Surgical Decompression of the Forearm, Hand, and Digits for Compartment Syndrome

Introduction and Epidemiology
Acute compartment syndrome (ACS) of the upper extremity represents a catastrophic orthopedic and vascular emergency characterized by critically elevated interstitial tissue pressure within a closed, unyielding osteofascial envelope. The fundamental pathophysiology is driven by the arteriovenous pressure gradient theory; as intracompartmental pressure rises, it surpasses the capillary venous outflow pressure, leading to venous congestion. This congestion further increases compartmental pressure, eventually exceeding capillary perfusion pressure, thereby halting microvascular flow. This initiates a devastating cascade of cellular hypoxia, anaerobic metabolism, and the generation of oxygen free radicals. If surgical decompression is not achieved expeditiously, irreversible myonecrosis and ischemic neuropathy ensue, culminating in Volkmann’s ischemic contracture, profound functional impairment, or limb loss.
While the anterior compartment of the lower leg is the most frequent site of ACS, the forearm and hand are highly susceptible, particularly following high-energy trauma. The true incidence is difficult to capture due to the heterogeneity of etiologies. However, classic triggers in the upper extremity include pediatric supracondylar humerus fractures (particularly Gartland Type III), both-bone forearm shaft fractures, high-energy distal radius fractures, severe crush injuries, and ischemia-reperfusion cascades following vascular repair.
Clinical presentation of acute compartment syndrome in the upper extremity, demonstrating a tense, swollen forearm with shiny, unyielding skin.
Non-fracture etiologies must also be considered, including prolonged limb compression (e.g., in obtunded patients), circumferential full-thickness burns, high-pressure injection injuries, extravasation of cytotoxic intravenous fluids, and coagulopathies. Given the complex, densely packed neurovascular and musculotendinous anatomy of the upper extremity, rapid clinical recognition and emergent fasciotomy are the absolute standard of care to preserve limb viability and function. The ischemic tolerance of peripheral nerves is approximately 2 to 4 hours before irreversible damage begins, while skeletal muscle can sustain up to 6 hours of ischemia before frank myonecrosis occurs. Therefore, the window for intervention is exceptionally narrow.
The pathophysiology of ischemia-reperfusion injury further complicates the clinical picture. When perfusion is restored either spontaneously or via surgical decompression, the sudden influx of oxygenated blood interacts with accumulated hypoxanthine, producing a massive surge of reactive oxygen species (ROS). These ROS induce lipid peroxidation of cell membranes, exacerbating cellular edema and potentially causing a secondary spike in compartmental pressures if the fascial release is inadequate.
Pathophysiologic cascade of acute compartment syndrome illustrating the cyclical nature of venous congestion, reduced arterial inflow, and progressive tissue ischemia.
Surgical Anatomy and Biomechanics
A profound understanding of the cross-sectional anatomy and fascial boundaries of the upper extremity is a prerequisite for executing an adequate surgical decompression. Failure to release a single involved compartment can lead to localized necrosis and catastrophic functional deficits.
Arm Compartment Anatomy
The brachium (upper arm) is divided into two distinct fascial compartments by the medial and lateral intermuscular septa, which extend from the brachial fascia to the humeral shaft.
- Anterior Compartment: Contains the biceps brachii, brachialis, and coracobrachialis muscles. It also houses the critical neurovascular bundle, including the brachial artery and median nerve, as well as the musculocutaneous nerve.
- Posterior Compartment: Contains the triceps brachii muscle and the radial nerve, which courses intimately along the spiral groove of the humerus.
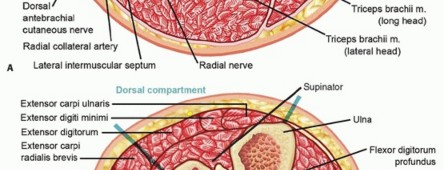
Cross-sectional anatomy of the upper arm demonstrating anterior and posterior compartments.
Forearm Compartment Anatomy
The forearm is anatomically unforgiving, comprising three primary fascial compartments: the volar (anterior), the dorsal (posterior), and the mobile wad of Henry (lateral).

Cross-sectional anatomy of the forearm, illustrating the volar, dorsal, and mobile wad compartments.
The volar compartment is the most frequently affected and is anatomically subdivided into superficial and deep layers. The superficial volar layer contains the pronator teres, flexor carpi radialis (FCR), palmaris longus (PL), flexor digitorum superficialis (FDS), and flexor carpi ulnaris (FCU). The deep volar layer contains the flexor digitorum profundus (FDP), flexor pollicis longus (FPL), and pronator quadratus. The deep volar compartment is particularly vulnerable to ischemia due to its tight fascial boundaries and proximity to the interosseous membrane. The median nerve courses between the FDS and FDP, making it highly susceptible to compression.

Detailed dissection of the superficial and deep volar forearm compartments, highlighting the course of the median nerve.
The dorsal compartment is similarly divided into superficial and deep layers. The superficial layer contains the extensor digitorum communis (EDC), extensor digiti minimi (EDM), and extensor carpi ulnaris (ECU). The deep layer houses the supinator, abductor pollicis longus (APL), extensor pollicis brevis (EPB), extensor pollicis longus (EPL), and extensor indicis proprius (EIP).
The mobile wad consists of the brachioradialis, extensor carpi radialis longus (ECRL), and extensor carpi radialis brevis (ECRB). While technically distinct, the mobile wad is often released concurrently with the dorsal or volar compartments depending on the surgical approach.

Anatomic boundaries of the mobile wad and dorsal compartments of the forearm.
Hand and Digit Compartment Anatomy
The hand is a highly complex structure containing ten distinct fascial compartments. Proper decompression requires a meticulous approach to address each potential space:
1. Dorsal Interosseous Compartments (Four): Containing the dorsal interossei muscles.
2. Volar Interosseous Compartments (Three): Containing the volar interossei muscles.
3. Thenar Compartment: Containing the abductor pollicis brevis, flexor pollicis brevis, and opponens pollicis.
4. Hypothenar Compartment: Containing the abductor digiti minimi, flexor digiti minimi brevis, and opponens digiti minimi.
5. Adductor Compartment: Containing the adductor pollicis.
Cross-sectional representation of the metacarpal level of the hand, delineating the ten intrinsic compartments.
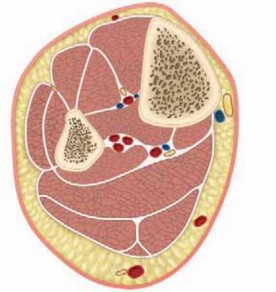
The digits themselves are compartmentalized by the volar skin, the flexor tendon sheath, and the fascial septa extending from the skin to the periosteum (Cleland's and Grayson's ligaments). While true compartment syndrome of the digits is rare, severe crush injuries or extravasation can necessitate digital fasciotomies to prevent localized necrosis and neurovascular compromise.
Cross-sectional anatomy of a digit, illustrating the neurovascular bundles and fascial septa.
Indications and Contraindications
The diagnosis of acute compartment syndrome is primarily clinical, augmented by intracompartmental pressure (ICP) monitoring in equivocal cases or in patients who are obtunded, intubated, or otherwise unable to provide a reliable clinical examination. The classic "6 Ps" (Pain out of proportion, Pallor, Paresthesias, Pulselessness, Paralysis, and Poikilothermia) are frequently cited; however, relying on the latter five is dangerous, as they represent late, often irreversible ischemic changes. Pain with passive stretch of the involved compartment remains the most sensitive early clinical indicator.
When clinical suspicion is high but definitive diagnosis is elusive, continuous or single-injection ICP monitoring is indicated. The absolute pressure threshold remains debated, but a differential pressure (Delta P) calculation is the widely accepted gold standard. Delta P is defined as the diastolic blood pressure minus the intracompartmental pressure (Delta P = Diastolic BP - ICP). A Delta P of less than 30 mmHg is an absolute indication for emergent fasciotomy.

Intracompartmental pressure measurement technique utilizing a solid-state transducer catheter in the volar forearm.
Contraindications to fasciotomy are limited but critically important. The primary contraindication is a "missed" compartment syndrome, typically defined as a presentation delayed beyond 24 to 48 hours with established, irreversible myonecrosis. In these late presentations, the muscle is already dead, and opening the fascial envelope exposes the necrotic tissue to nosocomial pathogens, significantly increasing the risk of life-threatening sepsis and inevitably leading to amputation. In such cases, observation with delayed reconstructive procedures or primary amputation is preferred.
| Clinical Scenario | Intervention Strategy | Rationale and Evidence Base |
|---|---|---|
| Clear Clinical Diagnosis (Awake Patient) | Emergent Operative Fasciotomy | Clinical signs (pain on passive stretch) are sufficient; delay for pressure testing is unwarranted and risks muscle death. |
| Obtunded/Intubated Patient at Risk | ICP Monitoring; Fasciotomy if Delta P < 30 mmHg | Unable to assess clinical symptoms; objective pressure data is mandatory to guide surgical intervention. |
| Equivocal Clinical Exam | ICP Monitoring; Serial Examinations | Prevents unnecessary morbidity of fasciotomy while ensuring ACS is not missed. Delta P < 30 mmHg mandates surgery. |
| Missed ACS (>48 hours, established necrosis) | Non-Operative (Observation) or Primary Amputation | Fasciotomy in established necrosis leads to severe infection. Contracture reconstruction or amputation is delayed until stable. |
| Prophylactic (e.g., Revascularization >6h) | Prophylactic Operative Fasciotomy | High risk of reperfusion injury and secondary ACS; preemptive release prevents irreversible ischemic damage. |
Algorithm for the diagnosis and management of acute compartment syndrome based on clinical findings and pressure monitoring.
Pre Operative Planning and Patient Positioning
Emergent surgical intervention leaves minimal time for extensive preoperative planning; however, a standardized approach ensures rapid and effective decompression. The surgical team must be assembled expeditiously, and blood products should be available if the etiology involves major trauma or vascular injury.
Anesthetic Considerations
General anesthesia is the modality of choice. Regional anesthesia (e.g., brachial plexus blocks) is generally contraindicated in patients at risk for compartment syndrome as it eliminates the ability to perform serial clinical examinations. If a patient already has a definitive diagnosis and is proceeding to the operating room, regional anesthesia may be used, but general anesthesia is preferred to avoid any masking of postoperative residual or recurrent compartment syndrome symptoms.
Patient Positioning and Setup
The patient is positioned supine with the affected upper extremity extended on a radiolucent hand table. A pneumatic tourniquet is routinely placed high on the brachium. The use of a tourniquet in the setting of ischemia is controversial. The standard recommendation is to avoid inflating the tourniquet unless massive, uncontrolled hemorrhage is encountered during the approach. If a tourniquet is utilized for initial visualization, it must be deflated prior to assessing muscle viability, as tourniquet-induced ischemia will mask the visual cues of reperfusion (muscle color, contractility, and bleeding).

Standard operating room setup for upper extremity fasciotomy, demonstrating the radiolucent hand table and high brachial tourniquet.
Equipment and Instrumentation
The surgical tray must include instruments for extensive soft tissue dissection and potential fracture stabilization if an underlying fracture is present. Standard equipment includes:
* Scalpels (No. 10 and No. 15 blades)
* Metzenbaum and Mayo scissors
* Fasciotomes or long dissecting scissors for blind fascial release (used with caution)
* Electrocautery
* Vessel loops and skin staples (for shoelace closure technique)
* Negative Pressure Wound Therapy (NPWT) systems

Essential instrumentation for upper extremity fasciotomy, including vessel loops for delayed primary closure techniques.
If an underlying fracture requires stabilization (e.g., both-bone forearm fracture), the necessary orthopedic hardware (plates, screws, external fixators) must be readily available in the room. Rigid skeletal stabilization is crucial to protect the soft tissues from further mechanical trauma and to facilitate postoperative wound care.
Detailed Surgical Approach and Technique
Surgical decompression of the upper extremity demands a systematic, anatomic approach to ensure all fascial compartments are completely released. Incomplete release is the most common cause of fasciotomy failure.
Forearm Volar Approach
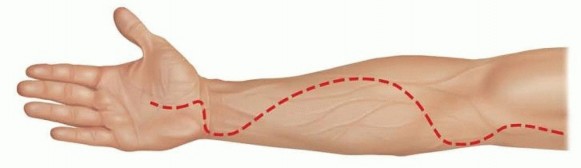
The volar compartment is decompressed using a curvilinear incision, classically described as the extended Henry approach or the McConnell modification. The incision begins proximal to the medial epicondyle, crosses the antecubital fossa obliquely to the mobile wad, extends distally along the volar forearm, and crosses the wrist crease obliquely to align with the carpal tunnel.
Marking of the curvilinear volar forearm incision, extending from the medial epicondyle across the wrist to the palmar crease.
- Incision and Superficial Dissection: The skin and subcutaneous tissue are incised. Care is taken to identify and protect the medial antebrachial cutaneous nerve proximally and the palmar cutaneous branch of the median nerve distally.
- Lacertus Fibrosus Release: Proximally, the bicipital aponeurosis (lacertus fibrosus) must be completely divided. This is a critical compression point for the brachial artery and median nerve.
- Superficial Fasciotomy: The superficial fascia of the volar forearm is incised longitudinally over the flexor carpi radialis (FCR) or between the FCR and flexor digitorum superficialis (FDS). The muscle bellies will typically bulge immediately upon release.
- Deep Fasciotomy: Releasing the superficial compartment does not adequately decompress the deep compartment. The surgeon must retract the FDS ulnarly and the FCR radially to expose the deep compartment (flexor digitorum profundus and flexor pollicis longus). The fascia overlying these deep muscles must be longitudinally incised. Epimysiotomies (incising the epimysium of individual muscle bellies) should be performed if the muscles remain tight after fascial release.
- Carpal Tunnel Release: The incision is extended distally across the wrist crease (avoiding a perpendicular crossing to prevent flexion contractures) and into the palm. The transverse carpal ligament is completely divided to decompress the median nerve within the carpal tunnel.

Intraoperative view following volar fasciotomy, demonstrating significant muscle bulging indicative of elevated intracompartmental pressure.
Forearm Dorsal Approach
While the volar incision decompresses the volar and mobile wad compartments, a separate dorsal incision is frequently required to address the dorsal compartments, especially in severe trauma.
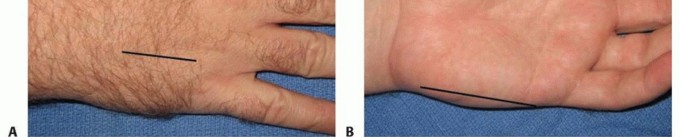
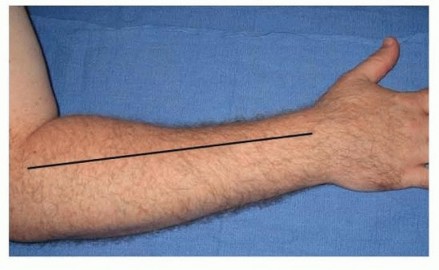
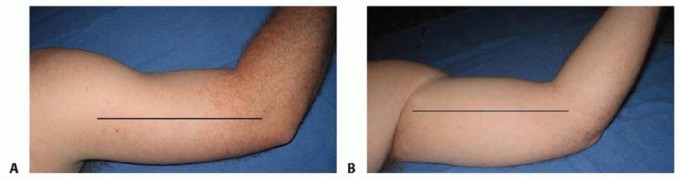
- Incision: A straight longitudinal incision is made from the lateral epicondyle to the midline of the dorsal wrist (Lister's tubercle).
- Fascial Release: The subcutaneous tissues are divided, protecting superficial draining veins where possible. The dorsal antebrachial fascia is incised longitudinally.
- Deep Dorsal Release: The interval between the extensor digitorum communis (EDC) and the extensor carpi radialis brevis (ECRB) is developed to access the deep dorsal compartment (supinator and outcropping muscles of the thumb). The fascia over these deep muscles is released.
Dorsal forearm fasciotomy utilizing a straight longitudinal incision, exposing the extensor musculature.
Hand Fasciotomies
Decompression of the hand requires meticulous attention to the ten distinct compartments.
- Dorsal Interossei: Two longitudinal dorsal incisions are made. The first is centered over the second metacarpal (releasing the 1st and 2nd dorsal interossei). The second is centered over the fourth metacarpal (releasing the 3rd and 4th dorsal interossei).
- Volar Interossei: Through the same dorsal incisions, blunt dissection is carried volar to the transverse metacarpal ligament to decompress the volar interosseous compartments.
- Thenar and Hypothenar Compartments: The thenar compartment is decompressed via a longitudinal incision along the radial border of the first metacarpal. The hypothenar compartment is released via a longitudinal incision along the ulnar border of the fifth metacarpal.
- Adductor Compartment: This can be accessed through the dorsal incision over the second metacarpal by dissecting bluntly along the ulnar border of the first metacarpal.

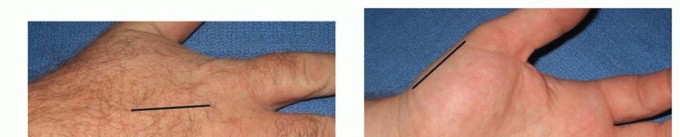
Placement of dorsal hand incisions over the second and fourth metacarpals for interosseous compartment decompression.
Digit Fasciotomies
When digital decompression is indicated, mid-axial incisions are utilized.
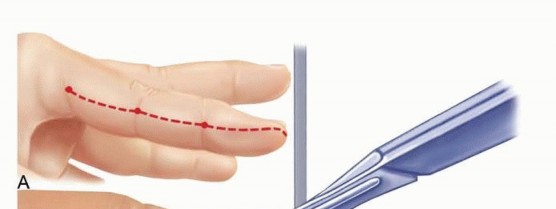
- Incision: A longitudinal incision is made along the mid-axial line of the digit (typically ulnar side for digits 2-4, and radial side for the thumb and small finger to avoid contact surfaces). The mid-axial line connects the apices of the flexion creases.
- Dissection: The incision is carried down to the flexor tendon sheath. Cleland's ligaments (dorsal to the neurovascular bundle) and Grayson's ligaments (volar to the neurovascular bundle) are divided. The neurovascular bundle must be carefully identified and protected throughout the dissection.

Mid-axial incision technique for digital fasciotomy, demonstrating protection of the neurovascular structures.
Muscle Viability Assessment and Fracture Management
Following complete decompression, all exposed muscle must be assessed for viability using the "4 Cs": Color, Consistency, Contractility, and Capacity to bleed. Frank necrotic muscle should be debrided, but borderline tissue should be left in situ for re-evaluation at a planned second-look operation 48 to 72 hours later.
If an underlying fracture is present, rigid internal fixation (ORIF) is the treatment of choice, provided the patient is physiologically stable. Stabilization prevents further soft tissue trauma and facilitates the extensive wound care required postoperatively. If the patient is unstable or the soft tissue envelope is catastrophically compromised, external fixation may be utilized.

Assessment of muscle viability post-decompression. Note the return of capillary bleeding and healthy red color in the viable muscle bellies.
Wound Management and Closure Strategies
Fasciotomy wounds are never closed primarily. The massive tissue edema precludes primary closure without recreating the compartment syndrome.
- Negative Pressure Wound Therapy (NPWT): The application of a wound VAC (Vacuum-Assisted Closure) at 75 to 125 mmHg continuous pressure is the current standard of care. NPWT manages exudate, reduces interstitial edema, and promotes granulation tissue formation.
- Vessel Loop Shoelace Technique: Alternatively, or in conjunction with NPWT, a dermatotraction technique using vessel loops interlaced through skin staples at the wound margins can provide continuous, gentle tension. This prevents skin retraction and facilitates delayed primary closure.
- Dressings: If NPWT is unavailable, sterile, non-adherent wet-to-dry dressings are applied, combined with a bulky, non-constricting splint.

Application of Negative Pressure Wound Therapy (NPWT) over a volar forearm fasciotomy wound to manage edema and exudate.
Complications and Management
The complications associated with acute compartment syndrome and its surgical management are severe and often life-altering. They range from systemic issues related to myonecrosis to localized functional deficits.
Volkmann's Ischemic Contracture
The most devastating local complication of missed or inadequately decompressed ACS is Volkmann's ischemic contracture. As necrotic muscle undergoes fibrotic replacement, it shortens, leading to classic fixed deformities: elbow flexion, forearm pronation, wrist flexion, metacarpophalangeal (MCP) joint extension, and interphalangeal (IP) joint flexion.
Tsuge classified Volkmann's contracture into three types:
* Mild: Localized to the deep finger flexors (FDP). Treated with tendon lengthening or muscle slides.
* Moderate: Involvement of FDP, FDS, and wrist flexors, often with median and ulnar nerve sensory deficits. Treated with radical infarct excision, neurolysis, and tendon transfers.
* Severe: Global involvement of volar and dorsal compartments. Salvage requires extensive debridement and free functional muscle transfers (e.g., gracilis flap).

Classic presentation of severe Volkmann's ischemic contracture, demonstrating fixed wrist flexion and intrinsic minus posturing of the digits.
Systemic Complications
Myonecrosis leads to rhabdomyolysis, releasing massive quantities of myoglobin, potassium, and creatine kinase into the systemic circulation. Myoglobinuria can precipitate acute tubular necrosis and acute renal failure. Management requires aggressive intravenous hydration, urine alkalinization with sodium bicarbonate, and potentially hemodialysis. Hyperkalemia can lead to fatal cardiac arrhythmias and must be managed emergently.
Iatrogenic Nerve Injury
The median nerve (especially the palmar cutaneous branch), superficial radial nerve, and medial antebrachial cutaneous nerve are at high risk during the surgical approach. Meticulous dissection and adherence to anatomic landmarks are imperative. Neuromas resulting from iatrogenic transection can cause debilitating chronic pain and Complex Regional Pain Syndrome (CRPS).
| Complication | Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Volkmann's Contracture | 1-10% (Higher in delayed presentations) | Prevention: Early diagnosis and complete fascial release. Salvage: Muscle slides, |
Clinical & Radiographic Imaging







You Might Also Like