Subtrochanteric Fractures & Hip Dislocations: Surgical Guide

Key Takeaway
Subtrochanteric femoral fractures and hip dislocations represent complex, high-energy orthopedic traumas requiring meticulous surgical intervention. This guide details the step-by-step operative technique for 95-degree blade plate fixation, emphasizing precise preoperative templating, chisel seating, and rotational alignment. Furthermore, it outlines the critical diagnostic and reduction protocols for posterior and anterior hip dislocations to mitigate osteonecrosis and manage associated femoral head fractures effectively.
INTRODUCTION TO PROXIMAL FEMORAL TRAUMA
The management of high-energy proximal femoral trauma demands a profound understanding of local biomechanics, precise surgical execution, and rigorous postoperative protocols. Subtrochanteric femoral fractures and traumatic hip dislocations represent two of the most challenging entities in orthopedic traumatology. The subtrochanteric region is subjected to the highest biomechanical stresses in the human body, necessitating robust fixation constructs such as the 95-degree angled blade plate. Concurrently, traumatic hip dislocations, often accompanied by femoral head fractures, require emergent intervention to preserve the vascularity of the femoral head and mitigate the devastating complication of osteonecrosis.
This comprehensive masterclass details the operative techniques, biomechanical principles, and evidence-based management strategies for these complex injuries, tailored for the practicing orthopedic consultant and advanced surgical fellow.
FIXATION OF SUBTROCHANTERIC FEMORAL FRACTURES WITH A BLADE PLATE
Biomechanics and Deforming Forces
The subtrochanteric region of the femur is defined as the area extending from the lesser trochanter to approximately 5 cm distally into the proximal femoral shaft. This zone is characterized by thick cortical bone and is subjected to massive compressive forces medially and tensile forces laterally.
Fractures in this region are notoriously difficult to reduce and hold due to the powerful deforming forces exerted by the surrounding musculature:
* Proximal Fragment: Flexed by the iliopsoas, abducted by the gluteus medius and minimus, and externally rotated by the short external rotators.
* Distal Fragment: Adducted by the adductor magnus, longus, and brevis, and proximally migrated (shortened) by the hamstrings and quadriceps.
While cephalomedullary nailing has become the workhorse for many subtrochanteric fractures, the 95-degree angled blade plate remains an indispensable tool, particularly for fractures with proximal extension into the greater trochanter, corrective osteotomies, and the management of nonunions.
Preoperative Planning and Templating
Preoperative planning for the placement of a blade plate is extremely important and cannot be overstated. The margin for error with a fixed-angle device is minimal.
Clinical Pearl: Even with the advent of advanced computerized digital templating, we strongly advocate using printed radiographs to create an accurate, tactile template. The exact entry point, the angle of the seating chisel, and the length of the blade must be determined preoperatively to restore the mechanical axis and prevent varus collapse.
Patient Positioning and Setup
- Position the patient supine on a radiolucent fracture table.
- Apply traction via a skeletal pin or a well-padded traction boot.
- Ensure the C-arm fluoroscope can freely obtain perfect anteroposterior (AP) and lateral views of the proximal femur and hip joint without obstruction.
- Prep and drape the entire hemipelvis and lower extremity to allow for intraoperative adjustments.
Surgical Approach
Make a standard lateral exposure of the proximal femur. This is similar to the exposure used for the placement of a proximal femoral locking plate, but the incision must be extended significantly farther distally.
* Incise the fascia lata in line with the skin incision.
* Elevate the vastus lateralis off the intermuscular septum, or utilize a subvastus approach depending on the fracture morphology.
* Ensure the incision is as long as the anticipated plate length to avoid excessive soft tissue tension during plate application.
Step-by-Step Surgical Technique
1. Guide Wire Placement
Insert a Kirschner wire (K-wire) into the lateral aspect of the proximal femur at a precise 95-degree angle relative to the femoral shaft. This trajectory must be based strictly on your preoperative templating. Evaluate the position of the K-wire and the anteversion of the hip in both the AP and lateral fluoroscopic planes.
2. Cortical Preparation
Use a 3.2-mm drill bit to prepare an entrance window for the seating chisel just distal to the K-wire in the lateral cortex. This prevents the chisel from splitting the lateral cortex during insertion.
3. Chisel Seating
Advance the seating chisel into the lateral aspect of the femur and into the femoral neck, using the previously placed K-wire as a parallel guide.
Surgical Warning: Make sure the chisel is continually oriented to the alignment of the proximal fragment. You must completely disregard the orientation of the distal fragment at this stage.
Withdraw the chisel every 10 to 15 mm during advancement. Failure to do so will result in the incarceration of the seating chisel within the dense cancellous bone of the femoral neck, making extraction exceedingly difficult and risking iatrogenic fracture. Advance the chisel to the appropriate depth determined from preoperative templating.
4. Blade Plate Insertion and Fracture Reduction
Remove the chisel and introduce the blade plate. Once the blade is fully seated within the proximal fragment, use the plate as a lever to reduce the fracture to the femoral shaft.
Bone-holding forceps (e.g., Verbrugge or reduction clamps) can be used to provisionally reduce the plate to the bone distally. Insert an eccentrically placed screw first to achieve dynamic compression. If the compression provided by this screw is insufficient, an articulating tensioner should be applied to the distal end of the plate.
FIGURE 55-47: Malalignment from a suboptimal portal can be corrected by the addition of an anterior-to-posterior blocking screw (Poller screw) to direct the trajectory of the implant and maintain reduction.
Alternative Fixation: Proximal Femoral Locking Plates
In cases where the fracture extends proximally into the piriformis fossa or greater trochanter, a proximal femoral locking plate may be utilized as an alternative to the blade plate.

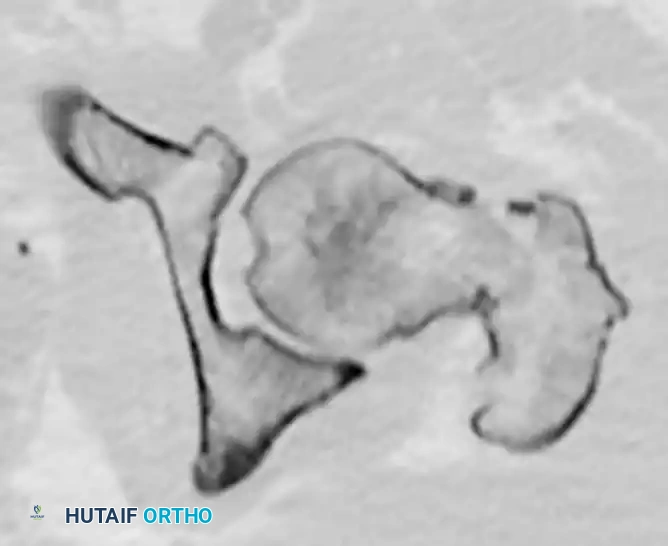


FIGURE 55-48: Proximal femoral locking plate fixation of a subtrochanteric femoral fracture with proximal extension. (A) Preoperative radiograph. (B) Preoperative axial CT scan shows extension proximally into the piriformis fossa. (C and D) Postoperative AP and lateral radiographs after fixation with a locking plate.
Management of Subtrochanteric Nonunions
The blade plate is particularly advantageous in the management of subtrochanteric nonunions, where rigid, fixed-angle stability is required to promote osteogenesis.



FIGURE 55-49: Fixation of a subtrochanteric nonunion with a blade plate. (A) Preoperative radiograph demonstrating hypertrophic nonunion. (B and C) Postoperative radiographs after rigid fixation and compression with a blade plate.
Assessment of Rotational Alignment
Evaluating rotation is a critical step before final fixation. Any rotational abnormality can be corrected by removing the distal screws, manually correcting the rotational deformity, and reinserting the screws.
Careful evaluation of rotation is paramount because the proximal segment is typically externally rotated by the short rotators; however, it may have been inadvertently internally rotated during the reduction of the fracture and plate placement. Compare the fluoroscopic image of the affected side to the image of the contralateral side obtained at the beginning of the procedure.
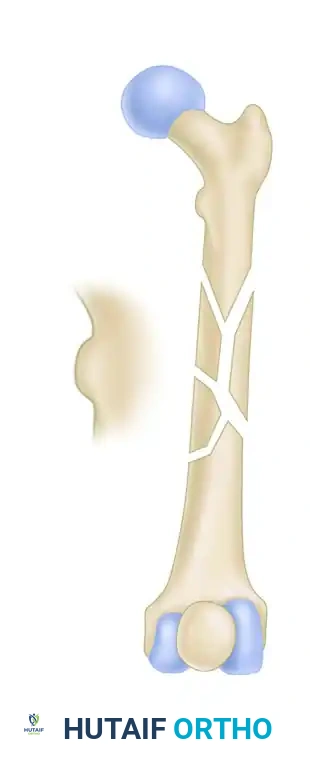
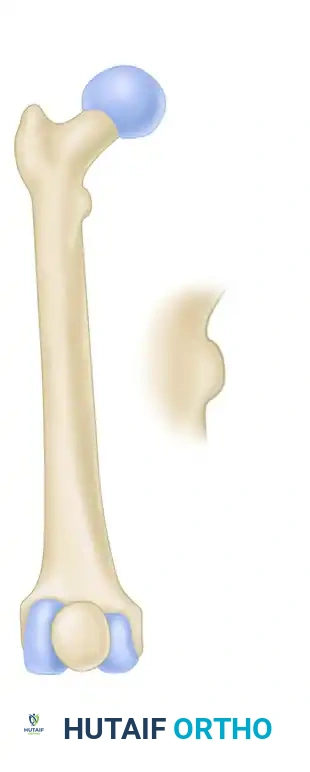
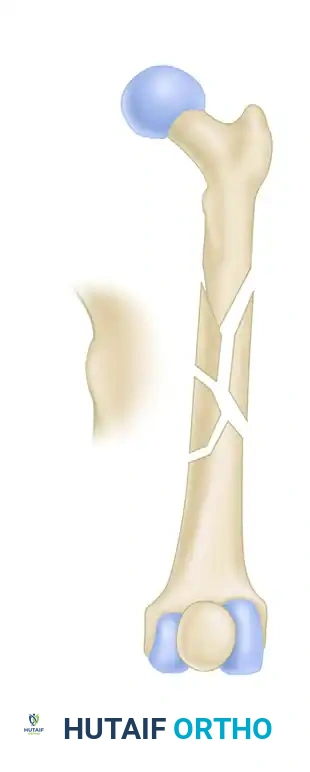
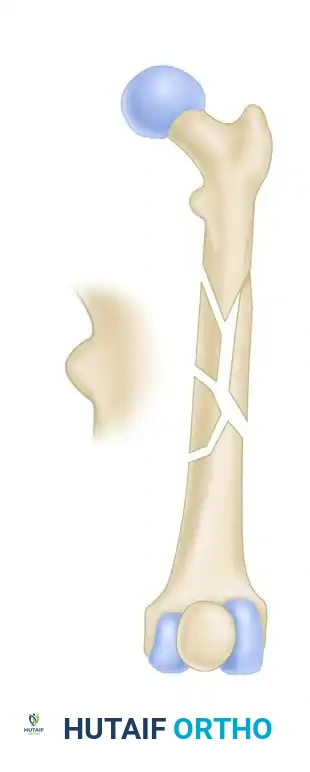
FIGURE 55-50: Rotation can be accurately assessed by comparing the contour and profile of the affected lesser trochanter to that of the contralateral, uninjured hip under fluoroscopy.
Final Fixation and Closure
- Place two or three additional screws in the femoral shaft to complete the final construct.
- The decision to use locking or nonlocking shaft screws is heavily influenced by the patient’s bone quality (e.g., locking screws are preferred in osteoporotic bone).
- Clinically evaluate limb length and rotation before the patient is awakened from anesthesia.
- After all screws are placed and hemostasis is achieved, close the incision in a standard, layered fashion.
Postoperative Care
Postoperative care requires strict adherence to weight-bearing restrictions to prevent hardware failure before bony union occurs. Touch-down weight bearing (TDWB) is allowed for the first 6 weeks. Weight-bearing status is subsequently advanced based on clinical examination and evidence of bridging callus on follow-up radiographs.
HIP DISLOCATIONS AND FEMORAL HEAD FRACTURES
Mechanism of Injury and Associated Pathologies
Hip dislocations and femoral head fractures typically result from high-energy mechanisms, with motor vehicle accidents (MVAs) being the most common etiology (the classic "dashboard injury"). The immense force required to dislocate the native hip joint frequently results in concomitant injuries.
Clinical Pitfall: Never evaluate a dislocated hip in isolation. One study noted an 89% incidence of an ipsilateral knee pathological process (e.g., PCL tear, patellar fracture) on MRI evaluation following a hip dislocation.
A high index of suspicion is necessary to avoid missing knee injuries and injuries to other areas of the body. Associated systemic injuries (head, chest, abdomen) have been documented in 40% to 75% of patients. Furthermore, sciatic nerve injuries (specifically the peroneal division) are common with posterior hip dislocations, documented in 10% to 15% of patients. A thorough neurological examination must be documented prior to any reduction attempt.
Clinical Presentation
The clinical presentation of the injured limb provides immediate, vital information regarding the likely type and direction of the hip dislocation:
- Posterior Dislocations (Most Common): The injured extremity presents as shortened, internally rotated, and adducted.
- Anterior Dislocations (< 10%): The limb presents as shortened, externally rotated, and slightly abducted.
- Pure Hip Dislocation with Femoral Head Fracture: This rare injury pattern presents uniquely with slight hip and knee flexion and neutral hip rotation. Mehta and Routt described this specific injury pattern and issued strict warnings about the severe consequences of attempted closed reduction, which can cause further displacement of the head fragment or iatrogenic damage to the articular cartilage.
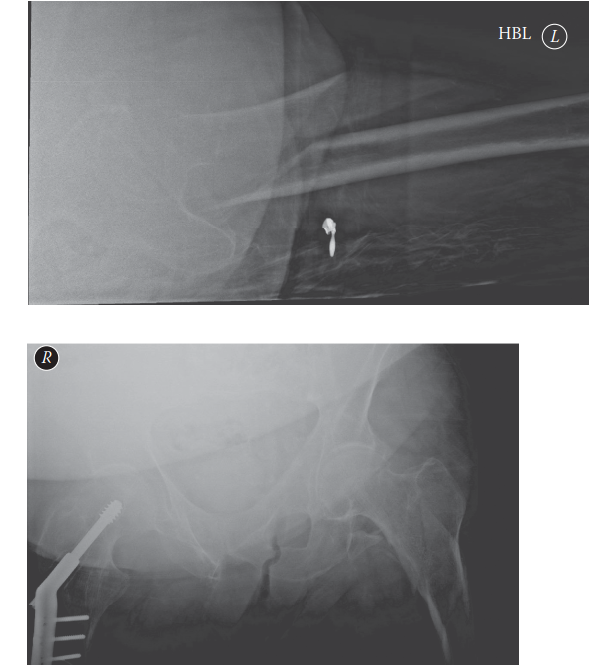
Radiographic Evaluation
The evaluation of a patient with a suspected hip dislocation must be expedited. Begin with an immediate anteroposterior (AP) pelvic radiograph before any attempt at reduction.
Analyze the radiograph for the following:
1. Size of the Femoral Head: With a posterior dislocation, the femoral head typically appears smaller (due to magnification differences as it sits closer to the cassette). With an anterior dislocation, the femoral head typically appears larger.
2. Projection of the Lesser Trochanter: In posterior dislocations, the lesser trochanter may not be seen because of the internal rotation of the extremity. In anterior dislocations, the lesser trochanter may be seen in its entirety due to external rotation.
3. Concentricity: Loss of concentricity of the femoral head with the acetabulum confirms the dislocation. Look closely for associated posterior wall acetabular fractures.
Principles of Closed Reduction and Osteonecrosis Mitigation
A pure hip dislocation is an orthopedic emergency and should be reduced as soon as possible to minimize the risk of osteonecrosis (AVN) of the femoral head. The risk of osteonecrosis clearly increases with increasing time to reduction, complicating 1% to 22% of posterior hip dislocations.
Surgical Warning: Multiple attempts at closed reduction should be strictly avoided to minimize the risk of iatrogenic damage to the femoral head cartilage and further vascular compromise. If one or two well-executed closed reduction attempts (e.g., Allis maneuver, Captain Morgan technique) fail, emergent open reduction in the operating room is mandated.
The decision regarding the location of the reduction (Emergency Department under procedural sedation vs. Operating Room under general anesthesia) should be based on the resources of the individual hospital, the patient's fasting status, and the presence of associated injuries.
Post-Reduction Management and Surgical Indications
Immediately following a successful closed reduction, repeat plain films (AP pelvis, Judet views) and a fine-cut CT scan of the pelvis must be obtained.
The CT scan is critical for evaluating:
* Concentricity of the reduction.
* Presence of intraarticular fragments (osteochondral loose bodies).
* Associated acetabular wall or column fractures.
* Femoral head fractures (Pipkin classification).
Indications for Surgical Intervention:
Intraarticular fragments from either the posterior wall or the femoral head that result in an incongruous reduction are an absolute indication for surgical treatment.
Patients with incongruous hip joints secondary to intraarticular fragments after closed reduction should be placed in distal femoral skeletal traction to prevent mechanical abrasion of the articular cartilage by the loose bodies. The exact size and location of these intraarticular fragments are evaluated on the CT scan. Patients are then treated with surgical debridement and fixation (via a Kocher-Langenbeck or surgical dislocation approach) on an emergency or urgent basis, depending on the size of the fragment and the patient’s overall hemodynamic condition.
📚 Medical References
- Subtrochanteric femoral fractures in children: alignment after 90 degrees-90 degrees traction and cast application, Clin Orthop Relat Res 341:170, 1997.
- Kasser JR: Femur fractures in children, Instr Course Lect 41:403, 1992.
- Kesemenli CC, Subasi M, Arslan H, et al: Is external fi xation in pediatric femoral fractures a risk factor for refracture, J Pediatr Orthop 24:17, 2004.
- Kiely N: Mechanical properties of different combinations of fl exible nails in a model of a pediatric femoral fracture, J Pediatr Orthop 22:424, 2002.
- Kirby RM, Winquist RA, Hansen ST Jr: Femoral shaft fractures in adolescents, comparison between traction plus cast treatment and closed intramedullary nailing, J Pediatr Orthop 1:193, 1981.
- Kissel EW, Miller ME: Closed-ended nailing of femur fractures in older children, J Trauma 29:1585, 1989.
- Langenskiöld A: An operation for partial closure of an epiphyseal plate in children and its experimental basis, J Bone Joint Surg 57B:325, 1975.
- Large TM, Frick SL: Compartment syndrome of the leg after treatment of a femoral fracture with an early sitting spica cast: a report of two cases, J Bone Joint Surg 85A:2207, 2003.
- Lee SS, Mahar AT, Newton PO: Ender nail fi xation of pediatric femur fractures: a biomechanical analysis, J Pediatr Orthop 21:442, 2001.
- Letts M, Jarvis J, Lawton L, et al: Complications of rigid intramedullary rodding of femoral shaft fractures in children, J Trauma 52:504, 2002.
- Ligier JN, Metaizeau JP, Prevot J, et al: Elastic stable intramedullary nailing of femoral shaft fractures in children, J Bone Joint Surg 70B:74, 1988.
- Limbird TJ, Cramer KE: Pediatric lower extremity open fractures: treatment results and complications. Paper presented at the Fifty-seventh annual meeting of the American Academy of Orthopaedic Surgeons, Las Vegas, Feb 10, 1990.
- Litt R, Albassir A, Willems S, et al: Coxa vara: isolated growth of the greater trochanter: prevention and treatment, Acta Orthop Belg 56:310, 1990.
- Lombardo SJ, Harvey JP Jr: Fractures of the distal femoral epiphysis: factors infl uencing prognosis: a review of thirty-four cases, J Bone Joint Surg 59A:742, 1977.
- Mäkelä EA, Vainionpää S, Vihtonen K, et al: The effect of trauma to the lower femoral epiphyseal plate: an experimental study in rabbits, J Bone Joint Surg 70B:187, 1988.
- Mann DC, Weddington J, Davenport K: Closed Enders nailing of femoral shaft fractures in adolescents, J Pediatr Orthop 6:651, 1986.
- Martinez AG, Carroll NC, Sarwark JF, et al: Femoral shaft fractures in children treated with early spica cast, J Pediatr Orthop 11:712, 1991.
- Momberger N, Stevens P, Smith J, et al: Intramedullary nailing of femoral fractures in adolescents, J Pediatr Orthop 20:482, 2000.
- Morris S, Cassidy N, Stephens M, et al: Birth-associated femoral fractures: incidence and outcome, J Pediatr Orthop 22:27, 2002.
- Moseley CF: A straight-line graph for leg-length discrepancies, J Bone Joint Surg 59A:174, 1977.
- Narayanan UG, Hyman JE, Wainwright AM, et al: Complications of elastic stable intramedullary nail fi xation of pediatric femoral fractures, and how to avoid them, J Pediatr Orthop 24:363, 2004.
- Neer C, Cadman E: Treatment of fractures of the femoral shaft in children, JAMA 163:634, 1957.
- Newton PO, Mubarak SJ: Financial aspects of femoral shaft
You Might Also Like