
Comprehensive Introduction and Patho-Epidemiology
The knee is unequivocally the joint in which arthroscopy has found its greatest diagnostic and intraarticular surgical application, fundamentally altering the landscape of orthopedic surgery. Over the past several decades, the usefulness of arthroscopic techniques in the diagnosis and definitive treatment of intraarticular pathology has been exhaustively documented, transitioning from a novel exploratory tool to the gold standard of intraarticular intervention. Historically, arthroscopy allowed for the rigorous evaluation of the accuracy of clinical examinations, laboratory tests, radiographs, and early magnetic resonance imaging (MRI). The pioneering work of early arthroscopists demonstrated that clinical impressions were frequently incomplete or entirely inaccurate when compared to direct arthroscopic visualization. In a seminal analysis, Johnson compared preoperative clinical impressions with definitive arthroscopic diagnoses and found a statistically significant number of additional pathological entities, including completely different primary diagnoses, in a large percentage of patients. For instance, in a cohort of 229 patients presumed to have an isolated torn medial meniscus, arthroscopy confirmed this as an isolated diagnosis in only 21% of cases.
The patho-epidemiology of knee internal derangement reveals a complex interplay of ligamentous, meniscal, and chondral injuries that rarely occur in isolation. Additional pathology was identified in 23% of Johnson's cohort, and a completely different diagnosis was established in 56%. Furthermore, an unsuspected lateral meniscal tear was noted in 5% of the knees originally diagnosed with a medial meniscal tear. Ligamentous injuries, particularly to the anterior cruciate ligament (ACL), are notoriously associated with concomitant intraarticular damage. Only 10% of patients with a torn ACL present without other identifiable lesions; in 70% of all patients with ACL ruptures, an accompanying tear of a meniscus is identified. Curran and Woodward further elucidated this diagnostic gap by studying 396 knee arthroscopies, finding that the total clinical accuracy rate was a mere 71%. The implementation of diagnostic arthroscopy increased their diagnostic accuracy to an unprecedented 97%, cementing its role in the orthopedic armamentarium.
Acute traumatic hemarthrosis represents a specific patho-epidemiological subset where arthroscopy has proven invaluable. Noyes et al. reported some degree of ACL disruption in 72% of knees undergoing arthroscopy for acute, traumatic hemarthrosis; critically, many of these knees exhibited negative or equivocal clinical stress tests due to guarding and acute pain. DeHaven, Gillquist, and Hagberg similarly documented a remarkably high frequency of torn ACLs and other internal derangements in patients presenting with acute traumatic hemarthrosis when arthroscopy was performed early in the clinical evaluation process. These findings underscore the high prevalence of severe structural damage masked by acute effusion and muscle spasm, highlighting the necessity of direct visualization in complex presentations.
Despite its historical role as a primary diagnostic tool, modern orthopedic practice dictates that arthroscopy should be considered a surgical adjunct used in conjunction with a comprehensive history, meticulous physical examination, and appropriate advanced imaging. It must serve as an extension of, not a replacement for, a thorough clinical evaluation. With the ubiquitous availability and increased resolution of modern MRI, alongside enhanced proficiency in clinical examination, the purely "diagnostic arthroscopy" is now exceedingly rare and generally discouraged. Surgical alternatives and potential interventions must be discussed thoroughly with the patient prior to the procedure. Today, the definitive surgical procedure is anticipated and performed concurrently at the time of a thorough arthroscopic diagnostic sweep, minimizing anesthetic exposure and optimizing patient outcomes.


Detailed Surgical Anatomy and Biomechanics
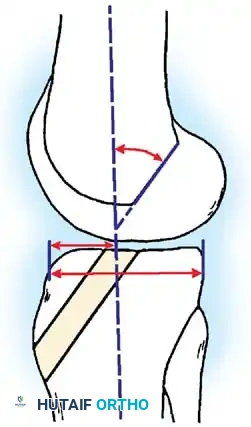
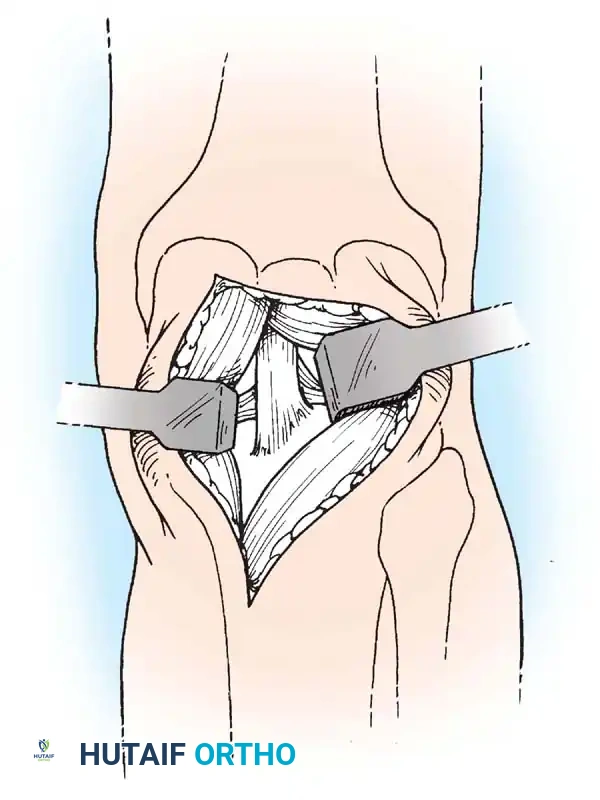
A profound understanding of the surgical anatomy and biomechanics of the knee is the absolute prerequisite for safe and effective arthroscopy. The knee is a complex modified hinge joint comprising two distinct articulations: the tibiofemoral joint and the patellofemoral joint. The osseous anatomy dictates the limits of arthroscopic maneuverability. The medial femoral condyle extends further distally and is more curved than the lateral condyle, contributing to the "screw-home" mechanism—an obligate external rotation of the tibia during the final degrees of extension, which locks the joint in a stable position. This biomechanical phenomenon must be accounted for during arthroscopic evaluation, as varying degrees of flexion are required to unlock the joint and adequately visualize the posterior aspects of the condyles and the meniscal horns. The intercondylar notch houses the cruciate ligaments, and its morphometry (e.g., notch width index) is a critical factor in both native ACL rupture risk and the technical execution of notchplasty during reconstruction.
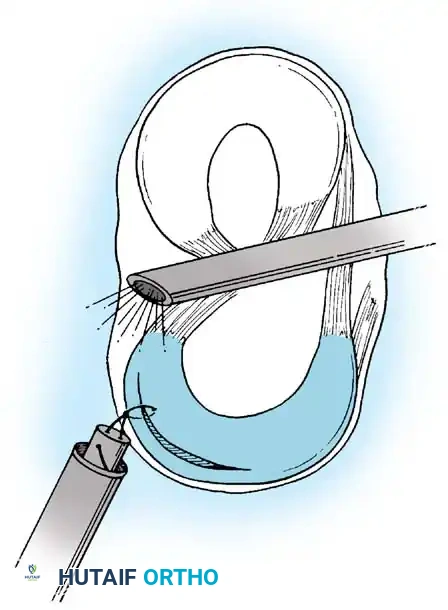
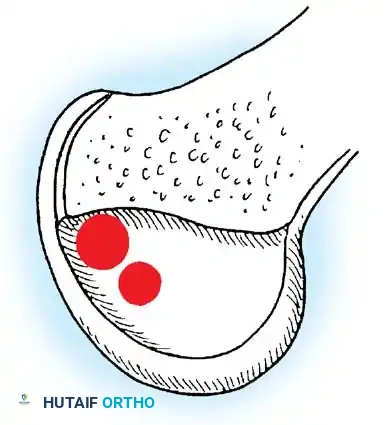
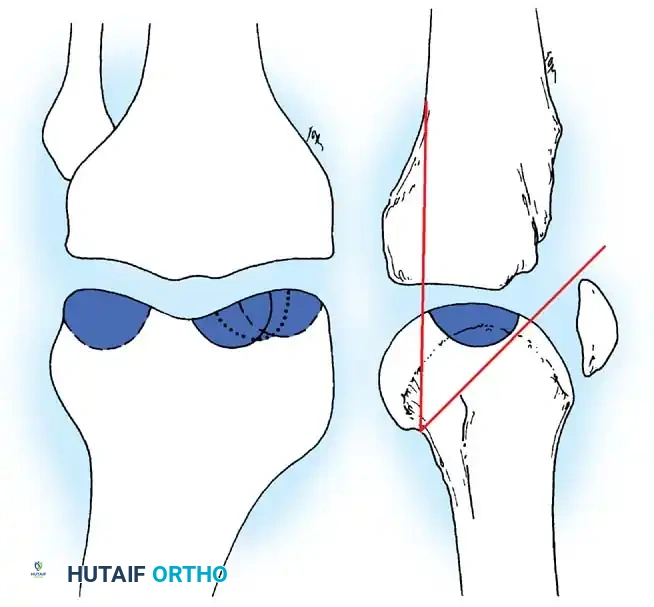
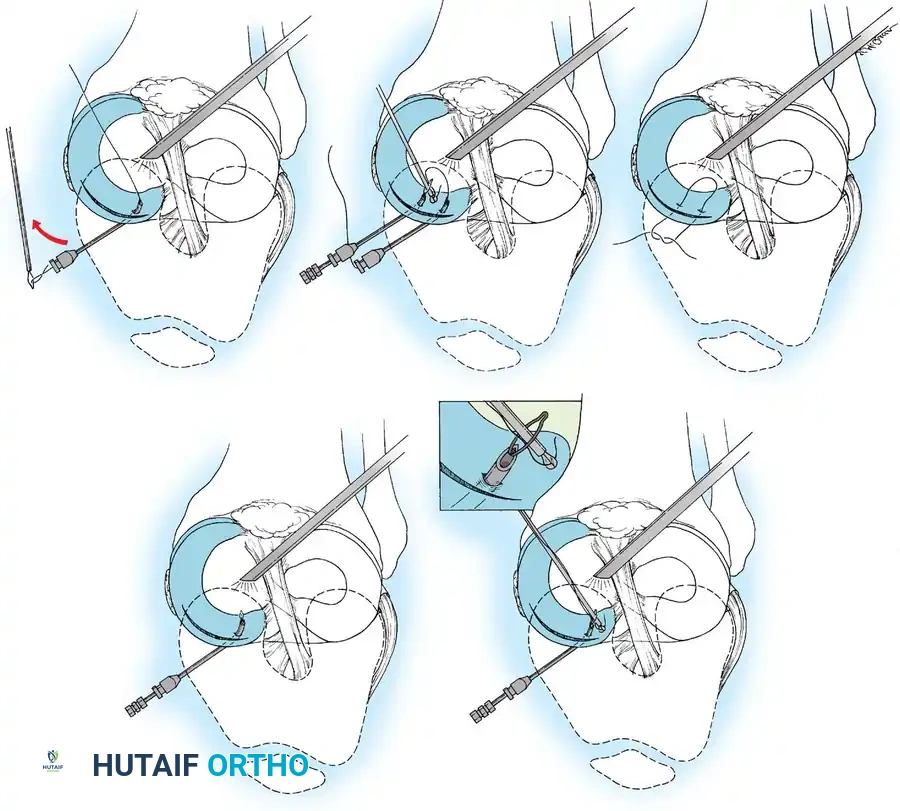
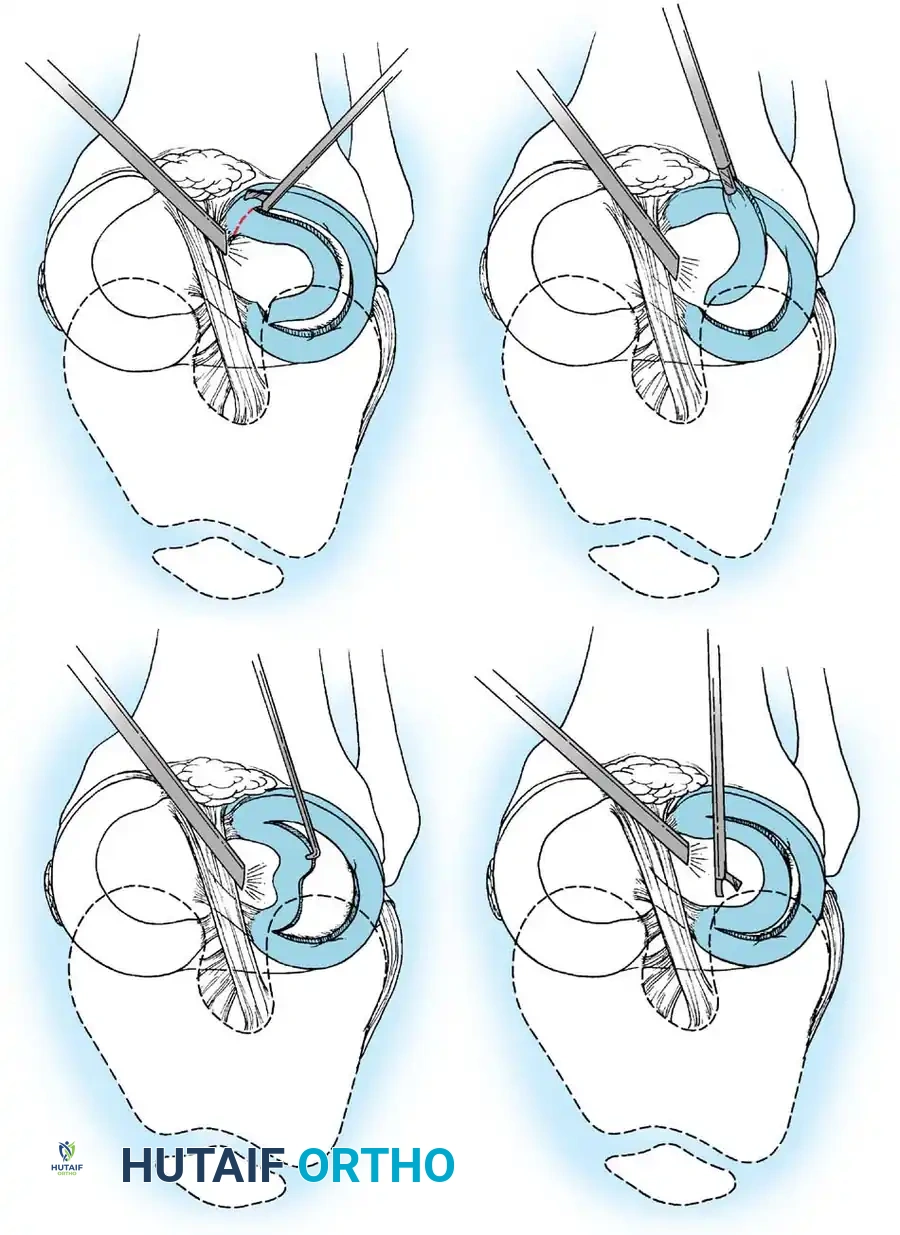
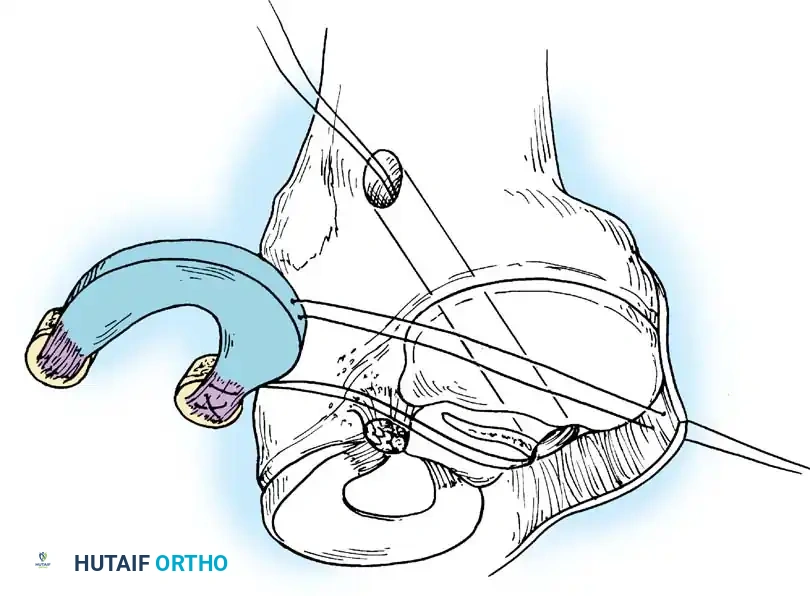
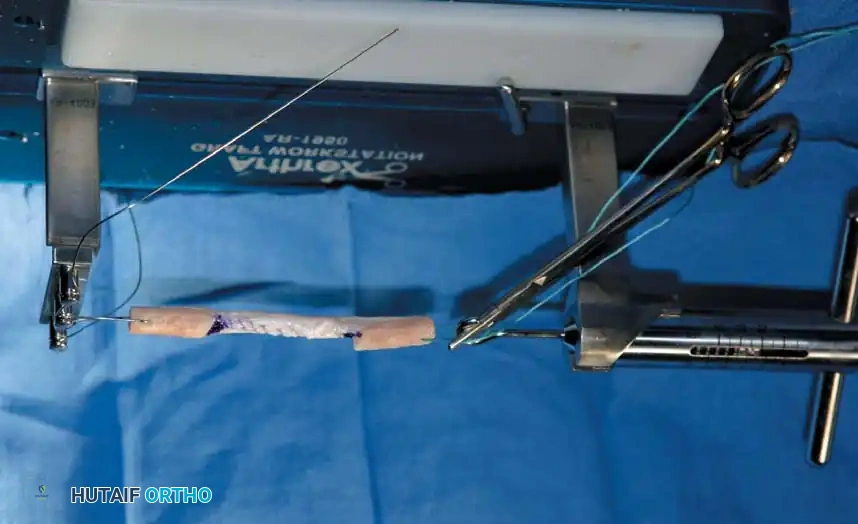
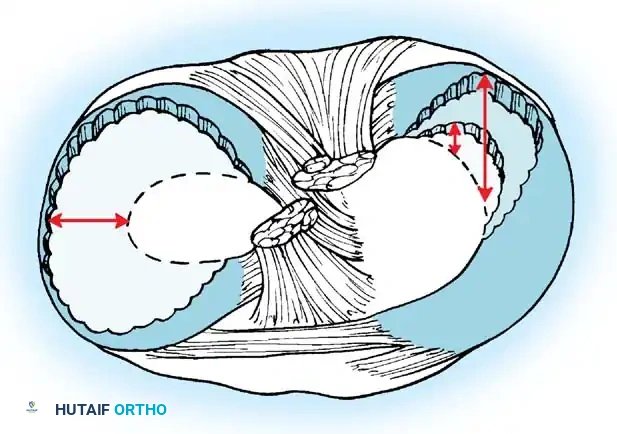
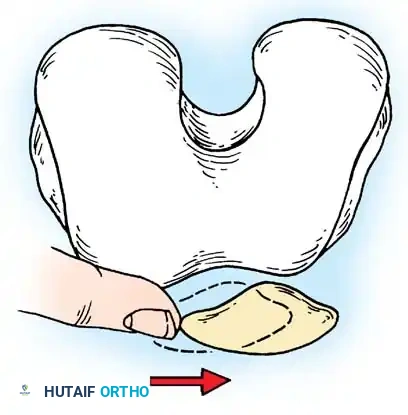
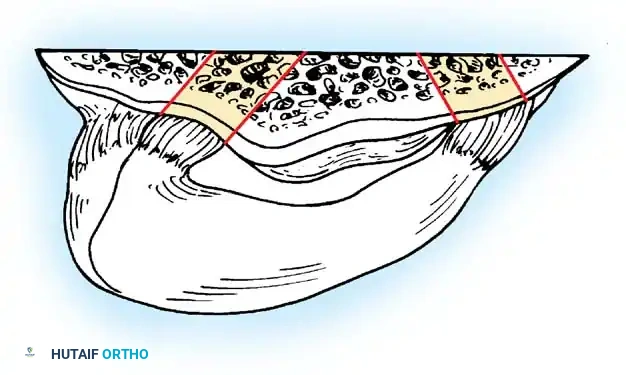
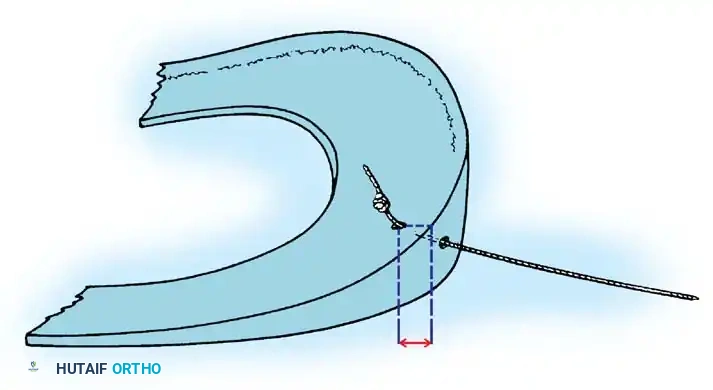
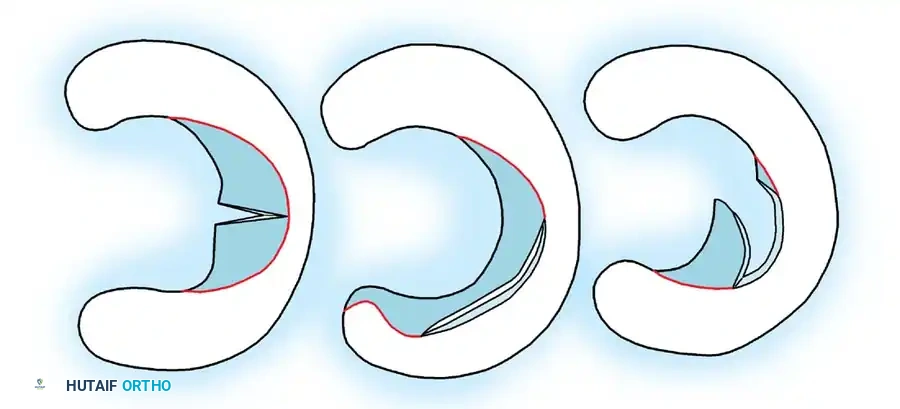
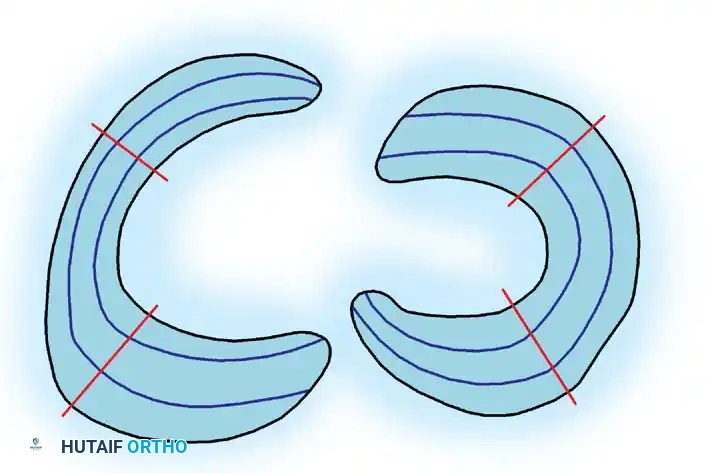
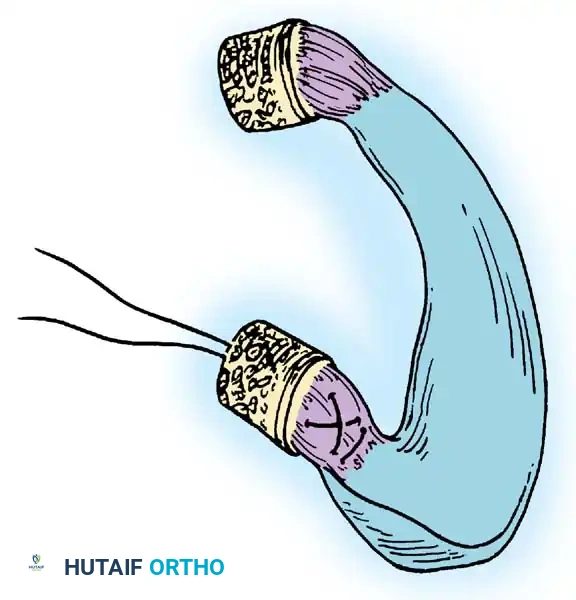
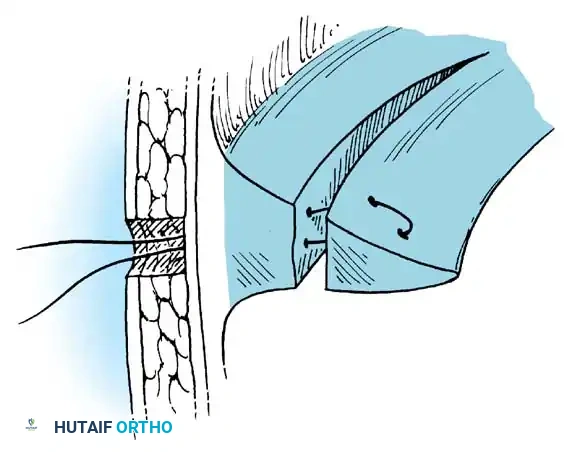
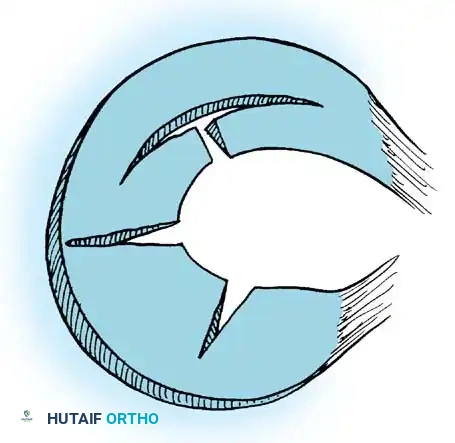
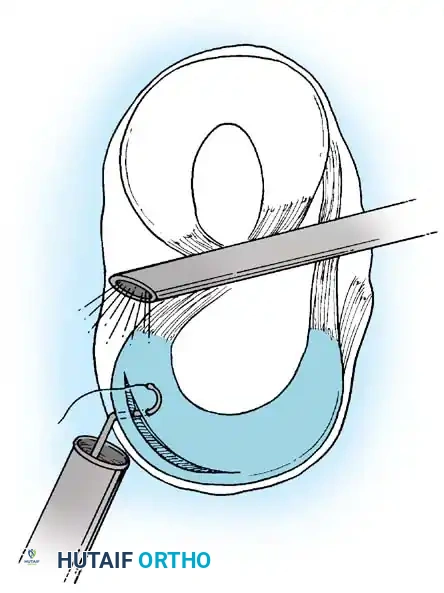
The menisci are highly specialized, C-shaped fibrocartilaginous structures that deepen the articular surfaces of the tibial plateau, providing shock absorption, load transmission, and secondary stabilization. The medial meniscus is larger, more semicircular, and intimately attached to the deep medial collateral ligament (MCL), making it less mobile and more susceptible to shear forces and subsequent tearing. Conversely, the lateral meniscus is more circular, covers a larger portion of the articular surface, and is more mobile due to the lack of strong capsular attachments and the presence of the popliteus hiatus. The vascular supply to the menisci originates from the peripheral genicular arteries, creating distinct functional zones: the peripheral, highly vascularized "red-red" zone; the transitional "red-white" zone; and the avascular, centrally located "white-white" zone. This vascular anatomy dictates the surgical decision-making process between meniscectomy and meniscal repair, as healing potential is strictly limited to the vascularized periphery.
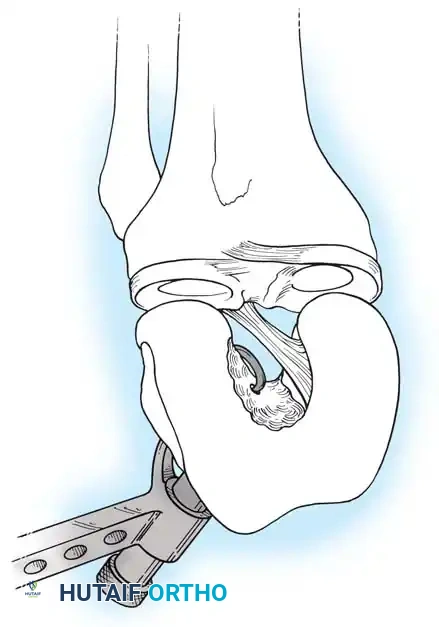
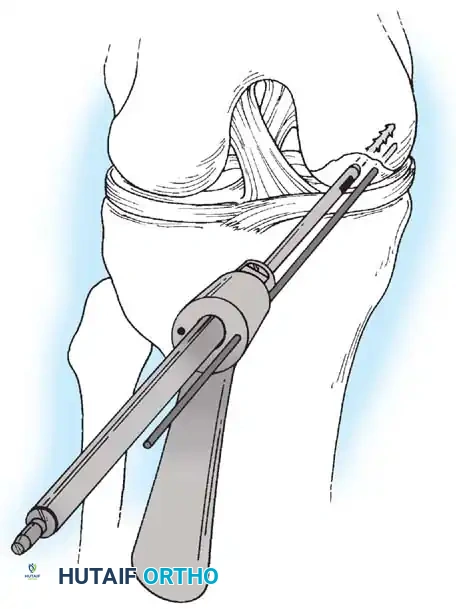
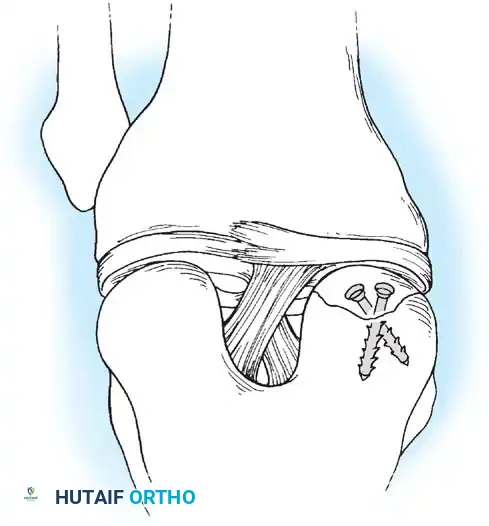
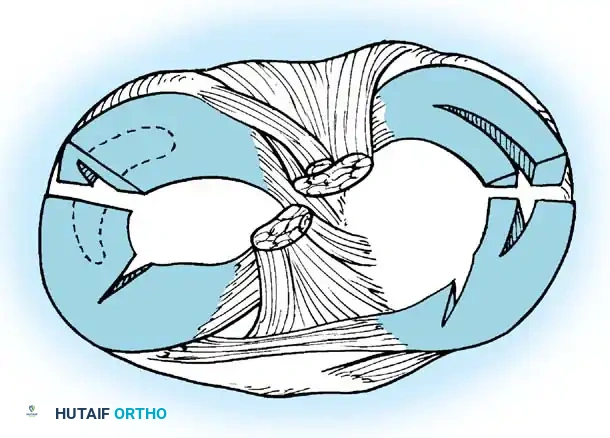
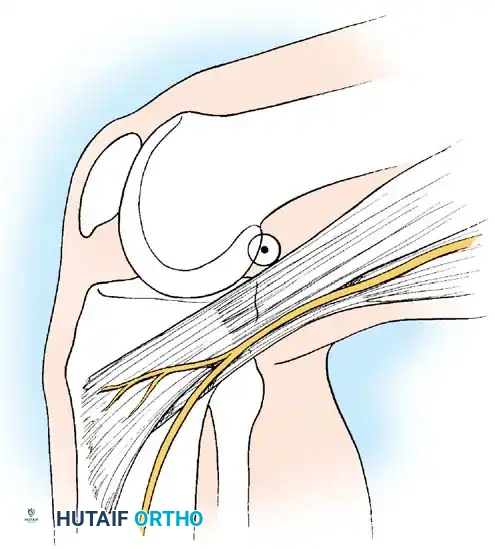
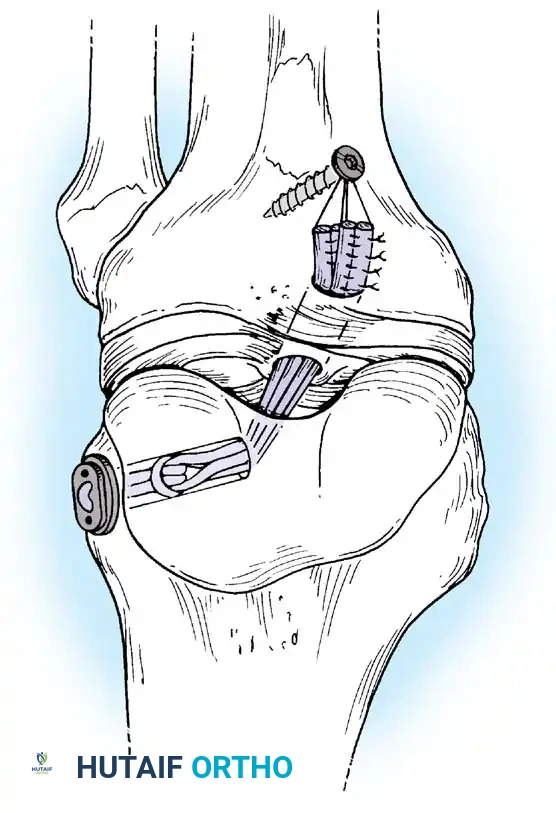
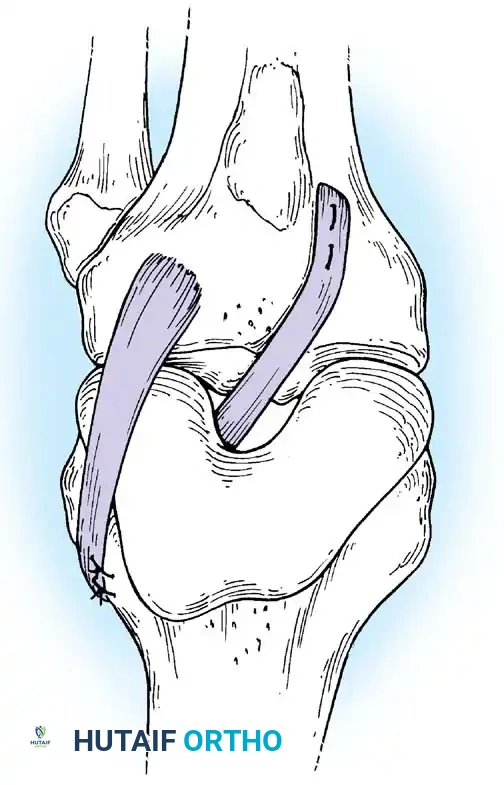
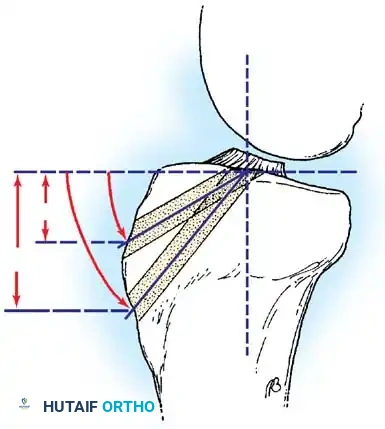
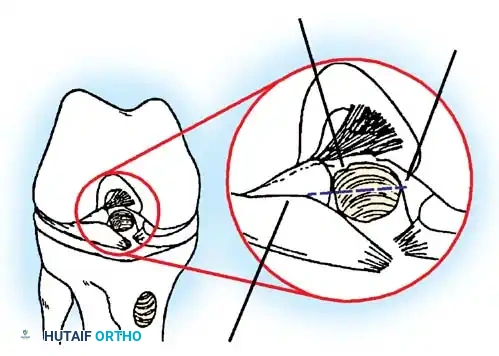
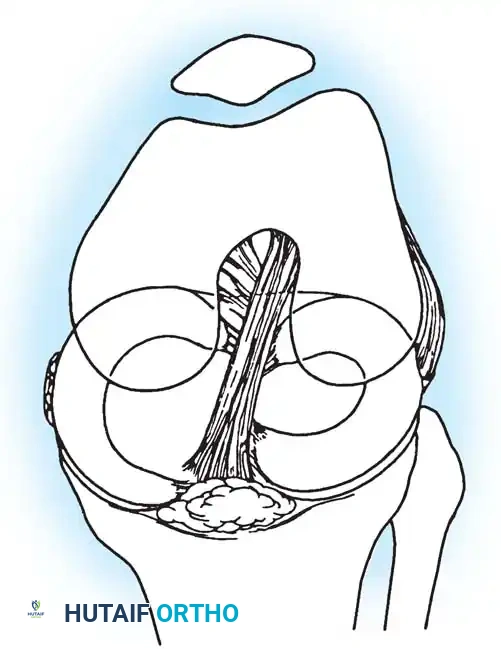
The ligamentous anatomy is visualized arthroscopically primarily within the intercondylar notch. The anterior cruciate ligament (ACL) originates from the posteromedial aspect of the lateral femoral condyle and inserts on the anterior intercondylar area of the tibia. It is composed of the anteromedial (AM) and posterolateral (PL) bundles, which exhibit differential tensioning throughout the arc of motion. The posterior cruciate ligament (PCL), the primary restraint to posterior tibial translation, originates from the anterolateral aspect of the medial femoral condyle and inserts on the posterior tibial sulcus. Arthroscopic evaluation of these structures requires meticulous probing to assess not only continuity but also appropriate tension and synovial coverage. The posterolateral corner (PLC) and posteromedial corner (PMC) are complex capsuloligamentous structures that, while primarily extra-articular, have intra-articular visual correlates that must be assessed, particularly in multi-ligamentous injuries.
The synovial lining of the knee joint is extensive and forms several distinct compartments and recesses, including the suprapatellar pouch, the medial and lateral gutters, and the posterior compartments. Synovial plicae are embryological remnants of the synovial septa that partitioned the joint during fetal development. The most commonly encountered are the suprapatellar plica, the mediopatellar plica (which can become pathologic and cause impingement), and the infrapatellar plica (ligamentum mucosum), which often obscures visualization of the ACL and requires careful resection. Understanding the normal variations of these synovial structures is crucial to avoid misinterpreting them as pathologic entities while ensuring they are addressed if they are contributing to mechanical symptoms or anterior knee pain.



Exhaustive Indications and Contraindications
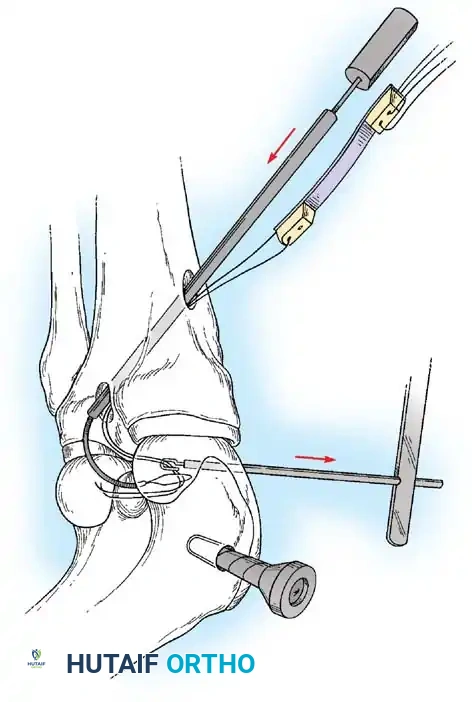
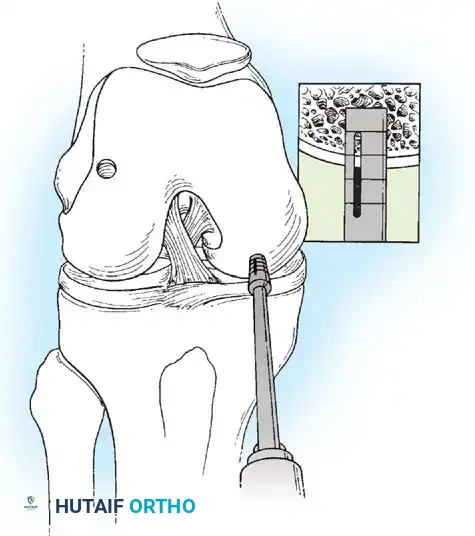
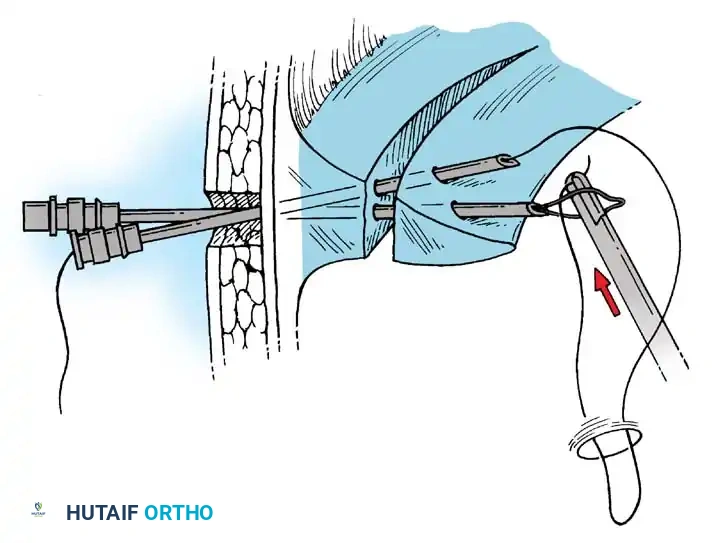
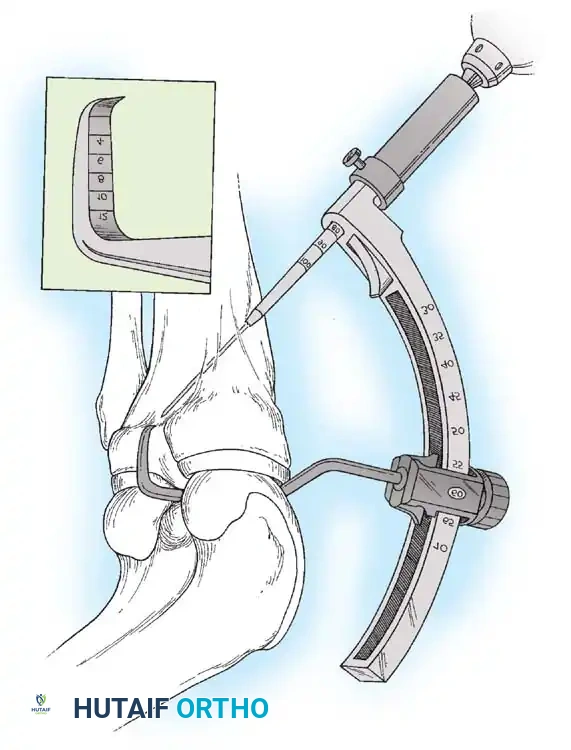
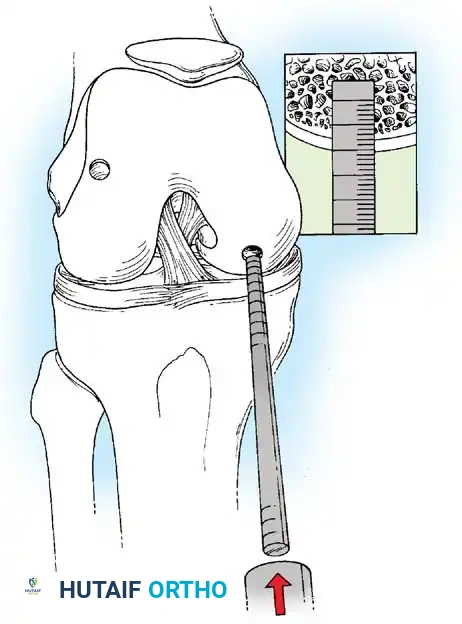
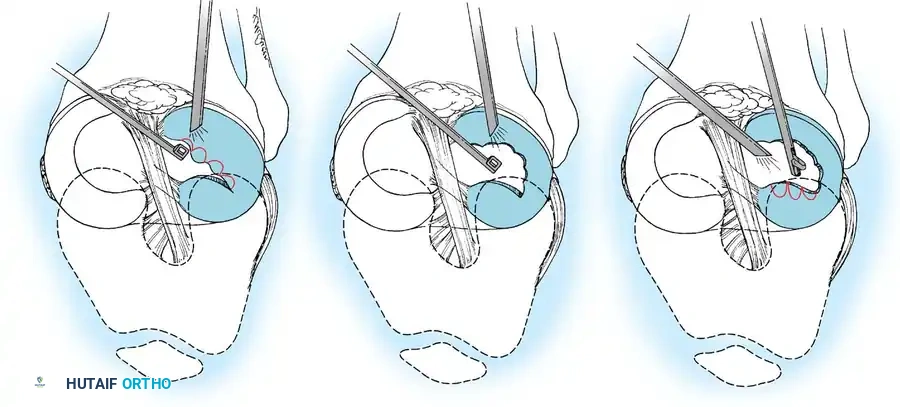
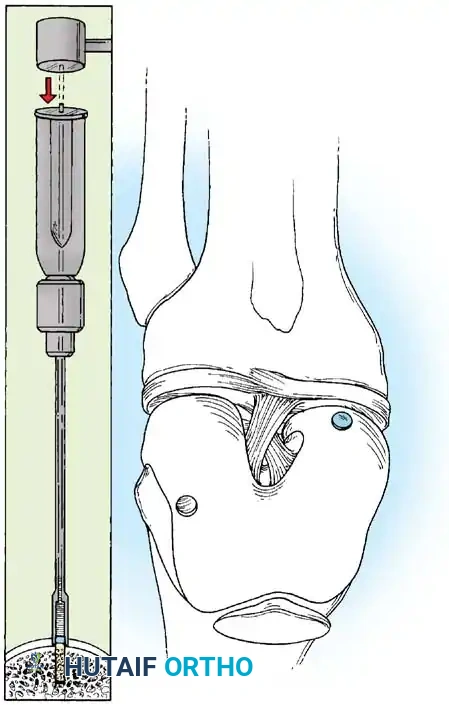
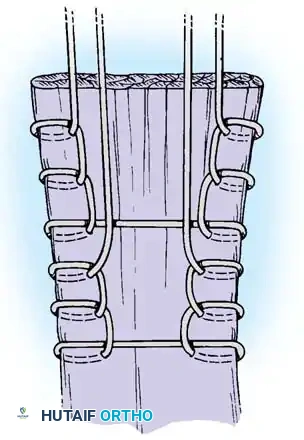
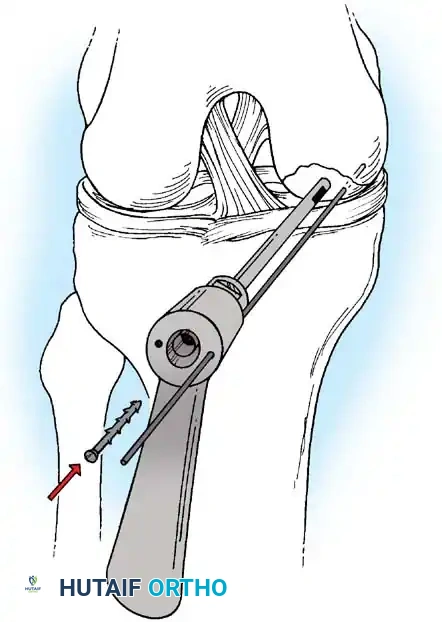
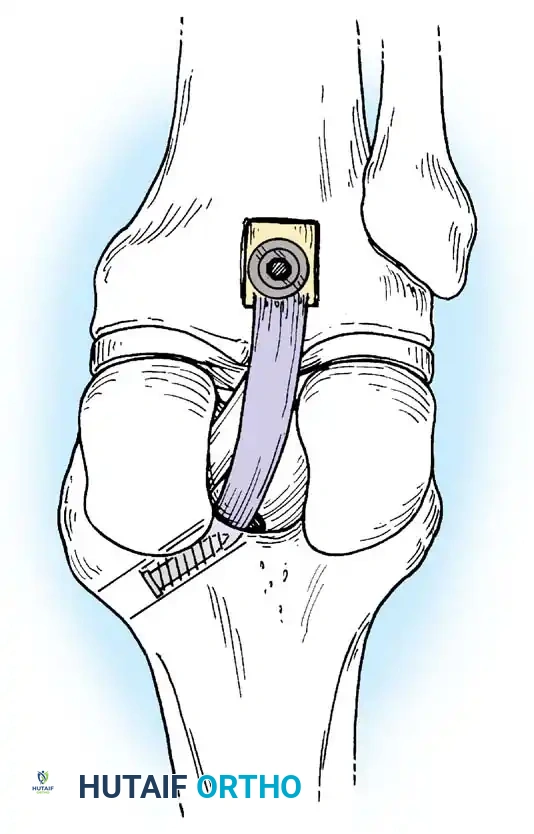
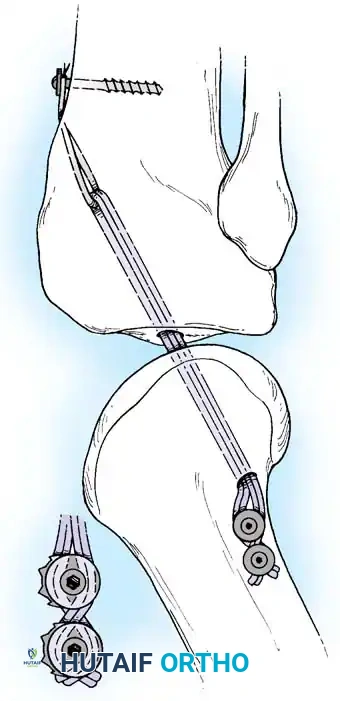
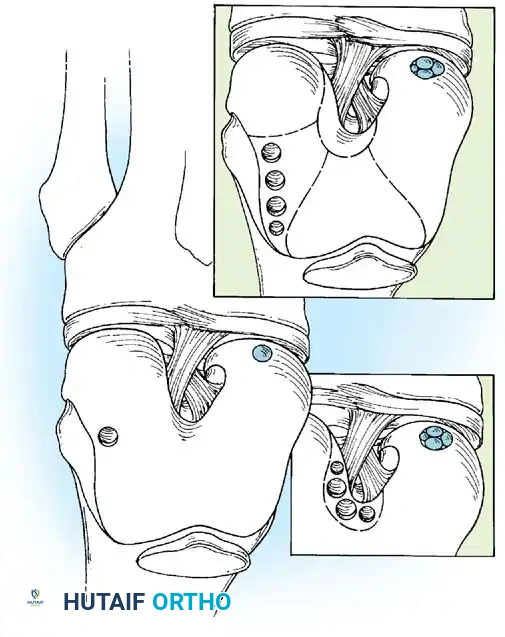
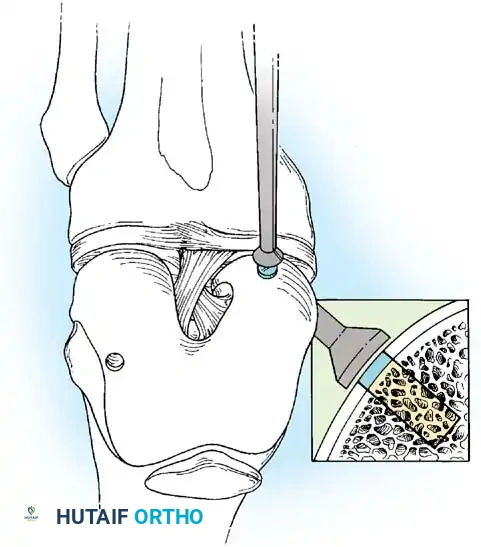
The indications for knee arthroscopy have evolved significantly, shifting from exploratory diagnostics to highly specific therapeutic interventions. The most frequent indication remains the surgical management of meniscal pathology, encompassing both partial meniscectomy for complex, avascular tears and meniscal repair for peripheral, longitudinal tears within the vascular zone. Arthroscopic reconstruction of the cruciate ligaments (ACL and PCL) represents another primary indication, allowing for precise tunnel placement, graft passage, and fixation with minimal morbidity compared to historical open techniques. Furthermore, the management of chondral defects has become increasingly reliant on arthroscopic techniques, ranging from simple chondroplasty and microfracture for small lesions to osteochondral autograft transfer (OATS) and matrix-induced autologous chondrocyte implantation (MACI) for larger, full-thickness defects.
Beyond the common ligamentous and meniscal procedures, arthroscopy is highly indicated for the removal of intraarticular loose bodies, which may arise from osteochondritis dissecans, synovial chondromatosis, or acute osteochondral fractures. Synovectomy is indicated for inflammatory arthritides, such as rheumatoid arthritis or pigmented villonodular synovitis (PVNS), when medical management fails. In cases of acute septic arthritis, emergent arthroscopic irrigation and debridement is the standard of care, offering superior joint lavage and loculation breakdown compared to repeated needle aspirations. Additionally, arthroscopy serves a critical role in the management of arthrofibrosis via lysis of adhesions, and as a preliminary evaluative step prior to proximal tibial osteotomy or unicompartmental knee arthroplasty to ensure the integrity of the compartments that will be subjected to increased load.
Despite its minimally invasive nature, arthroscopy carries specific absolute and relative contraindications that must be rigorously respected. Absolute contraindications include active extra-articular soft tissue infections (e.g., overlying cellulitis or infected abrasions) that risk introducing pathogens into the sterile intraarticular space. Severe, end-stage osteoarthritis with bone-on-bone articulation is generally considered a contraindication for routine arthroscopic debridement, as landmark studies (such as the Moseley trial) have demonstrated no significant benefit over conservative management, unless there is a clear, acute mechanical symptom (e.g., a displaced bucket-handle tear causing a locked knee). Ankylosis or severe loss of motion that precludes the safe introduction of the arthroscope and instruments is also an absolute contraindication.
Relative contraindications require careful clinical judgment and patient optimization. Severe medical comorbidities (e.g., uncontrolled coagulopathy, severe cardiopulmonary disease) may preclude the use of regional or general anesthesia, though local anesthesia with sedation may be an alternative in highly selected cases. A compromised soft tissue envelope, such as extensive scarring from previous trauma or multiple prior surgeries, may make portal placement hazardous and increase the risk of wound healing complications or fistula formation. Finally, complex regional pain syndrome (CRPS) in the affected extremity is a strong relative contraindication, as surgical intervention can severely exacerbate the sympathetic dystrophy.
| Category | Indications for Knee Arthroscopy | Contraindications for Knee Arthroscopy |
|---|---|---|
| Meniscal Pathology | Partial meniscectomy, Meniscal repair, Meniscal root repair, Meniscal allograft transplantation | Degenerative tears in the setting of end-stage osteoarthritis (without mechanical locking) |
| Ligamentous Injury | ACL/PCL reconstruction, Avulsion fracture fixation | Active local extra-articular infection (Absolute) |
| Chondral Defects | Chondroplasty, Microfracture, OATS, MACI | Bone-on-bone osteoarthritis (Relative/Absolute) |
| Synovial/Capsular | Synovectomy (PVNS, Rheumatoid), Lysis of adhesions, Plica excision | Severe ankylosis preventing safe instrument insertion |
| Other Pathology | Loose body removal, Septic arthritis (I&D), Evaluation prior to HTO | Uncontrolled coagulopathy, Severe CRPS (Relative) |


Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is paramount for successful arthroscopic intervention. The choice of anesthesia—local, regional (spinal or epidural), or general—must be tailored to the patient's comorbidities, the anticipated length of the procedure, and the surgeon's experience. While simple diagnostic or minor therapeutic procedures can be performed under local anesthesia in cooperative patients, we prefer an optimized protocol if local is selected: intravenous sedation coupled with portal site injection of 1% lidocaine, and an intraarticular bolus of 30 mL of bupivacaine and 15 mL of lidocaine administered 20 minutes prior to incision. However, for procedures anticipating complex intraarticular surgery or prolonged tourniquet use (>1 hour), general or regional anesthesia is strongly recommended to ensure complete muscle relaxation and patient comfort. Discomfort from the pneumatic tourniquet is a significant limiting factor under local or pure spinal anesthesia without adequate sedation.
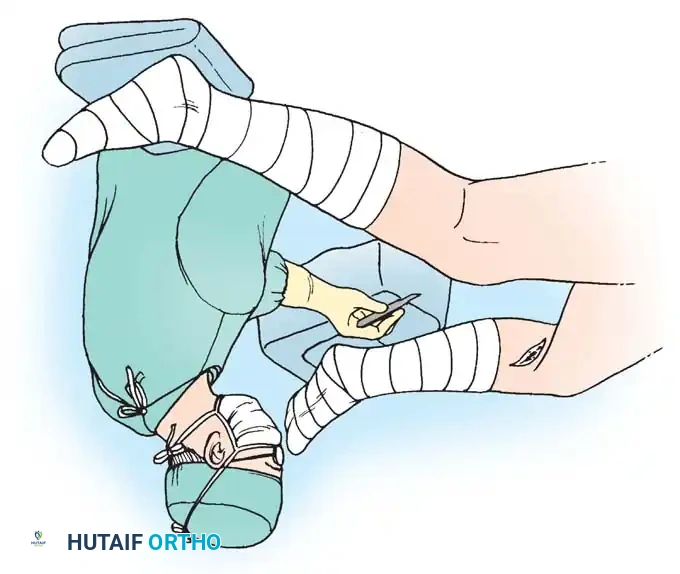
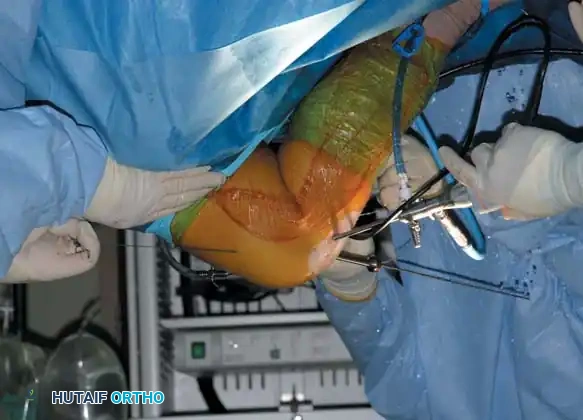
The operating room setup must adhere to strict sterile conditions, as the consequences of an intraarticular infection following arthroscopy are as devastating as those following open arthrotomy. The extremity is sealed proximal and distal to the surgical site, utilizing durable skin preparations such as DuraPrep and iodine-impregnated drapes. Waterproof arthroscopy gowns and drapes with fluid-collection pouches are essential to maintain the sterility of the surgical field and protect the surgical team from fluid contamination. The scrub nurse positions a large instrument table, typically on the operative side, with a Mayo stand placed over the patient's proximal thighs for immediate access to frequently used instruments. High-definition camera systems, fiberoptic light sources, and radiofrequency ablation units are positioned on a designated tower opposite the surgeon for optimal viewing ergonomics.
Fluid management and joint distension are critical components of the preoperative setup. Irrigation fluid can be delivered via gravity (bags suspended 4 to 5 feet above the patient) or through an automated arthroscopic fluid pump. We strongly advocate for the use of an arthroscopic pump system, which maintains a constant intraarticular hydrostatic pressure (typically set between 30 to 45 mmHg) and regulates outflow. This consistent distension often eliminates the need for a pneumatic tourniquet, significantly improving the visualization of meniscal and synovial vascularity—a crucial factor when assessing meniscal healing potential. If a tourniquet is utilized, it is typically applied to the proximal thigh but left uninflated unless troublesome bleeding obscures visualization. Tourniquet time must be strictly monitored and should not exceed 90 to 120 minutes to mitigate the risks of ischemic neurovascular injury and deep vein thrombosis (DVT).
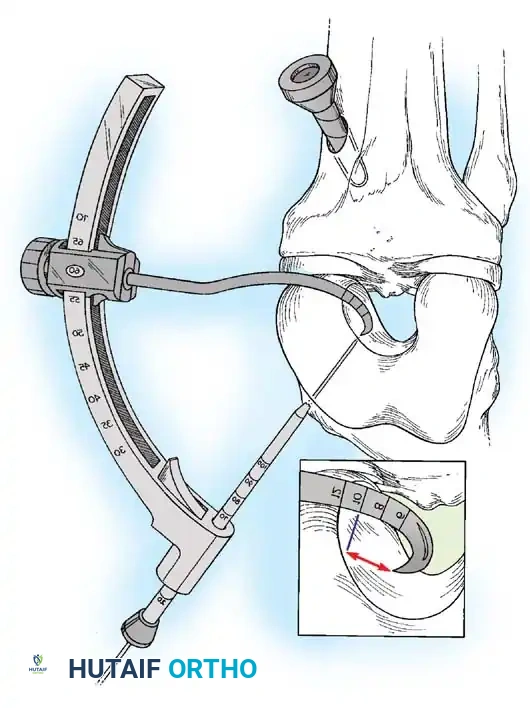
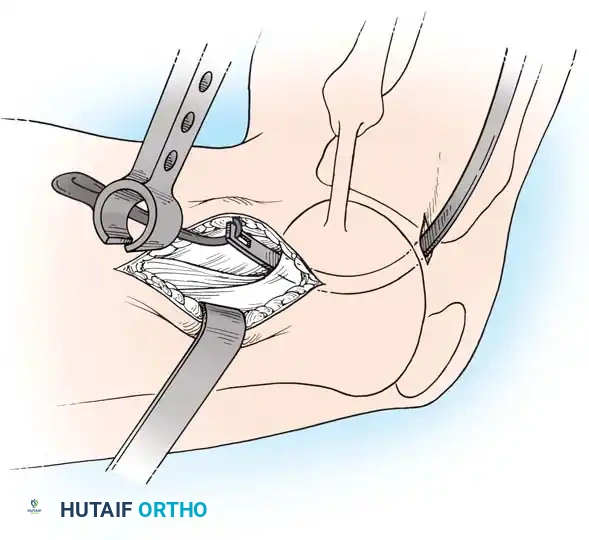
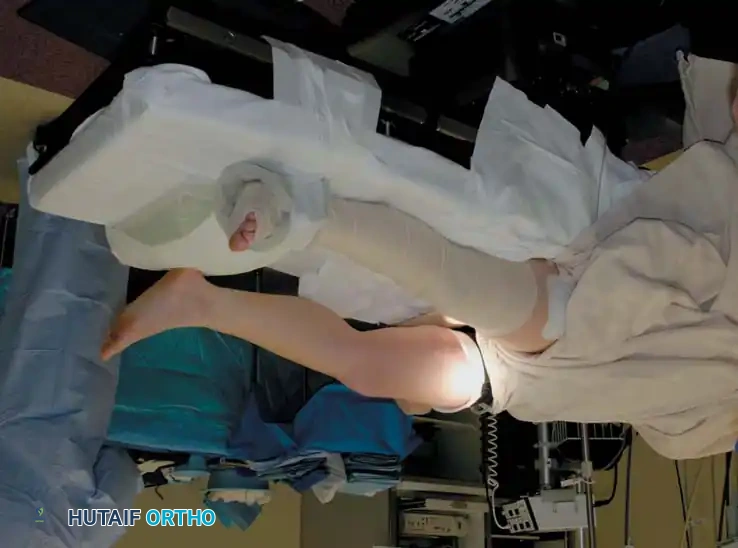
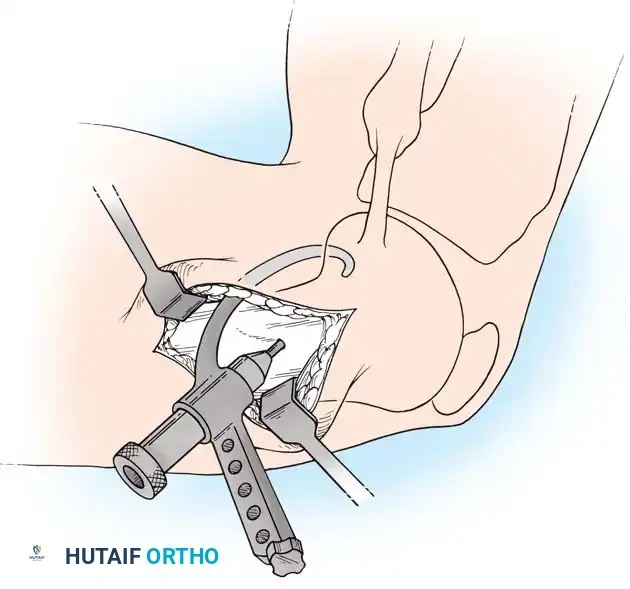
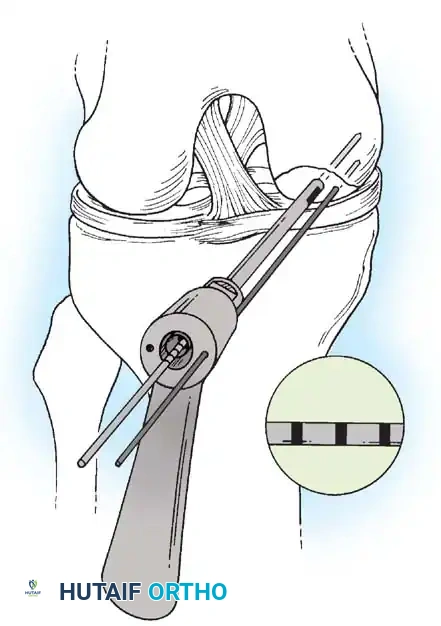
Patient positioning dictates the surgeon's ability to adequately stress the joint and access all compartments. The patient is typically placed supine. The use of a commercial leg-holding device or a padded lateral post is essential for applying valgus and varus stress. When using a leg holder, the operative limb is prepared and draped, and the tourniquet (if used) is positioned within the device. This setup allows the surgeon to stand medial to the abducted leg, utilizing their hip to control the patient's foot and ankle, thereby freeing both hands for instrumentation. Valgus stress is applied by leveraging the leg against the holder, opening the medial compartment. Alternatively, the "table-flat" position or the "dangling" position (where the end of the table is dropped, allowing the knees to flex to 90 degrees) can be employed. In all setups, the contralateral well-leg must be meticulously padded and supported, often wrapped with an elastic bandage or fitted with a compression stocking to minimize venostasis and prevent pressure-induced neuropathies.

Step-by-Step Surgical Approach and Fixation Technique
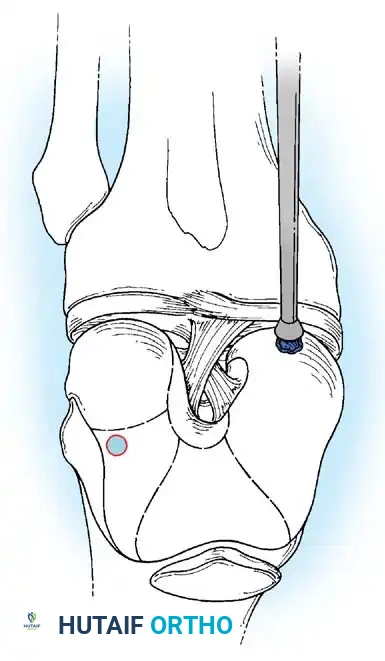
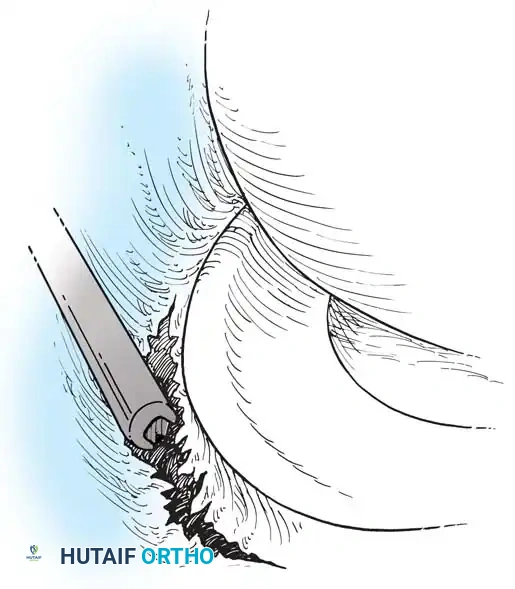
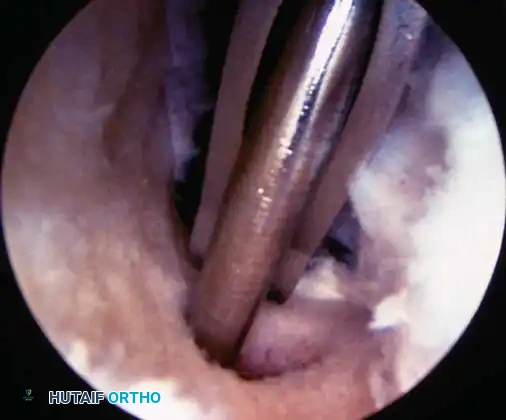
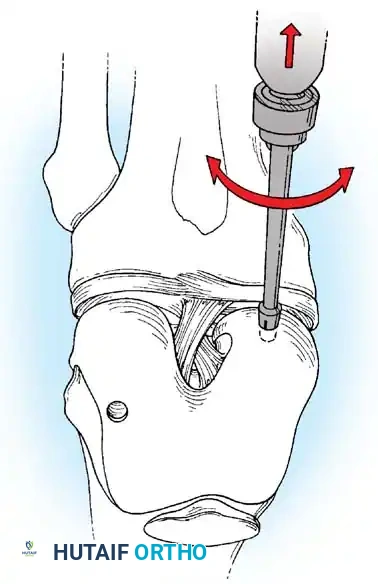
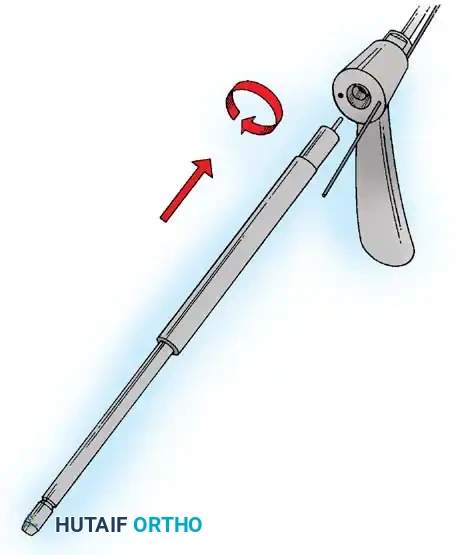
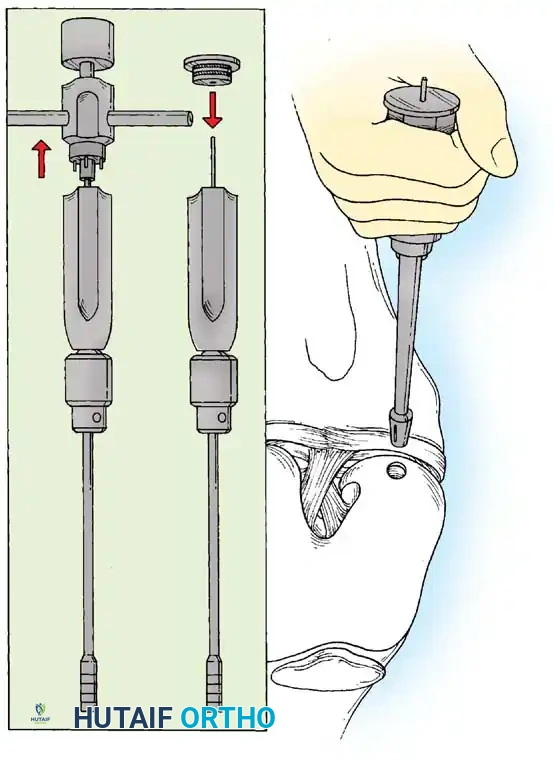
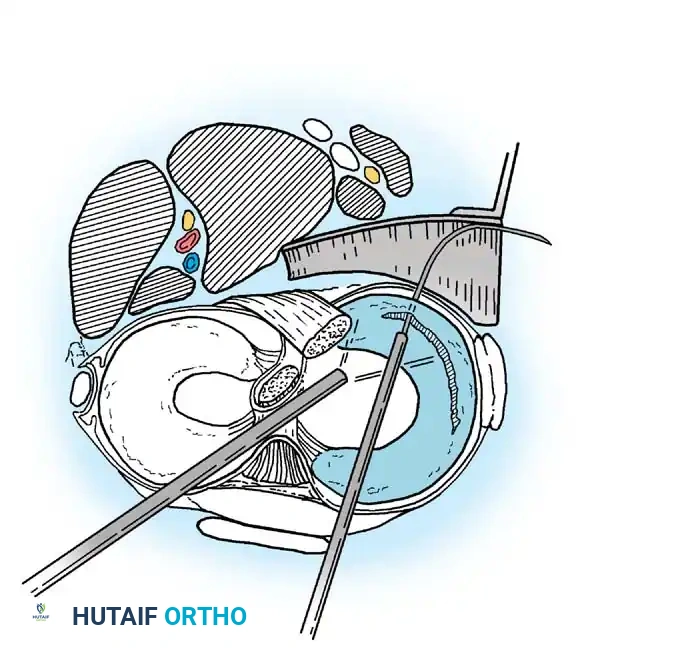
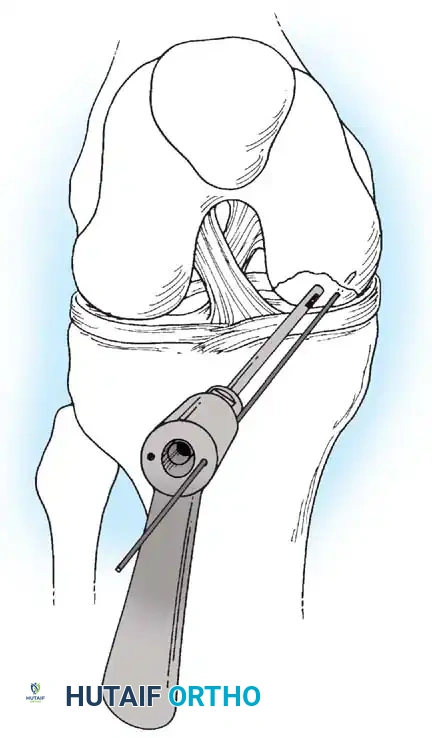
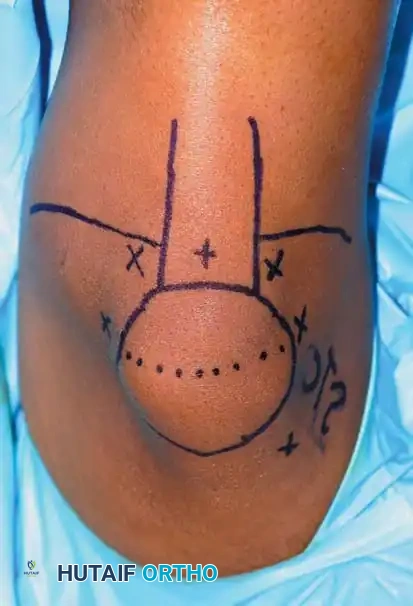
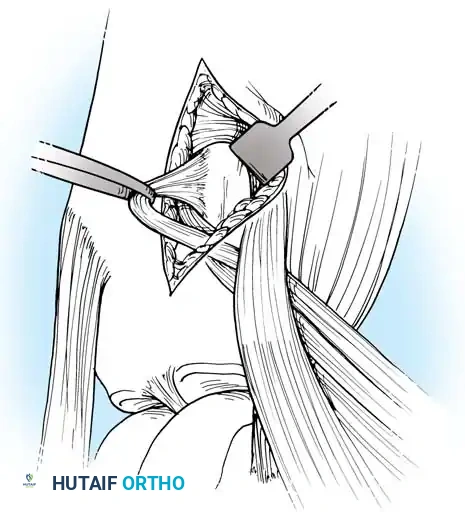
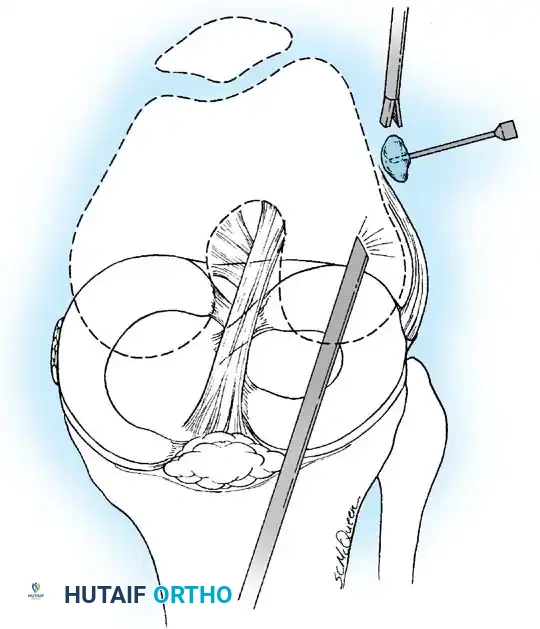
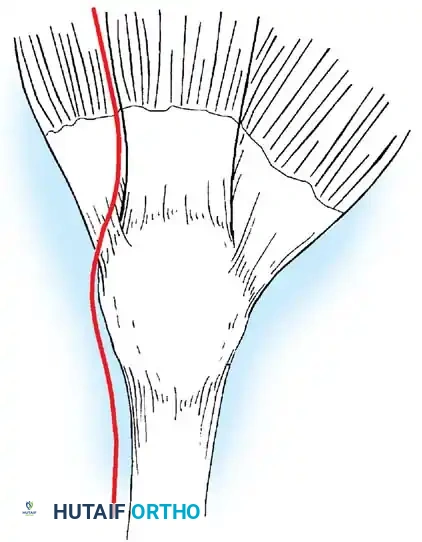
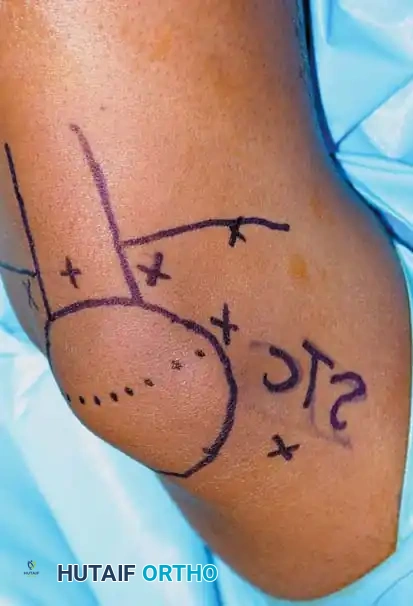
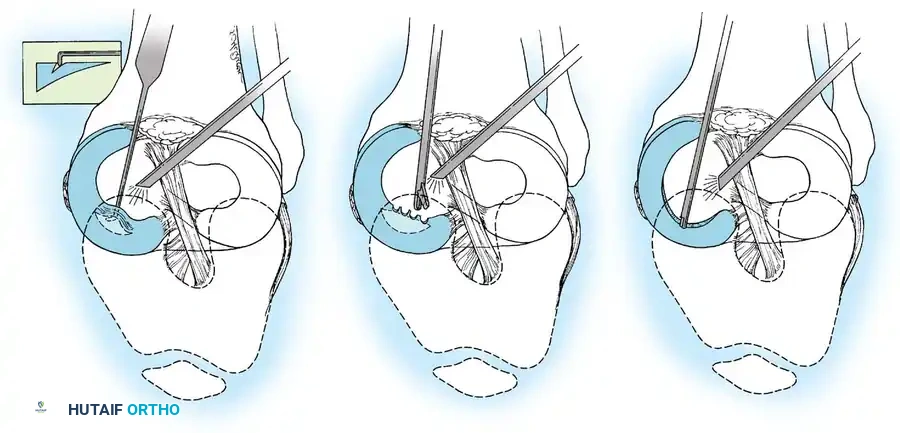
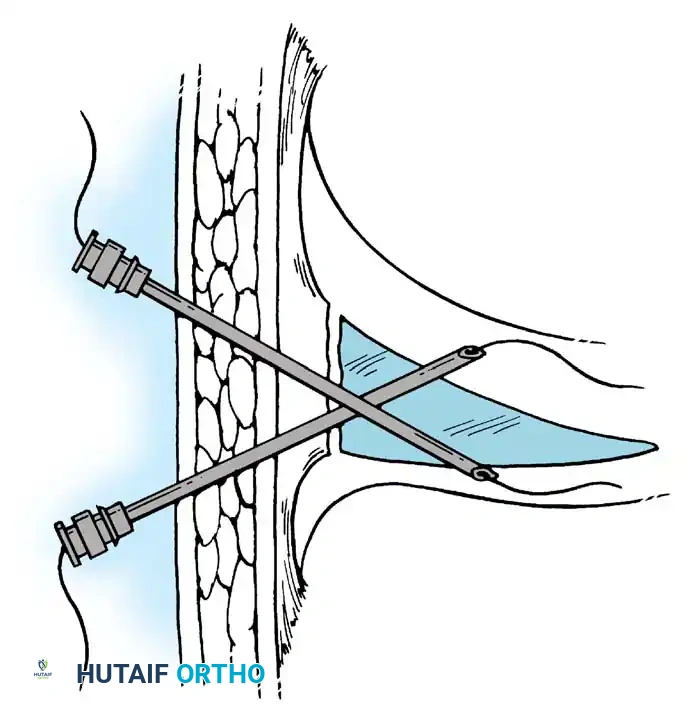
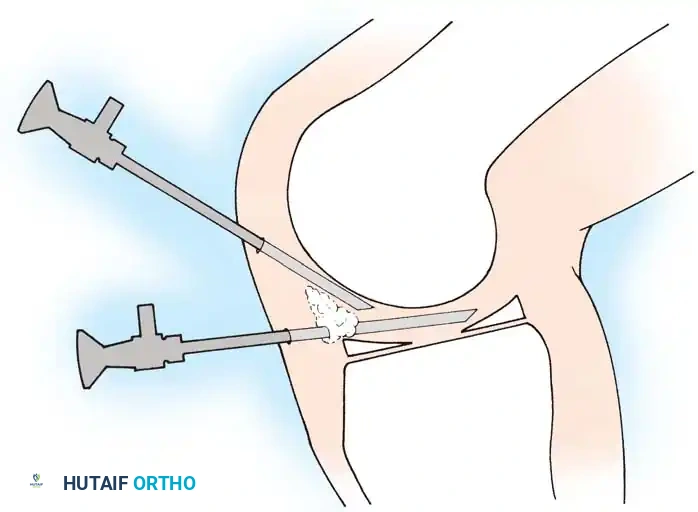
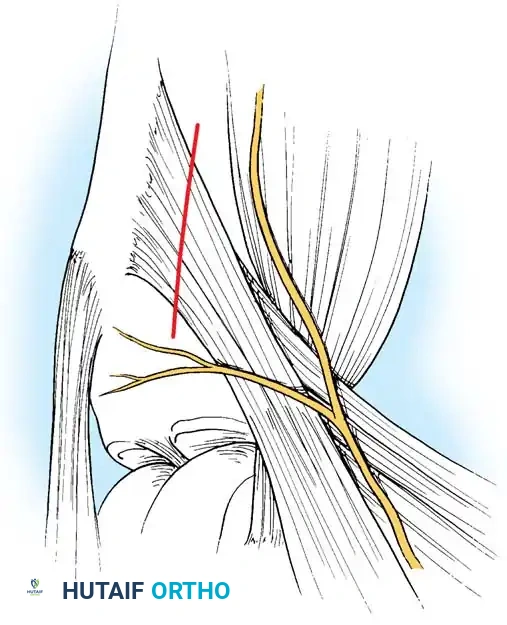
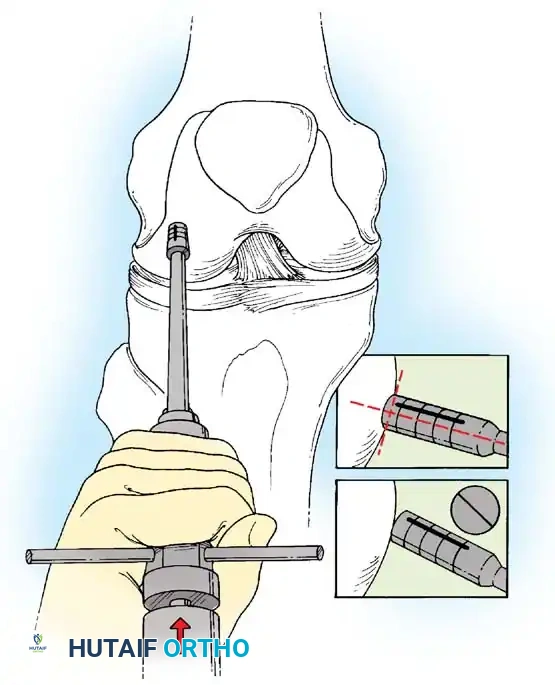
The foundation of a successful arthroscopic procedure lies in precise portal placement. Inadequate portal localization leads to instrument crowding, iatrogenic cartilage damage, and an inability to reach specific anatomic zones. Prior to incision, the bony landmarks—the patella, patellar tendon, medial and lateral joint lines, and tibial tubercle—are meticulously outlined with a sterile surgical marker. The standard anterolateral (AL) viewing portal is established first, typically located 1 cm above the lateral joint line and immediately adjacent to the lateral border of the patellar tendon. A number 11 blade is used to make a vertical or horizontal stab incision, carefully incising only the skin and capsule to avoid damaging the underlying articular cartilage. A blunt trocar is then used to introduce the arthroscope sheath into the intercondylar notch. The anteromedial (AM) working portal is subsequently established under direct intraarticular visualization using a spinal needle for precise localization, ensuring optimal trajectory to the target pathology. Accessory portals, such as superomedial, superolateral, or specialized posterior portals, are established as dictated by the specific surgical requirements.
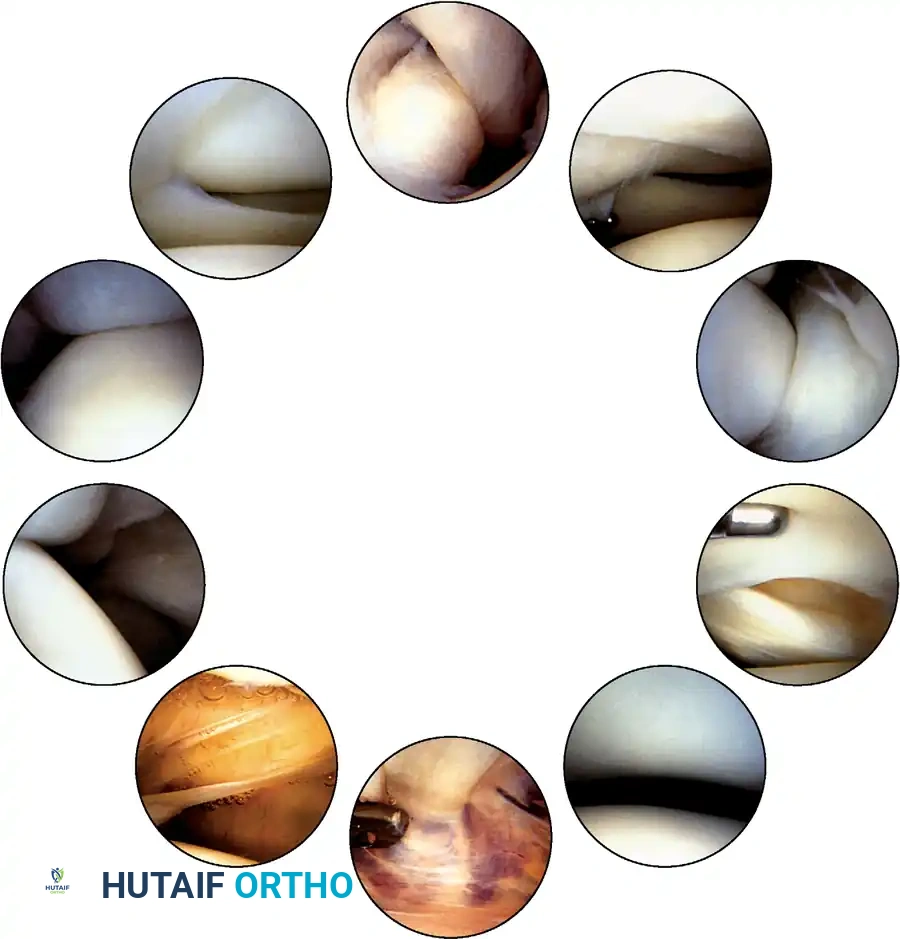
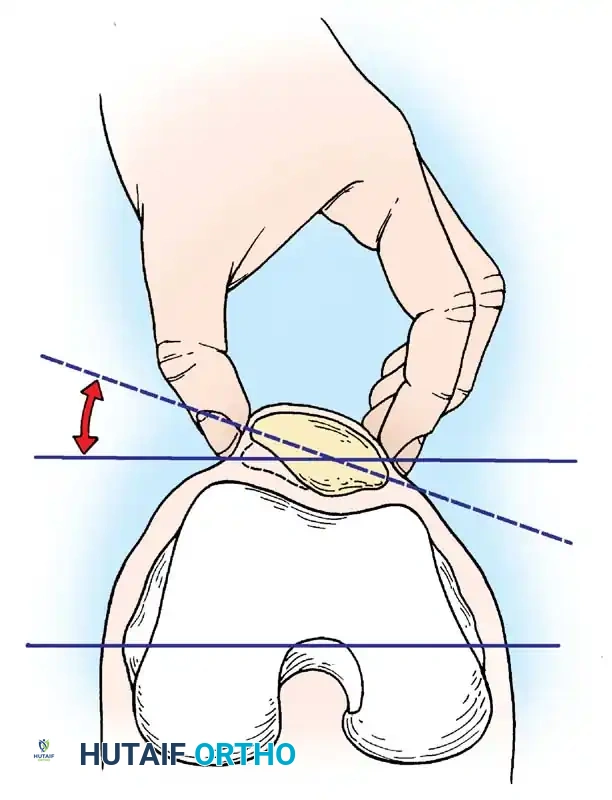
Once the arthroscope is introduced, a systematic, reproducible 15-point diagnostic sweep is mandatory to ensure no pathology is overlooked. The examination begins in the suprapatellar pouch, assessing the synovial lining for plicae, loose bodies, or inflammatory changes. The arthroscope is then retracted to evaluate the patellofemoral articulation. The knee is cycled through a range of motion to assess patellar tracking, congruence, and the integrity of the retropatellar and trochlear articular cartilage. The scope is then swept down the medial gutter to inspect for loose bodies and to visualize the medial capsular reflections.
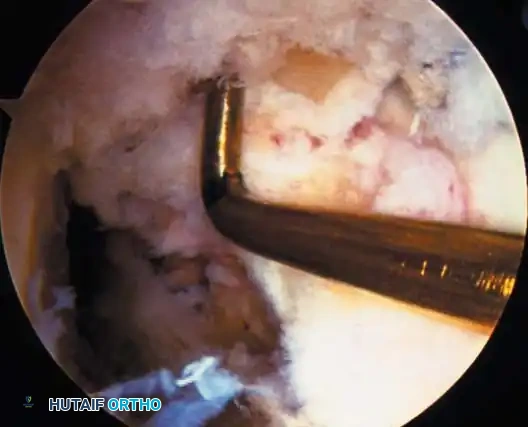
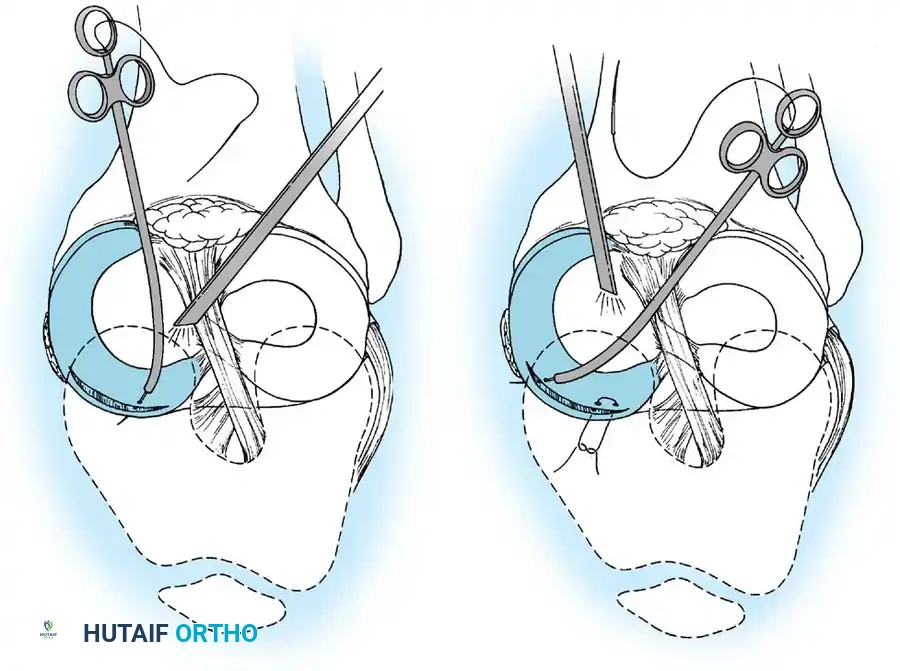
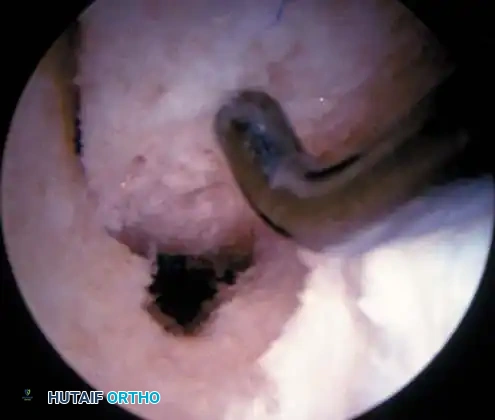
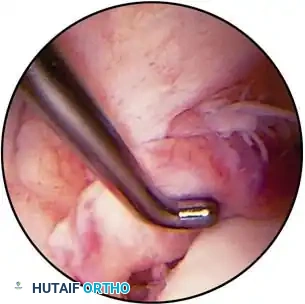
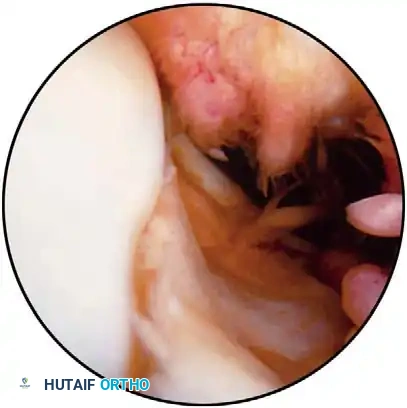
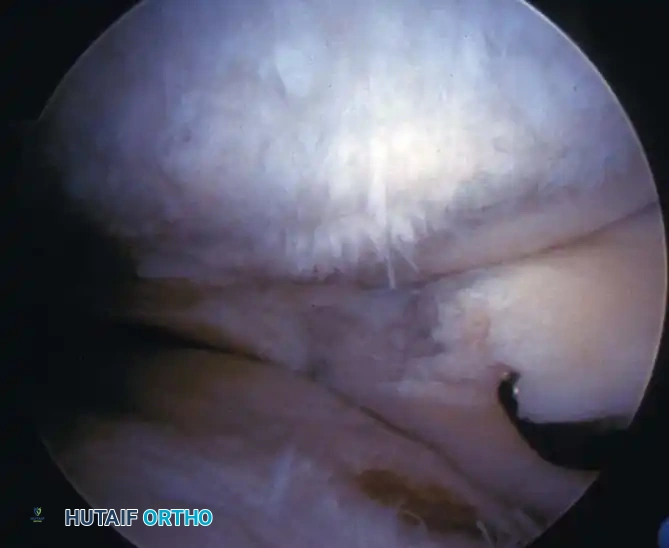
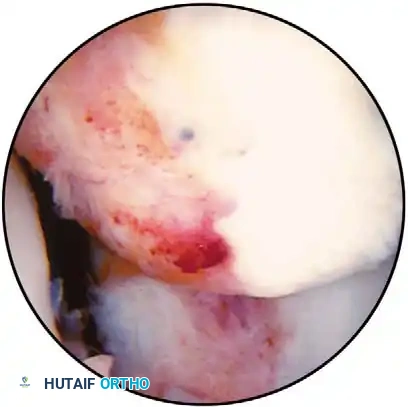
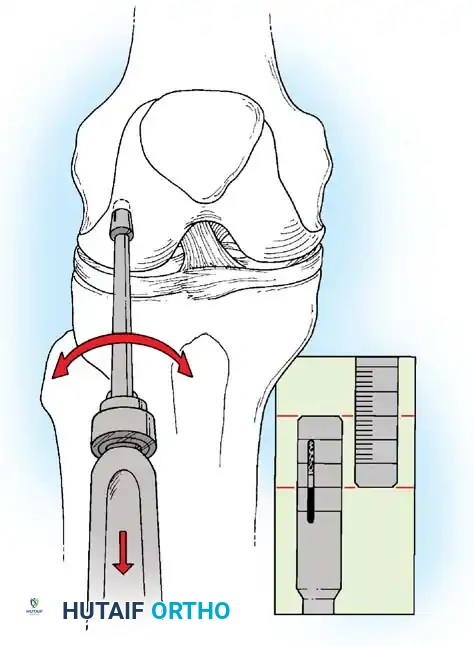
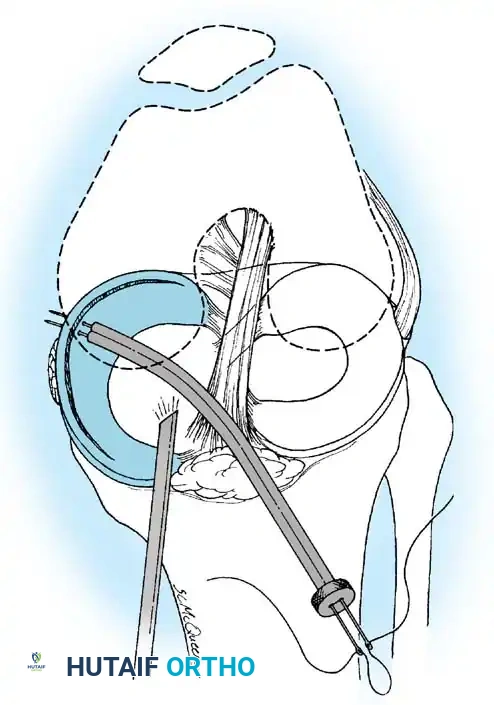
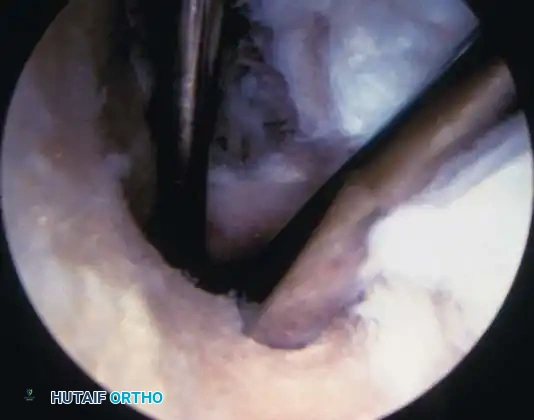
The medial compartment is evaluated next. The surgeon applies a valgus stress with the knee in slight flexion (10 to 30 degrees) to open the joint space. The medial meniscus is systematically probed from its posterior horn, through the body, to the anterior horn. The probe is used to palpate the superior and inferior surfaces of the meniscus, checking for hidden cleavage tears or instability indicative of a peripheral detachment or root tear. The articular surfaces of the medial femoral condyle and medial tibial plateau are concurrently evaluated for chondromalacia, fissuring, or full-thickness defects. Following the medial compartment, the arthroscope is directed into the intercondylar notch to evaluate the cruciate ligaments. The ACL is probed to assess its tension, synovial envelope, and footprint integrity. The PCL is visualized behind the ACL and similarly assessed. The ligamentum mucosum may need to be carefully resected to provide an unobstructed view of the notch.
Evaluation of the lateral compartment requires the knee to be placed in a "figure-four" position (hip flexed, abducted, and externally rotated with the knee flexed) while applying a varus stress. This maneuver opens the lateral joint space, allowing for comprehensive visualization of the lateral meniscus, the lateral femoral condyle, and the lateral tibial plateau. The popliteus tendon is identified within its hiatus, and the mobility of the lateral meniscus is assessed. Finally, the lateral gutter and the posterolateral compartment are inspected. If visualization of the posterior compartments is required (e.g.,
Clinical & Radiographic Imaging Archive










Detailed Chapters & Topics
Dive deeper into specialized chapters regarding arthroscopy-of-the-lower-extremity