Arthroscopic and Open Primary Repair of Acute Thumb Metacarpophalangeal Joint Radial and Ulnar Collateral Ligament Disruptions

Introduction and Epidemiology
Ulnar collateral ligament (UCL) and radial collateral ligament (RCL) disruptions of the thumb metacarpophalangeal (MCP) joint represent some of the most frequently encountered acute ligamentous injuries in hand and upper extremity surgery. Historically categorized under the colloquialisms of "skier's thumb" for acute UCL injuries and "gamekeeper's thumb" for chronic, attritional variants (originally described by Campbell in 1955 among Scottish fowl workers), these pathologies demand precise anatomical understanding and meticulous surgical management to restore pre-injury grip and pinch kinematics.
The mechanism of injury dictates the primary ligamentous disruption and subsequent pathoanatomy. Acute UCL injuries typically result from sudden, forceful hyperabduction and hyperextension of the thumb MCP joint. This vector of force is classically observed during a fall onto an outstretched hand with the thumb abducted, such as when a skier falls while gripping a ski pole, or when an athlete's hand strikes the playing surface. In this scenario, the proximal phalanx is levered radially, subjecting the ulnar-sided capsuloligamentous structures to catastrophic tensile failure.
Conversely, RCL injuries are precipitated by sudden, forced adduction and torsion of the MCP joint, often combined with hyperextension. While less common than their ulnar counterparts—comprising approximately 10 to 24 percent of all thumb MCP joint collateral ligament injuries—RCL tears are highly debilitating. The RCL plays a critical biomechanical role in resisting the palmar and ulnar subluxation forces generated during key pinch. A deficient RCL allows the proximal phalanx to subluxate under the unopposed pull of the adductor pollicis, leading to profound pinch weakness and early joint degeneration.
Epidemiologically, these injuries peak in the second to fourth decades of life, correlating directly with high-energy athletic participation and occupational hazards. The extent of the injury exists on a continuum, classified radiographically and clinically: microscopic interstitial sprains (Grade I), partial macroscopic tears with preserved stability (Grade II), and complete full-thickness disruptions with gross instability (Grade III). Complete Grade III disruptions frequently necessitate surgical intervention. This is particularly true when associated with a Stener lesion (interposition of the adductor aponeurosis) or significant articular instability, as non-operative management in these scenarios inevitably leads to chronic pain, pinch weakness, and progressive post-traumatic osteoarthritis.
Surgical Anatomy and Biomechanics
The MCP joint of the thumb is a highly specialized diarthrodial joint, transitional in morphology between a condyloid and a ginglymus (hinge) joint. The articulating surface of the proximal phalanx base is a shallow concavity that articulates with the asymmetric, trapezoidal metacarpal head, conferring minimal intrinsic osseous stability. Consequently, the joint relies heavily on its complex capsuloligamentous network and dynamic musculotendinous stabilizers.
The primary static stabilizers are the proper collateral ligaments (PCL) and the accessory collateral ligaments (ACL). Both the UCL and RCL complexes are structurally analogous, though they exhibit distinct differences in their failure patterns. The proper collateral ligaments originate from the dorsal aspect of the metacarpal neck epicondyles, dorsal to the joint's axis of rotation. They course obliquely in a volar and distal direction to insert onto the volar-lateral tubercles of the proximal phalanx base.
Biomechanically, the metacarpal head exhibits a "cam effect" due to its asymmetric profile—it is wider volarly than dorsally. As the MCP joint flexes, the proper collateral ligaments are drawn over the wider volar flare of the metacarpal condyles. Consequently, the PCLs are relatively lax in extension and become maximally taut in 30 to 40 degrees of MCP joint flexion, serving as the primary restraint to varus and valgus stress in the flexed posture.
The accessory collateral ligaments originate palmar to the proper collateral ligaments on the metacarpal neck and fan out to insert directly into the volar plate and the respective sesamoid bones. These structures are tensioned in full extension and provide critical stability in the dorsovolar plane. The volar plate itself is a robust fibrocartilaginous structure extending from the metacarpal neck to the proximal phalanx, preventing hyperextension and augmenting the articular surface area.
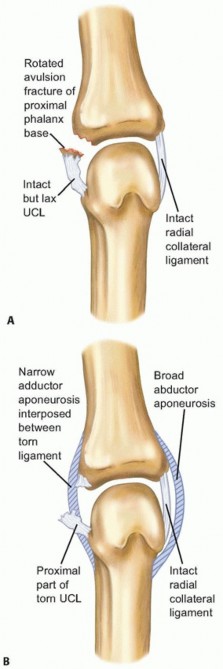
A critical anatomical distinction between the ulnar and radial aspects of the joint lies in the overlying aponeurotic structures, which dictate the pathology of complete ruptures. On the ulnar side, the adductor pollicis muscle (comprising transverse and oblique heads) transitions into a distinct, relatively narrow adductor aponeurosis that inserts into the extensor mechanism. When the UCL ruptures distally from its phalangeal insertion (the most common site of failure), the proximal stump can retract and become superficially displaced over the proximal edge of the adductor aponeurosis. This interposition, termed a Stener lesion, physically prevents the ligament from returning to its anatomical footprint. Spontaneous healing is impossible, rendering non-operative management futile.
Conversely, the radial aspect of the joint is covered by the broad abductor pollicis brevis (APB) aponeurosis. Because of its expansive coverage, a true Stener-equivalent lesion on the radial side is exceptionally rare. However, proximal retraction and interposition of local capsular tissue or the APB aponeurosis itself can still inhibit optimal healing of a completely ruptured RCL, often necessitating operative repair to restore anatomical tension.
Indications and Contraindications
The decision algorithm for operative versus non-operative management hinges on the grade of the injury, the presence of an aponeurotic interposition (Stener lesion), and the degree of clinical instability. Clinical evaluation requires meticulous, examiner-controlled stress testing of the MCP joint in both full extension (testing the ACL and volar plate) and 30 degrees of flexion (isolating the PCL).
Laxity greater than 30 degrees absolute, or a side-to-side discrepancy of greater than 15 degrees compared to the uninjured contralateral thumb, is highly sensitive and specific for a complete Grade III disruption. Furthermore, the lack of a firm, distinct endpoint during stress testing strongly correlates with a full-thickness tear.
Advanced imaging is instrumental in surgical planning. Standard radiographs (posteroanterior, lateral, and Roberts views) are mandatory to rule out osseous avulsions. High-resolution magnetic resonance imaging (MRI) or dynamic ultrasonography is highly sensitive for identifying Stener lesions, quantifying the degree of ligamentous retraction, and assessing for concomitant chondral or volar plate damage.
Operative vs Non Operative Management Parameters
| Parameter | Non-Operative Management | Operative Management |
|---|---|---|
| Injury Grade | Grade I and Grade II (Interstitial or partial tears) | Grade III (Complete full-thickness tears) |
| Clinical Laxity | < 30° absolute laxity; < 15° side-to-side difference | > 30° absolute laxity; > 15° side-to-side difference |
| Endpoint on Stress Test | Firm, distinct endpoint | Soft, mushy, or absent endpoint |
| Imaging Findings | Intact ligament continuity, minimal edema, no retraction | Complete disruption, Stener lesion present, significant gapping |
| Associated Fractures | Minimally displaced avulsion fractures (< 2mm) | Displaced avulsion fractures (> 2mm) or involving > 20% of articular surface |
| Chronicity | Acute injuries amenable to immobilization | Acute complete tears (< 6 weeks), or chronic symptomatic instability requiring reconstruction |
Contraindications to primary surgical repair include advanced degenerative joint disease of the MCP joint (where primary arthrodesis is the preferred reconstructive option), active local soft tissue infection, or severe medical comorbidities precluding safe anesthesia. Additionally, injuries older than 6 weeks may exhibit significant ligamentous resorption and scarring, making primary repair impossible and necessitating tendon graft reconstruction (e.g., palmaris longus graft).
Pre Operative Planning and Patient Positioning
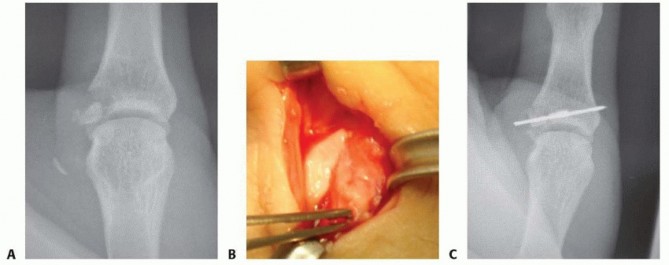
Thorough preoperative planning ensures a streamlined surgical workflow and minimizes intraoperative complications. Radiographic evaluation must be carefully scrutinized. If an avulsion fracture involves more than 20 percent of the articular surface and is displaced, the surgical plan must pivot from soft-tissue suture anchor repair to osseous fixation using miniature screws, Kirschner wires, or tension-band constructs to restore articular congruity.
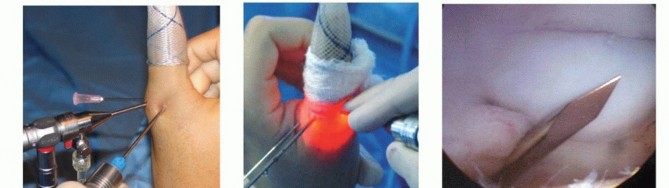
The procedure is typically performed on an outpatient basis. Anesthesia can be achieved via a regional brachial plexus block (axillary or supraclavicular approach) supplemented with intravenous sedation. Alternatively, the wide-awake local anesthesia no tourniquet (WALANT) technique is increasingly utilized. WALANT utilizes a mixture of lidocaine and epinephrine, providing excellent hemostasis without a tourniquet while allowing for intraoperative dynamic active testing of the repair construct by the awake patient.
The patient is positioned supine with the operative extremity extended onto a radiolucent hand table. If a WALANT technique is not employed, a well-padded pneumatic tourniquet is applied to the proximal arm. The limb is exsanguinated with an Esmarch bandage, and the tourniquet is inflated to 250 mmHg.
For arthroscopic-assisted repairs, specialized small-joint equipment must be available. This includes a 1.9 mm or 2.7 mm 30-degree arthroscope, a dedicated small-joint fluid management system, and small-joint instrumentation (shavers, biters, and radiofrequency wands). The thumb is placed in a small-joint traction tower utilizing Chinese finger traps, applying 5 to 10 pounds of longitudinal traction to distract the MCP joint sufficiently for instrument navigation.

Detailed Surgical Approach and Technique
The surgical technique varies depending on the specific ligament injured (ulnar versus radial) and the chosen modality (open versus arthroscopic). Mastery of the regional neurovascular anatomy, particularly the superficial sensory nerves, is critical in all approaches to avoid debilitating postoperative neuromas.
Open Ulnar Collateral Ligament Repair
A lazy-S or gently curved longitudinal incision is made over the ulnar aspect of the thumb MCP joint, centered over the joint line. Straight longitudinal incisions over the flexion crease should be strictly avoided to prevent postoperative volar scar contracture.
Careful blunt dissection is employed through the subcutaneous tissues. The dorsal sensory branches of the radial nerve (Wartenberg's nerve) are highly variable in this region; they must be meticulously identified, mobilized, and protected with vessel loops. Neuropraxia or transection of these branches is a significant source of postoperative morbidity and complex regional pain syndrome (CRPS).

Deep to the subcutaneous fat, the adductor aponeurosis is visualized. In the setting of a complete UCL tear, a Stener lesion may be immediately apparent as a bulbous, hemorrhagic mass of ligamentous tissue sitting superficial to the proximal edge of the aponeurosis. To access the joint capsule and the native ligament footprint, the adductor aponeurosis is incised longitudinally, parallel to the extensor pollicis longus (EPL) tendon, leaving a robust 2 to 3 mm cuff of tissue dorsally to facilitate later repair. Alternatively, a step-cut or Z-lengthening incision can be utilized for easier closure.
Once the aponeurosis is reflected volarly, the UCL is inspected. Most commonly, the ligament is avulsed from its distal insertion on the proximal phalanx. The joint is thoroughly irrigated, and any interposed capsular tissue, hematoma, or chondral debris is debrided. The anatomical footprint at the volar-ulnar base of the proximal phalanx is decorticated with a curette or a small rongeur to expose bleeding cancellous bone. This step is critical for optimizing the biological environment for robust ligament-to-bone healing.
A modern suture anchor (typically 1.3 mm to 3.0 mm in diameter, depending on bone quality) is inserted into the prepared footprint. The trajectory of the drill and anchor should be directed distally and slightly volarly to avoid violating the articular surface of the proximal phalanx. The sutures are then passed through the distal stump of the UCL using a locking grasping stitch configuration (e.g., modified Kessler, Krackow, or running interlocking stitch) to maximize pull-out strength.
The MCP joint is reduced and held in approximately 30 degrees of flexion with slight ulnar deviation. This approximates the ligament to its footprint without excessive tension. The sutures are tied securely. The repair is dynamically stressed to confirm stability, restoration of a firm endpoint, and the absence of joint subluxation. The adductor aponeurosis is subsequently repaired using an absorbable suture (e.g., 3-0 Vicryl), and the skin is closed in a standard fashion.
Open Radial Collateral Ligament Repair
The approach for a radial collateral ligament repair mirrors that of the ulnar side but necessitates a dorsoradial incision. The terminal branches of the superficial radial nerve are at significant risk here and must be retracted gently.
The abductor pollicis brevis aponeurosis is identified and split longitudinally to expose the underlying capsule and RCL. Unlike UCL tears, which predominantly occur at the phalangeal insertion, RCL tears frequently occur at the proximal origin on the metacarpal head or within the mid-substance of the ligament.
For proximal avulsions, the footprint on the radial epicondyle of the metacarpal neck is debrided. A suture anchor is placed at the anatomical origin. It is imperative that the anchor is countersunk or seated deep enough to prevent hardware prominence beneath the thin radial soft tissues, which can cause significant postoperative irritation. The sutures are passed through the ligament, and the joint is immobilized in neutral to slight radial deviation during knot tying. Mid-substance tears may be repaired primarily using non-absorbable sutures in a figure-of-eight or horizontal mattress configuration, augmented by local capsular tissue or a periosteal flap if the repair is tenuous.

Arthroscopic Assisted Repair
Arthroscopic repair of MCP joint collateral ligaments is an advanced, technically demanding technique that offers the advantages of minimized soft tissue dissection, preservation of the extensor aponeurosis, and comprehensive evaluation of intra-articular pathology, including occult osteochondral lesions.
Standard radioulnar (1R) and radioulnar (1U) portals are established just proximal to the joint line, on either side of the EPL tendon. A diagnostic arthroscopy is performed to assess the articular cartilage, the volar plate, and the integrity of the collateral ligaments.

For a UCL avulsion, the ulnar recess is cleared of hematoma and capsular debris using a 2.0 mm shaver. The phalangeal footprint is prepared arthroscopically down to bleeding bone. A small stab incision is made over the ulnar aspect of the joint to allow for percutaneous anchor placement. Under direct arthroscopic visualization, the anchor drill is introduced, and the anchor is deployed into the proximal phalanx.
Suture passage can be achieved using specialized micro-suture passers or spinal needles to shuttle the sutures through the ligament stump. Knotless anchor constructs are particularly advantageous in arthroscopic repairs to minimize the volume of suture material and knot stacks within the tight joint capsule. The repair is tensioned, and stability is confirmed arthroscopically before portal closure.
Complications and Management
Despite meticulous surgical technique, complications following primary repair of thumb MCP joint collateral ligaments can occur. The most frequent complication is transient neuropraxia of the dorsal sensory branches of the radial nerve. This typically resolves with observation, desensitization therapy, and neuromodulatory medications (e.g., gabapentinoids). Iatrogenic transection resulting in a painful neuroma may require surgical exploration, neuroma excision, and targeted muscle reinnervation (TMR) or burying the nerve stump into bone.
Stiffness of the MCP joint is another common sequela, particularly in cases of prolonged postoperative immobilization (beyond 4 weeks). While a slight loss of terminal flexion is generally well-tolerated and does not significantly impair hand function, severe arthrofibrosis may require aggressive hand therapy, dynamic splinting, or, rarely, surgical capsulotomy and tenolysis.
Recurrent instability is a catastrophic complication, often resulting from patient non-compliance with rehabilitation, premature return to high-impact activities, failure of biological healing due to poor bone quality, or technical errors (e.g., placing the anchor too dorsally, failing to recreate the proper tension axis).

Common Surgical Complications and Salvage Strategies
| Complication | Estimated Incidence | Etiology / Risk Factors | Management and Salvage Strategies |
|---|---|---|---|
| Radial Sensory Neuropraxia | 10% - 15% | Excessive traction, direct laceration during approach | Observation, gabapentinoids; surgical exploration and neuroma management if refractory |
| MCP Joint Stiffness | 15% - 20% | Prolonged immobilization (> 4 weeks), overtensioned repair | Aggressive hand therapy, dynamic splinting; late surgical capsulotomy if refractory |
| Recurrent Instability | 3% - 5% | Non-compliance with rehab, poor bone quality, technical error | Revision with free tendon graft reconstruction (e.g., palmaris longus) or MCP joint arthrodesis |
| Hardware Prominence | 2% - 4% | Superficial anchor placement, large knot stacks under thin skin | Hardware removal after biological healing is confirmed (typically > 6 months post-op) |
| Infection | < 1% | Standard surgical risks, diabetic patients, immunocompromise | Oral/IV antibiotics; urgent surgical irrigation and debridement for deep space/articular infections |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is meticulously designed to protect the healing ligamentous construct while mitigating the risk of arthrofibrosis and extensor tendon adhesions.
Phase I: Immobilization (0 to 2 Weeks)
Immediately postoperatively, the thumb is immobilized in a bulky thumb spica orthosis or a short-arm thumb spica cast. The interphalangeal (IP) joint is deliberately left free to allow for immediate active range of motion, preventing EPL and flexor pollicis longus (FPL) adhesions. The wrist is positioned in slight extension (20 degrees), and the MCP joint is immobilized in neutral to 15 degrees of flexion to minimize tension on the repair.
Phase II: Protected Motion (2 to 4 Weeks)
At the two-week mark, sutures are removed. The patient is transitioned to a custom-molded thermoplastic hand-based thumb spica splint. Gentle, active range of motion of the MCP joint is initiated under the strict guidance of a certified hand therapist. All passive motion and any varus/valgus stressing are strictly prohibited during this phase. The splint is worn continuously, removed only for hygiene and designated, supervised exercise sessions.
Phase III: Progression of Motion (4 to 6 Weeks)
Active-assisted range of motion is introduced to maximize the arc of motion. The splint is gradually weaned during the day for light, non-resistive activities of daily living (ADLs) but must be maintained at night and in vulnerable environments (e.g., crowds, public transport).
Phase IV: Strengthening and Return to Play (6 to 12 Weeks)
At six weeks, biological healing of the ligament to bone is generally sufficient to initiate gentle strengthening exercises, including putty squeezing and isometric key pinch strengthening. Dynamic stressing of the ligament is gradually introduced. Return to full, unrestricted athletic activity is typically permitted between 8 to 12 weeks, contingent upon the restoration of symmetric pinch strength and the absence of pain. For contact sports or skiing, prophylactic taping or the use of a rigid thumb spica playing splint is highly recommended for the remainder of the athletic season to prevent reinjury.
Summary of Key Literature and Guidelines
The foundational understanding of acute thumb MCP joint instability is rooted in the seminal work of Stener in 1962, who first described the interposition of the adductor aponeurosis in complete UCL ruptures. This anatomical discovery established the absolute clinical indication for operative intervention in Grade III injuries with displacement, altering the trajectory of hand surgery.
Subsequent long-term outcome studies, such as those by Glickel et al., have consistently demonstrated that primary open repair of acute UCL injuries yields excellent functional results, with over 90% of patients returning to their pre-injury level of activity. The literature emphasizes that primary repairs performed within the first three to four weeks post-injury have significantly better outcomes regarding range of motion and stability compared to delayed reconstructions utilizing tendon grafts.
Recent advancements in arthroscopic techniques have been extensively evaluated in the literature. Comparative cohort studies indicate that while arthroscopic-assisted repairs have a steeper learning curve and require specialized equipment, they offer statistically significant improvements in early postoperative range of motion and a reduction in incisional morbidity compared to traditional open techniques. Biomechanical analyses of suture anchor fixation have consistently shown that modern micro-anchors provide load-to-failure strengths that exceed the physiological forces of early active rehabilitation, supporting the modern trend toward accelerated postoperative motion protocols.
The management of radial collateral ligament injuries, while less prominently featured in historical literature, follows parallel biomechanical principles. Contemporary studies highlight the critical necessity of restoring the RCL to prevent the palmar and ulnar subluxation of the proximal phalanx that occurs under the unopposed pull of the adductor pollicis during key pinch maneuvers. Optimal outcomes in both RCL and UCL repairs rely on a triad of success: anatomical reduction, rigid mechanical fixation, and a meticulously supervised rehabilitation paradigm.
You Might Also Like


