital tunnel, formed by Osborne's ligament (flexor carpi ulnaris aponeurosis), is incised to decompress the nerve.
* Decision for Transposition: A critical intraoperative decision is whether to perform an anterior transposition of the ulnar nerve. This is indicated if:
* The nerve is unstable in its groove after fracture reduction.
* Significant pre-existing ulnar nerve symptoms are present.
* The fracture fragment is large, requiring extensive dissection in the cubital tunnel.
* Hardware placement may impinge on the nerve.
If transposed, the nerve is gently mobilized from its bed and moved anteriorly, usually beneath the flexor-pronator mass (submuscular) or subcutaneously. Simple decompression may be sufficient if the nerve is stable and asymptomatic.

Exposure of the Fracture Fragment
- Flexor-Pronator Mass Dissection: After identification and protection of the ulnar nerve, the origin of the common flexor-pronator mass is identified. This mass typically remains attached to the avulsed medial epicondyle fragment. A subperiosteal dissection is performed, lifting the flexor-pronator musculature anteriorly from the distal humerus to expose the fracture site. Care is taken to stay close to the bone to avoid injury to deeper structures.
- Fragment Identification: The fracture fragment, which includes the epicondyle, the origin of the flexor-pronator mass, and the attachment of the UCL, is identified. If the fragment is incarcerated within the joint (often between the trochlea and olecranon), the elbow joint capsule may need to be incised to allow retrieval. A nerve hook or small blunt instrument can be used to gently extract the incarcerated fragment.

Fracture Reduction
- Direct Reduction: The fracture fragment is directly visualized and manipulated back to its anatomical position on the distal humerus. This often requires gentle traction on the attached flexor-pronator mass. The reduction should be concentric and restore the smooth contour of the medial epicondyle.
- Temporary Fixation: Once anatomical reduction is achieved, it is temporarily secured with one or two small K-wires. These K-wires should be placed obliquely and carefully to avoid future fixation sites and articular surfaces. Intraoperative fluoroscopy confirms satisfactory reduction in AP and lateral planes.
Internal Fixation
Stable internal fixation is crucial to allow for early mobilization and prevent nonunion or malunion. The choice of fixation depends on the fragment size, bone quality, and surgeon preference.
* Screw Fixation: For adequately sized fragments, partially threaded cancellous screws (typically 2.7 mm, 3.5 mm, or 4.0 mm) are often preferred.
* Lag Screw Principle: The screws are inserted in a lag fashion, perpendicular to the fracture plane, to achieve interfragmentary compression. This involves overdrilling the near cortex (or the epicondyle fragment) and underdrilling the far cortex (humeral metaphysis), followed by tapping and screw insertion.
* Screw Placement: One to two screws are typically sufficient. They should be placed to achieve maximal compression and stability, avoiding the articular surface and the ulnar nerve.
* Tension Band Wiring: For smaller or comminuted fragments, or when strong traction forces are anticipated, tension band wiring can be an effective alternative or adjunct. This technique converts tensile forces into compressive forces at the fracture site. K-wires are placed across the fracture, and a cerclage wire is then looped around the K-wires and tightened.
* Suture Anchors: In cases of pure avulsion where the bone fragment is extremely small or mostly cartilaginous, suture anchors can be used to reattach the soft tissue (UCL and flexor-pronator origin) directly to the medial epicondyle or distal humerus. This is particularly relevant in pediatric avulsions where the bone fragment is minimal.
* Stability Assessment: After fixation, the elbow is put through a full range of motion, and valgus stress is applied to confirm stability. There should be no gapping at the fracture site or clinical evidence of valgus instability. The ulnar nerve should also be reassessed for any signs of impingement by hardware or soft tissue.

Closure
- Layered Closure: After confirming stable fixation and satisfactory ulnar nerve status, the wound is irrigated. The flexor-pronator mass is reapproximated over the fracture site. The subcutaneous tissue and skin are closed in layers.
- Ulnar Nerve Position: If the ulnar nerve was transposed, its new stable position should be confirmed. If it was simply decompressed, ensure it lies freely in its groove without tension or impingement.
- Dressings: A sterile dressing is applied, and the elbow is typically immobilized in a posterior splint or hinged elbow brace at 90 degrees of flexion with the forearm in neutral rotation.
Complications and Management
Despite meticulous surgical technique, complications can arise following open reduction and internal fixation of medial epicondyle fractures. Proactive recognition and appropriate management are crucial for optimizing patient outcomes.
Common Complications and Salvage Strategies
| Complication | Incidence (Approximate) | Pathophysiology / Presentation | Management / Salvage Strategy |
|---|---|---|---|
| Ulnar Neuropathy | 10-25% | Iatrogenic injury, traction, compression by hardware/scar tissue, persistent instability. Presents as paresthesia/dysesthesia in small/ring fingers, intrinsic muscle weakness. | Prevention: Meticulous dissection, careful retraction, routine nerve identification/decompression/transposition if indicated. Management: Observation for mild, transient symptoms. Neurolysis (surgical release) for persistent/worsening symptoms. Revision anterior transposition if unstable or compressed by hardware. |
| Nonunion / Malunion | 5-15% | Inadequate reduction, unstable fixation, biological factors, chronic apophysitis. Presents as persistent pain, deformity, instability, or loss of motion. | Management: For asymptomatic, stable nonunion, observation. For symptomatic nonunion: revision ORIF with debridement of fibrous tissue, bone grafting (autograft/allograft), and more robust fixation. Malunion may require corrective osteotomy if significantly symptomatic or causing impingement. |
| Elbow Stiffness / ROM Loss | 15-30% | Prolonged immobilization, heterotopic ossification, capsular contracture, articular damage. Presents as limited flexion/extension or pronation/supination. | Prevention: Early, controlled range of motion (ROM) initiated post-operatively per rehabilitation protocol. Management: Aggressive physical therapy, dynamic/static progressive splinting. Manipulation Under Anesthesia (MUA) for intractable stiffness. Arthroscopic or open arthrolysis for severe capsular contracture or heterotopic ossification. |
| Hardware-Related Issues | 10-20% | Prominence causing pain/irritation, migration, breakage. | Management: Hardware removal after fracture healing is complete, typically 6-12 months post-op, if symptomatic. In rare cases of hardware breakage with nonunion, revision fixation may be required. |
| Infection | 1-5% | Superficial or deep wound infection. Presents with pain, erythema, swelling, warmth, drainage, fever. | Prevention: Strict sterile technique, appropriate prophylactic antibiotics. Management: Superficial infections typically respond to oral antibiotics. Deep infections require surgical irrigation and debridement, intravenous antibiotics, and potentially hardware removal (once fracture is stable or in cases of septic nonunion). |
| Chronic Valgus Instability | < 5% (post-ORIF) | Inadequate primary repair of UCL, failed healing of epicondyle fragment (nonunion), inadequate fixation, associated ligamentous injuries not addressed. | Management: Physiotherapy for dynamic stability. For persistent symptomatic instability in high-demand patients, revision surgery for UCL reconstruction (e.g., "Tommy John" surgery) using autograft (palmaris longus or gracilis tendon) may be necessary, often coupled with addressing any underlying bony nonunion or malreduction. |
| Growth Disturbances (Pediatric) | Rare | Premature physeal closure, physeal arrest, angular deformity. | Prevention: Careful K-wire/screw placement to avoid traversing the physis unnecessarily or causing compression. Management: Observation for minor disturbances. Corrective osteotomy for significant angular deformity if symptomatic and affecting function. |
Post Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is crucial following surgical repair of medial epicondyle fractures to restore optimal elbow function, stability, and range of motion while protecting the healing fracture and soft tissue repair. The protocol must be individualized based on the stability of fixation, patient age, concomitant injuries, and functional goals.
Phase 1: Immediate Post-Operative Period (Weeks 0-4)
- Goals: Control pain and swelling, protect the surgical repair, maintain range of motion in adjacent joints (shoulder, wrist, hand), and initiate controlled elbow motion.
- Immobilization: The elbow is typically placed in a posterior splint or a hinged elbow brace, maintaining approximately 90 degrees of flexion with the forearm in neutral rotation. This provides protection while allowing for controlled initiation of movement.
- Pain Management: Opioids, NSAIDs, and cryotherapy are utilized.
- Early Motion:
- Day 1-7: Active-assisted and passive range of motion (AAROM/PROM) exercises for elbow flexion and extension are initiated within a protected arc (e.g., 30-90 degrees, gradually expanding as tolerated). Forearm pronation and supination are also started, avoiding excessive stress on the medial epicondyle.
- Precautions: Absolutely no active valgus stress or resisted forearm pronation/wrist flexion is permitted. The hinged brace typically locks out valgus stress. Patient education on proper body mechanics and avoiding lifting or carrying with the affected arm is critical.
- Adjunctive Therapy: Gentle scar massage, edema control, and light isometric exercises for the shoulder and hand (e.g., grip strengthening) are encouraged.
Phase 2: Intermediate Strengthening (Weeks 4-10)
- Goals: Gradually increase elbow range of motion, initiate light strengthening, and prepare for functional activities.
- Progression of Motion: The range of motion in the hinged brace is progressively increased as healing permits, aiming for full flexion and extension by the end of this phase.
- Strengthening:
- Low-resistance isotonic exercises: Gentle concentric and eccentric exercises for elbow flexion/extension (e.g., bicep curls, tricep extensions) and forearm pronation/supination.
- Initiate light flexor-pronator strengthening: Very light resistance, focusing on endurance and control, avoiding high-impact or sudden, forceful contractions.
- Scapular stabilization exercises: Crucial for overall upper extremity kinetic chain.
- Functional Activities: Gradual reintroduction of light daily living activities. Avoid heavy lifting, carrying, or activities involving significant valgus stress.
- Ulnar Nerve Considerations: If ulnar nerve transposition was performed, specific nerve gliding exercises may be incorporated.
Phase 3: Advanced Strengthening and Return to Activity (Weeks 10-24+)
- Goals: Restore full strength, power, and endurance; return to sport-specific or high-demand occupational activities.
- Intensified Strengthening: Progressive resistance exercises for all major elbow and forearm muscle groups, including the flexor-pronator mass. Advanced core and scapular strengthening.
- Sport-Specific Training (for athletes):
- Interval throwing programs: For throwing athletes, a highly structured, gradual return to throwing is initiated, beginning with short distances and low intensity, progressively increasing velocity and distance. This often involves a multi-month progression.
- Valgus Stress Conditioning: Controlled, progressive exercises that simulate sport-specific valgus stresses, carefully monitored.
- Proprioception and Neuromuscular Control: Exercises to improve joint awareness and dynamic stability.
- Return to Activity: Full return to unrestricted activities is typically not permitted until 4-6 months post-operatively, depending on the severity of the injury, healing progress, and the demands of the patient's sport or occupation. Clinical and radiographic healing must be confirmed. The absence of pain, full range of motion, and symmetrical strength are prerequisites.
Summary of Key Literature and Guidelines
The management of medial epicondyle fractures has evolved significantly, particularly with advances in surgical techniques and a deeper understanding of elbow biomechanics. Consensus guidelines emphasize the importance of accurate diagnosis, assessment of elbow stability, and individualized treatment plans.
Historical literature often highlighted the potential for nonunion and functional deficits in displaced medial epicondyle fractures, especially in skeletally immature patients. Studies by Fowles et al. (1990) and others demonstrated that a significant percentage of displaced fractures treated non-operatively can result in symptomatic nonunion, elbow stiffness, or valgus instability, particularly if the fragment is incarcerated. This evidence strongly supports surgical intervention for significantly displaced or incarcerated fragments.
Current literature broadly supports the following principles:
* Displacement Thresholds: While precise displacement thresholds vary slightly across studies, the general consensus for operative intervention in pediatric patients and high-demand athletes ranges from 2-5 mm. For stable, minimally displaced fractures (<2mm) without incarceration, non-operative management with early controlled motion remains the standard.
* Role of Associated Dislocation: The strong association between medial epicondyle fractures and elbow dislocations is a critical consideration. The incidence of fragment incarceration within the joint following elbow dislocation is well-documented, necessitating surgical reduction and fixation to restore concentric joint articulation and prevent mechanical impingement.
* Ulnar Nerve Management: Ulnar nerve involvement is the most common complication. Routine intraoperative identification and protection are standard. The debate surrounding routine anterior ulnar nerve transposition versus simple decompression continues. While some advocate for routine transposition, others reserve it for cases of pre-existing symptoms, nerve instability, or anticipated hardware impingement. Evidence suggests that careful in-situ decompression with protection is often sufficient, with transposition reserved for specific indications.
* Fixation Techniques: Both screw fixation (lag screw principle) and tension band wiring are well-established and effective methods for stable internal fixation, depending on fragment morphology. Suture anchors offer a viable option for avulsion injuries with minimal bone, particularly in adolescents.
* Rehabilitation: Modern protocols emphasize early, controlled range of motion to prevent stiffness while protecting the healing repair. Prolonged immobilization is generally discouraged, as it correlates with increased stiffness and prolonged recovery. Gradual progression to strengthening and sport-specific activities is key, with return to play criteria focusing on strength, pain absence, and functional performance rather than arbitrary timelines.
Ongoing research continues to refine surgical indications, fixation strategies, and rehabilitation protocols. The long-term outcomes for appropriately managed medial epicondyle fractures are generally excellent, especially with anatomical reduction, stable fixation, and adherence to progressive rehabilitation. However, complications such as ulnar neuropathy and stiffness remain a concern, underscoring the importance of meticulous surgical technique and comprehensive post-operative care.
You Might Also Like