Arthroscopic Complications: Prevention, Recognition, and Management

Key Takeaway
Complications in arthroscopy are infrequent but potentially devastating. Mastery of regional anatomy, meticulous preoperative planning, and precise portal placement are paramount. This guide details the prevention and management of fluid extravasation, compartment syndrome, and iatrogenic neurovascular injuries during knee and shoulder arthroscopy, emphasizing evidence-based surgical techniques and strict adherence to universal safety protocols.
Comprehensive Introduction and Patho-Epidemiology
Complications during or after arthroscopy are generally infrequent and, fortunately, are usually minor in severity when viewed across the broad spectrum of orthopedic interventions. However, the minimally invasive nature of arthroscopic surgery can sometimes lull the unwary surgeon into a false sense of security. The reality is that the confined intra-articular spaces, the reliance on two-dimensional video interpretation of three-dimensional anatomy, and the use of high-speed motorized instruments in close proximity to critical neurovascular structures create a unique environment where catastrophic errors can occur in an instant. Most complications are entirely preventable with rigorous preoperative and intraoperative planning, coupled with an uncompromising attention to the details of basic surgical techniques.
The epidemiological landscape of arthroscopic complications has evolved significantly over the past four decades. Early landmark studies, such as the comprehensive retrospective reviews conducted by Small in the 1980s, established baseline complication rates of approximately 0.56% to 1.68% across various joints. Today, as indications for arthroscopy have expanded from simple diagnostic procedures and partial meniscectomies to complex, multi-ligamentous reconstructions, massive rotator cuff repairs, and hip labral reconstructions, the complication profile has shifted. Modern database studies, including analyses of the American Board of Orthopaedic Surgery (ABOS) certification database, indicate that while overall complication rates remain low (typically between 1% and 4%), the severity and complexity of these complications have increased proportionately with the technical difficulty of the procedures being performed.
Mastery of local and regional anatomy is the cornerstone of safe arthroscopy. The operating surgeon must possess a profound, three-dimensional spatial awareness that extends beyond the visible optical cavity. Gaining familiarity with new techniques through accredited learning centers, operating alongside experienced colleagues, reviewing unedited surgical videos, and staying current with peer-reviewed specialty journals allows the surgeon to assimilate valuable information from the collective experiences of the orthopedic community. The learning curve for advanced arthroscopic procedures is steep, and the incidence of iatrogenic injury is inversely proportional to the surgeon's case volume and specific training in that anatomical domain.
The most effective management of an arthroscopic complication is its absolute prevention. A deep, three-dimensional understanding of joint anatomy and the biomechanical behavior of arthroscopic instruments is non-negotiable for the operating surgeon. Surgeons must adopt a philosophy of hyper-vigilance, recognizing that an arthroscopic procedure is not merely a "scope" but a major surgical intervention governed by the same strict physiological and anatomical rules as open surgery. Anticipation of anatomical variants, meticulous fluid management, and disciplined portal placement form the triad of safe arthroscopic practice.
Detailed Surgical Anatomy and Biomechanics
The genesis of many arthroscopic complications—ranging from iatrogenic cartilage damage to poor visualization and frank neurovascular injury—lies in suboptimal portal placement and a failure to respect the underlying regional anatomy. Portals must be established with absolute precision, respecting the underlying intra-articular structures and the trajectory required for instrumentation. In the knee, the standard anterolateral and anteromedial portals are the workhorses of the procedure. The anatomical "slot" between the femoral condyle and the tibial plateau dictates the safe passage of instruments. The infrapatellar branch of the saphenous nerve is highly variable and frequently crosses the anteromedial portal site; recognizing this variability is essential to minimize the risk of painful postoperative neuromas.
The biomechanics of cannula trajectory are critical to the success and safety of the procedure. When establishing portals, the angle of obliquity determines the surgeon's ability to navigate the joint. If the portal is positioned too high (superiorly), the angle of obliquity becomes too steep. This trajectory causes the instruments to abut the femoral condyle, making it biomechanically impossible to visualize or instrument the posterior horn of the meniscus without levering against the articular cartilage and causing iatrogenic chondral injury. Conversely, if the portal is placed too low (inferiorly), the cannula can inadvertently penetrate directly through the anterior horn of the meniscus, causing iatrogenic tearing and severely limiting both the field of view and the mobility of the arthroscope.
FIGURE 49-10: Ideal placement of the cannula. If it is positioned too high, the angle of obliquity is such that the posterior horn cannot be seen; if it is too low, the cannula can go through the meniscus and limit view or mobility. Ideal placement is directly in the slot between the femur and tibia.
In shoulder arthroscopy, the anatomical hazards are equally unforgiving. The axillary nerve and the cephalic vein represent the primary structures at risk during portal placement. The branches of the axillary nerve that course along the deep surface of the deltoid muscle (approximately 5 cm distal to the lateral acromial edge) may be injured if either the anterior or posterior portal sites are placed too far inferiorly. The standard posterior portal must be placed exactly 2 cm inferior and 1 cm medial to the posterolateral corner of the acromion to stay well within the "safe zone." Furthermore, the cephalic vein, residing in the deltopectoral groove, is vulnerable during the creation of the anterior portal if the trajectory deviates medial to the coracoid process.
Beyond static anatomy, the biomechanics of fluid dynamics within the closed joint space must be thoroughly understood. Arthroscopy relies on fluid distention to maintain the optical cavity and provide hemostasis. The joint capsule possesses a specific compliance curve; once maximum volume is reached, internal pressure rises exponentially. This pressure is transmitted to the surrounding capsular tissues and, if capsular integrity is breached, to the adjacent fascial compartments. Understanding the hydrostatic pressure gradient between the arthroscopic pump system, the intra-articular space, and the surrounding capillary beds is paramount in preventing fluid extravasation and subsequent compartment syndrome.
Exhaustive Indications and Contraindications
The decision to proceed with arthroscopic surgery must be predicated on a rigorous risk-benefit analysis, weighing the potential for functional improvement against the inherent risks of the procedure. While arthroscopy is indicated for a vast array of intra-articular pathologies—including meniscal tears, ligamentous ruptures, labral pathology, and localized chondral defects—it is not a panacea. The surgeon must carefully evaluate the patient's physiological status, the chronicity of the pathology, and the anatomical feasibility of an arthroscopic approach. Expanding indications into highly complex reconstructions demand an honest appraisal of the surgeon's skill set and the facility's equipment capabilities.
Absolute contraindications to arthroscopy are relatively few but must be strictly respected to avoid devastating outcomes. Active localized soft tissue infection or systemic sepsis precludes elective arthroscopy due to the risk of seeding the joint or exacerbating systemic illness. Severe ankylosis or profound joint stiffness, where the joint space cannot be adequately distended or navigated without applying excessive, cartilage-crushing force, is another absolute contraindication. In such scenarios, the risk of iatrogenic neurovascular injury, instrument breakage, and catastrophic chondral damage far outweighs any diagnostic or therapeutic benefit.
Relative contraindications require nuanced clinical judgment. Severe, end-stage osteoarthritis with complete loss of joint space makes arthroscopic navigation exceedingly difficult and is generally associated with poor clinical outcomes, often accelerating the need for arthroplasty. Patients with profound coagulopathies or those on aggressive, unyielding anticoagulation therapy present significant risks for postoperative hemarthrosis and subsequent arthrofibrosis. Furthermore, distorted regional anatomy due to prior trauma, massive heterotopic ossification, or previous complex surgeries significantly alters the standard portal safe zones, demanding advanced imaging and potentially an open approach.
Table of Indications and Contraindications
| Clinical Scenario / Procedure | Primary Indications for Arthroscopic Intervention | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Knee: Meniscal Pathology | Symptomatic acute tears, mechanical locking, bucket-handle tears in young patients. | Active joint infection, severe bony ankylosis preventing flexion/extension. | End-stage tricompartmental osteoarthritis, severe uncorrected malalignment. |
| Shoulder: Rotator Cuff | Full-thickness tears, symptomatic partial tears failing conservative management. | Active cellulitis over portal sites, advanced cuff tear arthropathy (Hamada 4/5). | Parkinson's disease (high failure rate), profound cervical radiculopathy mimicking shoulder pain. |
| Hip: Femoroacetabular Impingement | Symptomatic cam/pincer lesions, labral tears, failed conservative therapy. | Acetabular protrusion, severe hip dysplasia (LCEA < 20 degrees). | Advanced joint space narrowing (< 2mm), severe obesity limiting distraction. |
| Ankle: Osteochondral Lesions | Symptomatic OLTs, loose bodies, anterior impingement syndromes. | Active localized infection, severe peripheral vascular disease (ischemia risk). | Charcot arthropathy, severe end-stage tibiotalar arthritis. |
Pre-Operative Planning, Templating, and Patient Positioning
Before any operative procedure commences, having all comprehensive office notes, advanced imaging (MRI/CT), and plain radiographs available in the operating room is mandatory. The cognitive rehearsal of the procedure, including the anticipation of potential anatomical variants, significantly reduces intraoperative errors. Templating, while traditionally associated with arthroplasty, is equally vital in complex arthroscopy. For example, in anterior cruciate ligament (ACL) reconstruction, measuring the native footprint and calculating expected graft lengths and tunnel trajectories on preoperative MRI can prevent catastrophic intraoperative complications such as tunnel blowout or graft-tunnel mismatch.
Wrong-site surgery remains a catastrophic, yet entirely preventable, "never event" in orthopedic surgery. The psychological devastation to the patient and the career-altering medicolegal implications for the surgeon cannot be overstated. Historically, having the patient write the word “wrong” on the nonoperative extremity was utilized to alleviate possible confusion on a long, fatiguing operative day. Today, standardized, universally mandated protocols have superseded this archaic practice. The Sign Your Site program initiated by the American Academy of Orthopaedic Surgeons (AAOS) and the Universal Protocol recommendations mandated by the Joint Commission dictate a strict sequence of preoperative verification that must be executed without exception.
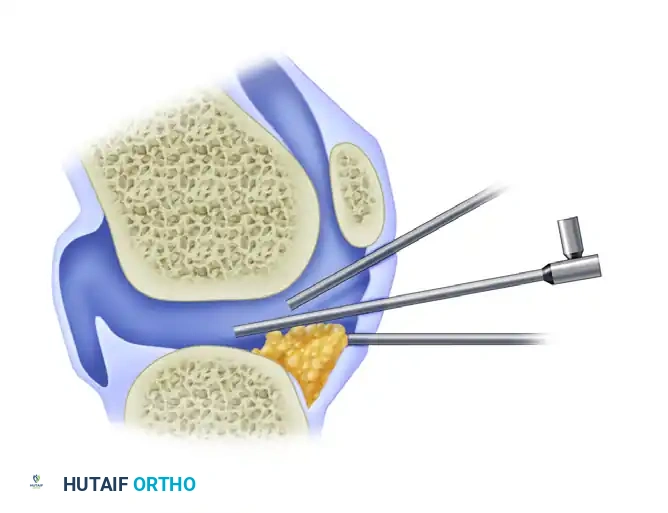
FIGURE 49-9: The operative extremity has been clearly marked by the surgeon prior to draping, adhering to the Universal Protocol to prevent wrong-site surgery.
Patient positioning is a critical phase of preoperative planning that directly impacts both surgical access and complication prevention. In shoulder arthroscopy, the choice between the lateral decubitus and the beach chair position carries distinct risk profiles. The beach chair position offers excellent anatomical orientation and ease of conversion to an open procedure, but it carries the severe risk of cerebral hypoperfusion and catastrophic ischemic brain injury if mean arterial pressure is not meticulously maintained. Conversely, the lateral decubitus position provides excellent joint distraction but places the brachial plexus at significant risk for traction neurapraxia. The biomechanical position that appears to result in the greatest traction tension on the brachial plexus is 30 degrees of forward elevation combined with 70 degrees of abduction. Traction weight must be strictly limited (typically 10-15 lbs), and the cervical spine must be maintained in a neutral alignment.
Tourniquet management and fluid pump calibration are the final steps before incision. In knee arthroscopy, if a tourniquet is utilized, it must be well-padded and calibrated to the patient's systolic blood pressure (typically 100 mm Hg above systolic) to minimize ischemic nerve injury. Arthroscopic pump systems must be set to the lowest possible pressure required to maintain visualization, typically 30–40 mm Hg for the knee and 40-50 mm Hg for the shoulder, adjusting dynamically for the patient's mean arterial pressure. Failure to calibrate the pump correctly is the primary catalyst for massive fluid extravasation and subsequent compartment syndrome.
Step-by-Step Surgical Approach and Fixation Technique
The prevention of intraoperative complications begins with the meticulous execution of portal creation. Portals should be marked appropriately before the joint is distended, utilizing palpable bony landmarks rather than relying on visual estimation. Once marked, the joint is distended with fluid to displace the neurovascular structures away from the capsule. The surgeon must ensure that the scalpel penetrates the skin only, utilizing a #11 blade to avoid deep plunging. Subsequently, a hemostat should be used to spread the subcutaneous tissues down to the joint capsule, gently pushing away superficial nerves and vessels. Finally, blunt trocars should be routinely used to enter the joint capsule; the use of sharp trocars is a historical practice fraught with the risk of scuffing the articular cartilage and lacerating intra-articular structures.
Once the optical cavity is established, intra-articular navigation must proceed with disciplined, systematic precision. The arthroscope should be swept through the joint in a standardized sequence to ensure no pathology is missed and to establish spatial orientation. When introducing instruments through the working portals, the surgeon must adhere to the cardinal rule of arthroscopy: never advance an instrument blindly. The tip of the motorized shaver, radiofrequency wand, or biting punch must be visualized at all times. In the knee, clearing the infrapatellar fat pad must be done cautiously to avoid amputating the anterior horn of the lateral meniscus or severing the intermeniscal ligament, which can lead to catastrophic destabilization of the menisci.
Fluid management during the step-by-step approach requires constant vigilance. Fluid can escape the joint capsule through portal sites, iatrogenic capsular rents, or anatomical weak points (such as the popliteus hiatus in the knee). When fluid accumulates in the fascial compartments of the extremity, interstitial pressure rises. If this pressure surpasses the capillary perfusion pressure, tissue ischemia ensues. By utilizing gravity inflow or maintaining lower automated pump pressures and ensuring adequate fluid outflow through a dedicated cannula, the vast majority of extravasation complications can be avoided. The surgeon must routinely palpate the calf and thigh (or the deltoid and pectoral regions in the shoulder) to assess for induration and swelling.
If excessive extravasation is noted intraoperatively, a strict, step-by-step salvage protocol must be initiated immediately. First, halt inflow: immediately stop the fluid inflow and assess the joint for capsular breaches. Second, decompress: release any constricting dressings, drapes, or tourniquets that may be acting as a venous tourniquet. Third, positional drainage: place the extremity at the level of the heart to optimize venous and lymphatic return without compromising arterial inflow. Fourth, mechanical milking: wrap the extremity with an Esmarch bandage from distal to proximal, and then remove it. This technique mechanically forces the extravasated fluid out of the interstitial spaces. Persistence of elevated compartment pressure despite these maneuvers is a dire warning sign requiring formal compartment pressure monitoring and potential emergent fasciotomy.
Complications, Incidence Rates, and Salvage Management
Nerve injuries in arthroscopy are rare but can lead to profound postoperative morbidity, chronic pain, and devastating litigation. The mechanisms of nerve injury are multifactorial and include direct trauma (laceration from a scalpel or motorized shaver), traction (neurapraxia from overdistraction), compression (from positioning devices or fluid extravasation), and ischemia. In the knee, the inferior branches of the saphenous nerve and the sartorial branches of the femoral nerve are the most commonly injured. In the shoulder, the axillary nerve and brachial plexus are at highest risk. Complex Regional Pain Syndrome (CRPS) can arise from a poorly defined mechanism following even minor cutaneous nerve damage. Salvage management for neuromas includes surgical resection and burying of the nerve stump deep into muscle or bone, while CRPS requires aggressive multidisciplinary pain management and sympathetic blocks.
Vascular complications, while exceedingly rare (incidence < 0.1%), represent true limb-threatening emergencies. In knee arthroscopy, the popliteal artery is at immense risk during posterior horn meniscectomies, posterior capsular releases, or when establishing posteromedial/posterolateral portals. The use of motorized shavers without direct visualization in the posterior compartment is strictly contraindicated. Blind instrumentation may result in catastrophic hemorrhage or subsequent pseudoaneurysm formation. In the shoulder, the cephalic vein and the axillary artery are vulnerable. If a major vascular injury is suspected intraoperatively (evidenced by pulsatile bleeding, loss of distal pulses, or an expanding hematoma), the procedure must be aborted, direct pressure applied, and an emergent vascular surgery consultation obtained for immediate exploration and repair.
Iatrogenic cartilage damage and instrument breakage are highly frustrating complications that stem directly from poor technique or equipment failure. Scuffing of the femoral condyles or the humeral head often occurs during the initial insertion of the trocar or when levering instruments in a tight joint. Broken instruments, particularly the tips of biting punches or shaver blades, can become lost within the joint recesses. If an instrument breaks, the surgeon must immediately halt fluid flow to prevent the fragment from migrating. The inflow should be turned off, and the fragment localized visually or with fluoroscopy. A magnetic retrieval tool or an arthroscopic grasper must be used to carefully extract the loose body. Leaving a broken metallic fragment in the joint is unacceptable and will lead to rapid, severe third-body wear of the articular cartilage.
Postoperative joint infection (septic arthritis) following arthroscopy has an incidence ranging from 0.1% to 0.4%. Risk factors include prolonged operative times, concurrent open procedures, and patient comorbidities such as diabetes. Septic arthritis presents with severe, escalating pain, massive effusion, and systemic signs of infection, typically 3 to 10 days postoperatively. Salvage management requires emergent arthroscopic irrigation and debridement (often requiring multiple trips to the operating room), copious lavage with normal saline, and targeted intravenous antibiotic therapy based on intraoperative cultures. Delay in recognizing and treating septic arthritis will result in irreversible chondrolysis and permanent joint destruction.
Table of Complications, Incidence Rates, and Salvage Management
| Complication Type | Estimated Incidence | Primary Mechanism / Risk Factor | Immediate Salvage / Management Protocol |
|---|---|---|---|
| Iatrogenic Cartilage Injury | 1.0% - 2.5% | Sharp trocar use, tight joint space, poor portal trajectory. | Document injury, perform localized chondroplasty, alter portal if necessary. |
| Neurological Injury (Sensory) | 0.5% - 1.0% | Direct laceration during portal creation (e.g., saphenous branch). | Observation for neurapraxia; if painful neuroma develops, surgical excision and burying. |
| Vascular Injury (Major) | < 0.1% | Blind posterior instrumentation, aberrant portal placement. | Abort procedure, apply direct pressure, emergent vascular surgery intervention. |
| Compartment Syndrome | < 0.1% | High pump pressure, capsular breach, prolonged operative time. | Halt inflow, mechanical milking, measure pressures (Δp ≤ 30 mm Hg), emergent fasciotomy. |
| Septic Arthritis | 0.1% - 0.4% | Contamination, prolonged surgery, inadequate sterilization. | Emergent arthroscopic I&D, copious lavage, culture-directed IV antibiotics. |
| Instrument Breakage | 0.1% - 0.2% | Metal fatigue, excessive levering of punches/shavers. | Halt fluid flow immediately, localize fragment (visually/fluoroscopically), magnetic/grasper retrieval. |
Phased Post-Operative Rehabilitation Protocols
The prevention of complications extends seamlessly into the postoperative period. Immediate Post-Anesthesia Care Unit (PACU) monitoring must include a thorough, documented neurovascular assessment of the operative extremity. Vascular assessment requires checking capillary refill, distal pulses, and compartment compressibility. Neurological assessment demands that the motor function and sensory distribution of the major peripheral nerves be verified before the patient is considered for discharge. Disproportionate postoperative pain that is unresponsive to standard, appropriate analgesia is a blaring red flag. It must never be dismissed as "low pain tolerance"; rather, it may indicate impending compartment syndrome or the early onset of Complex Regional Pain Syndrome (CRPS).
Phase I of rehabilitation focuses on tissue protection and aggressive edema control. The physiological trauma of arthroscopy, including joint distension and capsular penetration, results in an obligatory inflammatory response. Cryotherapy and compressive dressings are essential to mitigate hemarthrosis and swelling, which can otherwise lead to reflex muscle inhibition (particularly of the quadriceps) and severe pain. Weight-bearing status and range-of-motion restrictions must be strictly tailored to the specific procedure performed. For example, isolated meniscectomies may allow immediate weight-bearing, whereas complex meniscal repairs or massive rotator cuff repairs require rigid immobilization to protect the biological healing of the fixation construct. The danger lies in balancing the risk of overly aggressive early motion (which can tear repairs) against prolonged immobilization (which guarantees arthrofibrosis).
Phase II involves the restoration of normal joint kinematics and neuromuscular control. Arthroscopy inherently disrupts the sensory nerve endings within the joint capsule, leading to altered proprioception. Physical therapy must focus on closed-kinetic-chain exercises to stimulate mechanoreceptors and restore dynamic joint stability. The surgeon must closely monitor the patient's progress during this phase; a failure to regain expected range of motion may herald the onset of adhesive capsulitis or arthrofibrosis, necessitating early intervention with oral corticosteroids, aggressive manipulation under anesthesia, or arthroscopic lysis of adhesions.
Phase III centers on the return to pre-injury activity levels, sports, or heavy labor, alongside long-term surveillance for delayed complications. Criteria for return to play must be objective, relying on functional testing, isokinetic strength parity (typically >90% of the contralateral limb), and psychological readiness. The surgeon must also remain vigilant for late-onset complications, such as deep indolent infections (e.g., Cutibacterium acnes in shoulder arthroscopy), hardware failure (such as bioabsorbable anchor osteolysis or migration), and the insidious development of chondrolysis. Regular clinical follow-up and appropriate radiographic surveillance ensure that the orthopedic surgeon can maintain the high success rates and minimal morbidity that modern arthroscopy promises.
Summary of Landmark Literature and Clinical Guidelines
The foundation of our understanding of arthroscopic complications is built upon the landmark literature published over the last several decades. In 1986, Small published his seminal retrospective report, detailing 229 nerve injuries across a massive cohort of knee arthroscopies. Specifically, 30 saphenous nerve injuries and six peroneal nerve injuries were reported in 3,034 meniscal repairs. This study was a wake-up call to the orthopedic community, highlighting that the peroneal nerve is particularly vulnerable during inside-out lateral meniscal repairs if the posterior retractor is not positioned correctly anterior to the lateral head of the gastrocnemius. Small’s subsequent 1988 series demonstrated how rapidly the field adapted; with the implementation of formal posteromedial and posterolateral safety incisions, the incidence dropped to a single saphenous nerve injury in 310 meniscal repairs.
Similarly, in shoulder arthroscopy, the literature reflects a distinct evolutionary curve in complication management. Small’s 1986 data reported one axillary nerve injury and three brachial plexus injuries in 14,329 shoulder arthroscopies. By 1988, reflecting improved positioning protocols, precise traction weight limitations, and heightened awareness of the axillary nerve "safe zone," there were zero nerve injuries reported in 1,184 shoulder procedures. Modern systematic reviews, such as those by Salzler et al., utilizing comprehensive databases like the American Board of Orthopaedic Surgery (ABOS) Part II certification data, have confirmed that while overall complication rates remain low (around 4.6% for shoulder arthroscopy), the nature of complications has shifted toward issues related to complex reconstructions, such as anchor pullout, stiffness, and delayed infection.
Clinical guidelines established by major orthopedic governing bodies provide the medico-legal and clinical framework for safe practice. The American Academy of Orthopaedic Surgeons (AAOS) and the Joint Commission's Universal Protocol are non-negotiable standards for the prevention of wrong-site surgery. Furthermore, guidelines regarding fluid management emphasize the critical need to monitor pump pressures and limit operative times to prevent extravasation and compartment syndrome. The established parameter dictating that emergent fasciotomy is indicated when compartment pressures remain within 30 mm Hg of the patient's diastolic blood pressure (Δp ≤ 30 mm Hg) is a universally accepted surgical threshold derived from extensive traumatology and arthroscopy literature.
Looking forward, the future of complication prevention lies in the integration of advanced technologies and rigorous simulation training. Preoperative 3D modeling and patient-specific templating allow surgeons to anticipate anomalous anatomy before the first incision is made. High-fidelity virtual reality simulators are becoming a mandatory component of orthopedic residency programs, ensuring that the steep learning curve of arthroscopic triangulation and instrument navigation occurs in a risk-free environment rather than on the patient. By adhering to the historical lessons of landmark literature, strictly following established clinical guidelines, and embracing the technological advancements of the future, the orthopedic surgeon can ensure that arthroscopy remains a profoundly safe and highly effective intervention.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons in surgical preparation and board reviews (AAOS, FRCS, Arab Board).
---