Basic Arthroscopic Techniques: Principles of Triangulation and Surgical Mastery
Key Takeaway
Arthroscopy represents a paradigm shift in orthopaedic surgery, demanding rigorous skill acquisition and a profound understanding of spatial orientation. The cornerstone of operative arthroscopy is the triangulation technique, which allows independent movement of the arthroscope and surgical instruments. Mastery of these basic arthroscopic techniques minimizes patient morbidity, accelerates rehabilitation, and enables complex intra-articular interventions that are often inaccessible via traditional open arthrotomy.
INTRODUCTION TO ARTHROSCOPIC SURGERY
The advent and evolution of arthroscopy have fundamentally transformed the landscape of orthopaedic surgery. What began as a purely diagnostic modality has rapidly evolved into a highly sophisticated therapeutic discipline, allowing for the minimally invasive management of complex intra-articular pathology. Proficiency in basic arthroscopic techniques requires a great deal of patience, persistence, and a profound understanding of altered spatial proprioception.
Patients’ expectations regarding the use of arthroscopic techniques have placed tremendous demands on practicing orthopaedic surgeons. The allure of smaller incisions, accelerated rehabilitation, and reduced postoperative pain drives patient preference. However, a surgeon must never be persuaded by these external pressures to perform a difficult arthroscopic procedure for which sufficient psychomotor skills have yet to be developed. Patient safety and optimal clinical outcomes must remain the paramount objectives.
SURGICAL WARNING:
If an arthroscopic procedure is not progressing as expected, or if visualization is critically compromised, it is imperative to abort the arthroscopic approach and return to an open method that has yielded proven, reliable results in the past. A skillfully performed procedure through an open arthrotomy is universally preferable to a poorly executed, prolonged arthroscopic procedure that risks iatrogenic neurovascular or chondral injury.
As arthroscopic procedures become better defined and technological instrumentation continues to improve, the volume and complexity of these interventions are increasing steadily. There remains a steep learning curve for the successful completion of complicated procedures, such as shoulder stabilization (e.g., arthroscopic Bankart repair) and rotator cuff repair. The practicing surgeon must commit to lifelong learning—keeping abreast of current literature, attending hands-on cadaveric workshops, and observing master arthroscopists.
SKILL ACQUISITION AND THE LEARNING CURVE
The transition from open surgery to arthroscopy requires a fundamental rewiring of the surgeon's hand-eye coordination. In open surgery, the surgeon enjoys direct, three-dimensional binocular vision. In arthroscopy, the surgeon must navigate a three-dimensional anatomical space using a two-dimensional monitor, relying heavily on tactile feedback and monocular depth cues.
Techniques are best learned through a structured, stepwise progression:
* Didactic and Virtual Reality Training: Utilizing high-fidelity simulators to develop basic camera navigation and triangulation skills without patient risk.
* Cadaveric Laboratories: Hands-on learning sources provided by the American Academy of Orthopaedic Surgeons (AAOS) and specialty societies (e.g., AANA) are excellent, low-risk environments to learn new procedures and test novel instrumentation.
* Mentored Clinical Practice: Assisting and performing surgical procedures under the direct supervision of an experienced arthroscopist during residency, fellowship, or early clinical practice.
* Continuous Education: Utilizing peer-reviewed internet surgical videos available through academic portals and vendor websites to visualize complex spatial approaches.
OPERATING ROOM SETUP AND ERGONOMICS
Before mastering intra-articular techniques, the surgeon must master the extra-articular environment. Proper operating room setup is critical to minimizing surgeon fatigue and maximizing technical precision.
Monitor Placement and Line of Sight
The surgical monitor must be positioned directly across from the surgeon, aligned with the surgeon's line of sight and the anatomical axis of the joint being operated upon. If the surgeon is forced to turn their head or torso to view the monitor, spatial disorientation and musculoskeletal fatigue will rapidly ensue.
Fluid Management and Joint Distension
Arthroscopy relies on a fluid medium to distend the joint capsule, providing a clear optical cavity and maintaining hemostasis through hydrostatic pressure.
* Gravity vs. Pump Systems: While gravity inflow can be used for simple diagnostic procedures, automated fluid management pumps are preferred for operative arthroscopy. They maintain a constant intra-articular pressure (typically 30–40 mm Hg for the knee, and up to 60 mm Hg for the shoulder) while adjusting flow rates to clear debris.
* Hemostasis: If bleeding obscures the visual field, transiently increasing the pump pressure or adding epinephrine (typically 1 mg per 3 liters of irrigation fluid) can restore clarity.
PITFALL:
Excessive intra-articular pressure, especially in the presence of capsular defects, can lead to massive fluid extravasation, resulting in compartment syndrome of the extremity. Always monitor the tension of the surrounding soft tissues throughout the procedure.
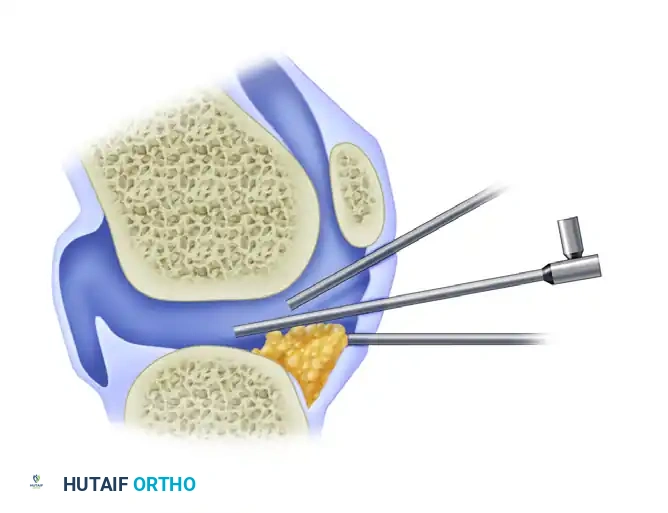
THE TRIANGULATION TECHNIQUE
The absolute cornerstone of operative arthroscopy is the principle of triangulation. Triangulation involves the use of one or more instruments inserted through separate portals and brought into the optical field of the arthroscope. Geometrically, the tip of the working instrument and the lens of the arthroscope form the base angles of a triangle, with the target intra-articular pathology forming the apex.
Biomechanics and Optical Principles
Triangulation separates the arthroscope from the operating instrument. This separation is critical for several reasons:
1. Magnification and Field of View: It allows the viewing arthroscope to be manipulated independently to enlarge the image or increase the panoramic field of view.
2. Variable Angles of Inclination: By rotating the light post of a 30-degree or 70-degree arthroscope, the angle of inclination can be varied, allowing improved visual access to hidden recesses of the joint (e.g., the posterior compartments of the knee).
3. Depth Perception: Separation of the instruments from the arthroscope provides dynamic monocular depth cues. As the instrument moves relative to the fixed background anatomy, the surgeon's brain reconstructs the three-dimensional space.
4. Independent Movement: Perhaps the most significant advantage, it permits the independent, unencumbered movement of the arthroscope and the surgical instrument, which is an absolute prerequisite for complex operative interventions like suturing or tissue ablation.
Step-by-Step Execution of Triangulation
Mastering triangulation requires a systematic approach to portal placement and instrument introduction.
- Establish the Viewing Portal: Insert the arthroscope through the primary portal (e.g., the anterolateral portal in the knee). Perform a systematic diagnostic sweep to orient yourself to the intra-articular anatomy.
- Spinal Needle Localization: Before making a working portal incision, insert an 18-gauge spinal needle into the joint under direct arthroscopic visualization. This ensures the trajectory of the working instrument will reach the target pathology without being obstructed by the fat pad, condyles, or ligaments.
- Establish the Working Portal: Create a precise dermatotomy. The working portal should ideally be placed so that the instrument approaches the arthroscope at an angle of 45 to 60 degrees.
- Converging Portals: If portals are placed too close together, the instruments will parallel the arthroscope, leading to a loss of depth perception and physical clashing ("sword-fighting") outside the joint.
- Panoramic Positioning: To begin triangulation, the arthroscope should be pulled back to a distance from the area to be probed. This provides a wide, panoramic field of vision, making it easier to locate the incoming instrument.
- Instrument Introduction: Introduce the probe or surgical instrument blindly through the capsule, guided by the external trajectory established by the spinal needle.
- Target Acquisition: Once the tip of the instrument enters the panoramic optical field, the scope and the instrument are advanced together toward the intended area. This simultaneous advancement reduces the field of vision while increasing the magnification of the target pathology.
CLINICAL PEARL:
A mistake commonly made by beginning arthroscopists is placing the scope too close to the target tissue before introducing the instrument. This creates a "microscopic" field of view. When the instrument enters the joint, it bypasses the narrow optical field entirely, resulting in the surgeon "losing the instrument" and risking iatrogenic damage to adjacent articular cartilage. Always pull back to a panoramic view to find your instrument.
ADVANTAGES OF ARTHROSCOPIC SURGERY
When basic arthroscopic techniques are mastered and executed correctly, the advantages over traditional open arthrotomy are profound. The minimization of surgical trauma alters the entire postoperative recovery trajectory.
1. Minimization of Surgical Morbidity
Open arthrotomies require extensive soft tissue dissection, capsular incision, and often the detachment of stabilizing structures. Arthroscopic techniques eliminate these requirements.
* Cosmesis and Scarring: Painful, disfiguring scars are virtually eliminated, replaced by millimeter-length portal incisions.
* Preservation of the Extensor Mechanism: In knee surgery, open approaches often disrupt the extensor mechanism, leading to functional imbalance, prolonged quadriceps inhibition, and arthrofibrosis. Arthroscopy preserves the extensor mechanism entirely, allowing for immediate postoperative muscle activation.
2. Reduced Hospital Stay and Economic Impact
The vast majority of arthroscopic procedures—ranging from simple meniscectomies to complex multi-ligament reconstructions—are now performed on an outpatient ambulatory basis. This transition drastically reduces hospital resource utilization, lowers the economic burden on the healthcare system, and allows the patient to recover in the comfort of their own home.
3. Reduced Complication Rates
While no surgical procedure is without risk, the complication profile of arthroscopy is highly favorable compared to open surgery.
* Infection: The continuous flow of sterile irrigation fluid, combined with minimal atmospheric exposure of the joint cavity, reduces the rate of deep joint infection (septic arthritis) to less than 0.5%.
* Thromboembolism: Because patients are mobilized almost immediately following surgery, the risk of deep vein thrombosis (DVT) and pulmonary embolism (PE) is significantly lower than in traditional open joint surgery.
4. Improved Follow-up and "Second-Look" Capabilities
The minimal morbidity associated with arthroscopy allows the intra-articular environment to be easily reevaluated if persistent symptoms warrant further investigation.
* These are often referred to as “relook” or “second-look” procedures.
* For example, following a complex meniscal repair or an autologous chondrocyte implantation (ACI), a second-look arthroscopy can be performed with minimal patient downtime to assess tissue healing, probe the repair site, and debride any reactive synovitis.
5. Access to Anatomical "Blind Spots"
There is a distinct possibility of performing surgical procedures that are difficult, highly morbid, or frankly impossible to perform through an open arthrotomy.
* A number of surgical procedures are vastly more easily performed with arthroscopic techniques.
* Meniscal Accessibility: The posterior horns of the medial and lateral menisci are notoriously difficult to visualize through an anterior arthrotomy without aggressive, potentially damaging retraction of the collateral ligaments. With a 30-degree or 70-degree arthroscope, these areas are easily illuminated and magnified. Many menisci that are highly amenable to repair are accessible only with arthroscopic techniques and cannot be satisfactorily viewed or instrumented through an open incision.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The success of any arthroscopic procedure relies heavily on the postoperative rehabilitation protocol. Because the surgical trauma to the joint capsule and overlying musculature is minimized, rehabilitation can typically commence immediately.
- Cryotherapy and Compression: Immediate postoperative application of cold therapy and compressive dressings is essential to manage hemarthrosis and limit reactive joint effusion.
- Early Range of Motion (ROM): Unlike open procedures that may require prolonged immobilization to protect capsular repairs, arthroscopic procedures (such as meniscectomy or loose body removal) allow for immediate, progressive ROM exercises to prevent arthrofibrosis and stimulate cartilage nutrition.
- Weight-Bearing Status: Weight-bearing is dictated by the specific intra-articular procedure performed rather than the surgical approach. Simple debridements may allow immediate weight-bearing as tolerated (WBAT), whereas meniscal repairs or microfracture procedures will necessitate strict non-weight-bearing (NWB) or partial weight-bearing protocols for 4 to 6 weeks to protect the healing tissue.
CONCLUSION
The mastery of basic arthroscopic techniques is a mandatory milestone in the career of a modern orthopaedic surgeon. The principles of triangulation, fluid management, and spatial orientation form the foundation upon which all advanced minimally invasive joint surgeries are built. By respecting the steep learning curve, utilizing meticulous portal placement, and understanding the optical physics of the arthroscope, the surgeon can leverage the profound advantages of arthroscopy—delivering superior clinical outcomes, minimizing patient morbidity, and expanding the frontiers of joint preservation. However, the ultimate hallmark of a master surgeon remains the clinical judgment to recognize the limitations of the technique and the humility to convert to an open procedure when patient safety demands it.
You Might Also Like