Open Reduction and Internal Fixation of Fractures of the Lateral Process of the Talus
Key Takeaway
Open reduction and internal fixation (ORIF) of lateral process talus fractures is indicated for displaced, comminuted, or intra-articular injuries. Often termed "snowboarder's fractures," these injuries require meticulous exposure via a sinus tarsi approach. Anatomical reduction of the subtalar joint and rigid fixation using countersunk or headless compression screws are paramount to preventing post-traumatic subtalar arthritis and ensuring optimal functional recovery in active patients.
INTRODUCTION AND EPIDEMIOLOGY
Fractures of the talus are complex injuries that demand precise anatomical understanding and meticulous surgical execution. While fractures of the talar neck and body are widely discussed, fractures involving the lateral or posterior process of the talus present unique diagnostic and therapeutic challenges. Lateral process fractures, in particular, have seen a dramatic increase in incidence over the last three decades, directly correlating with the rising popularity of snowboarding.
Historically considered rare, lateral process fractures are now specifically associated with ankle injuries incurred while snowboarding, earning the moniker "snowboarder's fracture." Due to their clinical presentation—which closely mimics a severe lateral ankle sprain (specifically involving the anterior talofibular ligament)—these fractures are notoriously elusive. Literature indicates that lateral process fractures are initially missed in up to 50% of patients presenting to emergency departments. Failure to diagnose and appropriately treat these injuries can lead to devastating long-term consequences, including severe subtalar osteoarthritis, chronic lateral column pain, and profound functional disability.
SURGICAL ANATOMY AND BIOMECHANICS
The lateral process of the talus is a prominent, wedge-shaped osseous structure projecting from the lateral aspect of the talar body. It serves a critical biomechanical role, acting as the apex of the lateral column of the ankle and subtalar joints.
The lateral process has two primary articular facets:
1. Dorsolateral Articulation: Articulates with the distal fibula (lateral malleolus).
2. Inferomedial Articulation: Forms the anterolateral portion of the posterior facet of the subtalar joint, articulating with the calcaneus.
Furthermore, the lateral process serves as the primary attachment site for the lateral talocalcaneal ligament and the bifurcate ligament, making it a critical stabilizer of the subtalar joint.
Mechanism of Injury
The classic mechanism of injury for a lateral process fracture involves a combination of axial loading, dorsiflexion, and inversion or eversion of the ankle. In snowboarders, the use of soft boots allows for significant ankle mobility. When a snowboarder lands a jump, the foot is often forced into acute dorsiflexion and inversion. This drives the lateral process of the talus directly into the crucial angle of Gissane on the calcaneus, creating a massive shear force that fractures the process.





Figure: Biomechanical vectors demonstrating neutral, eversion, and inversion forces contributing to lateral and posterior process talar fractures.
CLINICAL EVALUATION AND RADIOGRAPHIC DIAGNOSIS
Patients typically present with acute lateral ankle pain, swelling, and ecchymosis localized just anterior and inferior to the lateral malleolus. Point tenderness over the lateral process is a hallmark sign, though it is easily confused with anterior talofibular ligament (ATFL) pathology.
The "V-Sign" of von Knoch
Standard radiographic evaluation must include weight-bearing anteroposterior (AP), lateral, and mortise views of the ankle. The lateral view is paramount for identifying lateral process fractures. Von Knoch et al. described the "V-sign" as a highly reliable radiographic indicator of a lateral process fracture.
The normal lateral process forms a distinct, symmetrical V-shaped contour on a true lateral radiograph. If this normal V-contour is disrupted, asymmetric, or absent, the sign is considered positive, indicating a fracture.

A: Intact lateral process demonstrating a symmetrical V-shaped contour (negative V-sign).
B: Radiograph of an intact lateral process (negative V-sign).

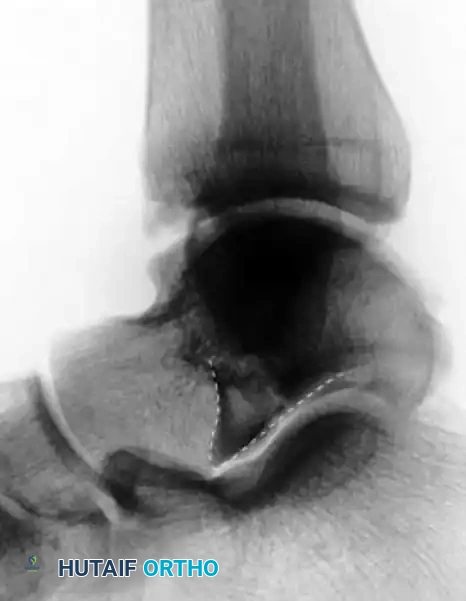
C: Disruption or asymmetry of the V-shape indicates a lateral process fracture (positive V-sign).

D: Radiograph demonstrating a positive V-sign, confirming a lateral process fracture.
💡 Clinical Pearl: Advanced Imaging
While the V-sign is highly specific, plain radiographs often underestimate the degree of comminution and articular displacement. A fine-cut computed tomography (CT) scan (coronal, sagittal, and axial planes) is considered the gold standard and is mandatory for preoperative planning to assess the posterior facet of the subtalar joint.
CLASSIFICATION OF LATERAL PROCESS FRACTURES
The Hawkins classification is the most widely utilized system for categorizing fractures of the lateral process of the talus. It dictates both the prognosis and the surgical approach.
Hawkins Type I: Simple Fracture (42%)
A large, single fracture fragment extending from the talofibular articular surface down to the posterior facet of the subtalar joint. These are highly amenable to Open Reduction and Internal Fixation (ORIF).

Hawkins Type II: Comminuted Fracture (34%)
Involves multiple fragments of the lateral process. These fractures present a significant surgical challenge. Large fragments may be fixed, but severe comminution often necessitates primary excision of the fragments to prevent mechanical block and subtalar arthritis.

Hawkins Type III: Chip Fracture (24%)
An avulsion-type chip fracture of the anterior and inferior aspect of the lateral process. These are typically non-articular and can often be managed non-operatively or with simple excision if they become symptomatic.

INDICATIONS FOR SURGERY
Non-operative management (short-leg cast, non-weight-bearing for 4-6 weeks) is strictly reserved for non-displaced fractures (less than 2 mm of displacement) with no articular step-off.
Absolute Indications for ORIF:
- Displacement greater than 2 mm.
- Any intra-articular step-off in the subtalar or talofibular joint.
- Hawkins Type I fractures of sufficient size to accept a screw.
- Hawkins Type II fractures with reconstructible fragments.
Indications for Primary Excision:
- Severe comminution (Hawkins Type II) where fragments are too small for stable fixation.
- Small, displaced Hawkins Type III chip fractures causing mechanical impingement.
SURGICAL TECHNIQUE: ORIF OF THE LATERAL PROCESS
Preoperative Preparation and Positioning
- Anesthesia: General anesthesia or a regional popliteal block is administered.
- Positioning: The patient is placed in the lateral decubitus position or supine with a large bump under the ipsilateral hip to internally rotate the leg, providing direct access to the lateral ankle.
- Tourniquet: A thigh or calf tourniquet is applied and inflated after exsanguination.
- Fluoroscopy: A C-arm is positioned to allow for unhindered AP, lateral, and mortise views of the ankle and subtalar joint.
Step 1: The Sinus Tarsi Approach
- Approach the lateral process of the talus through a classic sinus tarsi incision.
- Begin the incision at the distal tip of the lateral malleolus (fibula) and extend it obliquely and distally toward the base of the fourth metatarsal.
- Carefully deepen the incision through the subcutaneous tissue.
🚨 Surgical Warning: Nerve Protection
Meticulously identify and protect the communicating branch of the sural nerve and the dorsal intermediate cutaneous branch of the superficial peroneal nerve. These neural structures frequently cross the operative field within the subcutaneous fat. Iatrogenic injury will result in painful neuromas or lateral foot numbness.
Step 2: Deep Dissection and Exposure
- Identify the inferior extensor retinaculum and incise it in line with the skin incision.
- Identify the peroneal tendons (peroneus longus and brevis) within their sheath. Retract the peroneus brevis tendon plantarly to protect it.
- Identify the muscle belly of the extensor digitorum brevis (EDB). Reflect a portion of the EDB origin dorsally and distally. This maneuver opens the sinus tarsi and provides excellent, direct exposure to the lateral process of the talus and the lateral aspect of the posterior subtalar joint.
- Evacuate the fracture hematoma and thoroughly irrigate the joint to remove small osteochondral debris.
Step 3: Fracture Reduction
- Inspect the fracture site. Use a dental pick or a small Freer elevator to mobilize the main fragment.
- Debride any interposed soft tissue or unfixable microscopic bone fragments that block anatomical reduction.
- Reduce the fracture anatomically. The reduction must be verified visually at the articular surface of the posterior facet of the subtalar joint.
- Provisionally hold the reduction using smooth 0.045-inch or 0.062-inch Kirschner wires (K-wires). Ensure the K-wires are placed outside the planned trajectory of the definitive screws.
Step 4: Internal Fixation
- Fix the fracture using standard AO cortical or cancellous screws (typically 2.0 mm, 2.4 mm, or 2.7 mm depending on fragment size).
- Crucial Step: If using standard screws, you must countersink the heads. Prominent screw heads will impinge on the lateral malleolus during ankle dorsiflexion or on the calcaneus during subtalar eversion.
- Alternative (Preferred) Fixation: Utilize full headless compression screws (e.g., Herbert screws [Acumed, Hillsboro, OR] or Acutrak screws [Zimmer, Warsaw, IN]). These screws provide excellent interfragmentary compression while burying the head beneath the articular cartilage or cortical bone, completely eliminating the risk of hardware impingement.
- Confirm anatomical reduction, screw length, and extra-articular hardware placement using multi-planar fluoroscopy.
Step 5: Closure
- Copiously irrigate the wound.
- Allow the EDB muscle belly to fall back into its anatomical position.
- Repair the inferior extensor retinaculum using absorbable sutures (e.g., 2-0 Vicryl).
- Close the subcutaneous tissue and skin in a standard layered fashion.
POSTOPERATIVE CARE AND REHABILITATION
- Immediate Post-Op: Apply a bulky, sterile compression dressing and a short-leg non-walking cast (or rigid posterior splint) in neutral dorsiflexion.
- Weeks 0-3: The patient remains strictly non-weight-bearing. The compression dressing and short-leg non-walking cast are worn for 3 weeks.
- Weeks 3-6: The initial cast is removed. Sutures are removed. A short-leg walking cast or a rigid controlled ankle motion (CAM) boot is applied. The patient may begin progressive weight-bearing as tolerated. Gentle active range of motion (ROM) exercises for the ankle and subtalar joint are initiated out of the boot.
- Weeks 6-12: Transition to regular footwear with an ankle brace. Aggressive physical therapy focuses on subtalar inversion/eversion, peroneal strengthening, and proprioceptive training.
FRACTURES OF THE POSTERIOR PROCESS OF THE TALUS
While lateral process fractures are more common, fractures of the entire posterior process of the talus also occur and require distinct management. The posterior process consists of a medial tubercle and a lateral tubercle, separated by the groove for the flexor hallucis longus (FHL) tendon.
Mechanism of Injury
The probable mechanism of injury for posterior facet/process fractures is severe compression. As described by Dimon, the fragment is sheared off the posterior facet by the corresponding area of the calcaneus as the foot is forced into extreme dorsiflexion and slight external rotation. Alternatively, hyperplantarflexion can cause the posterior process to be crushed between the posterior tibia and the calcaneus (the "nutcracker" mechanism).
Management Strategy
- Non-operative: Posterior process fractures, if small and/or minimally displaced, can be treated non-operatively with cast immobilization.
- Operative (ORIF): Fractures of the entire posterior process are rare but may need ORIF because the fragment often involves a large portion of the articular surface of the subtalar joint. If the fragment is large enough to involve a significant portion of the articular surface and is displaced, surgical fixation through a posterolateral or posteromedial approach is indicated.
- Excision: Late excision of symptomatic non-unions or malunions of the posterior process (or a symptomatic os trigonum) can be highly effective in relieving chronic posterior ankle pain.
SALVAGE PROCEDURES: TIBIOTALAR ARTHRODESIS (BLAIR)
In cases of catastrophic talar body fractures with severe comminution, avascular necrosis (AVN), or when the lateral/posterior processes are entirely non-reconstructible and complicated by talar body collapse, salvage procedures are required. The Blair tibiotalar arthrodesis is a classic technique designed to fuse the tibia to the talar neck while removing the necrotic or destroyed talar body.
Blair Arthrodesis Technique
- Exposure: Expose the ankle through an anterolateral incision.
- Debridement: Remove the comminuted or necrotic fragments of the fractured body of the talus. Crucially, leave the viable head and neck fragments undisturbed to preserve the talonavicular joint.
- Graft Harvesting: Remove a sliding cortical bone graft measuring approximately 2.5 cm wide by 5.0 cm long from the anterior aspect of the distal tibia. Remove the cartilaginous tip from its distal end.
- Preparation of the Talus: Introduce the sliding graft into a previously prepared hole, about 1.8 cm deep, excavated into the dorsal aspect of the neck of the talus.
- Fixation: With the foot held in exactly 10 degrees of plantar flexion (to accommodate normal shoe wear), fix the proximal end of the sliding graft to the tibia with a cortical screw.
- Bone Grafting: Pack cancellous bone chips (harvested from the tibial window or iliac crest) tightly around the distal end of the graft and the talar neck junction.
Postoperative Care for Blair Arthrodesis
- A cast is applied from the groin to the toes with the knee in extension and is worn for 4 to 6 weeks.
- Following this, a short-leg cast is applied. Protected walking is allowed depending on the appearance of trabecular bridging and healing on follow-up radiographs.
- Cast immobilization usually is required for a total of 12 to 16 weeks to ensure solid arthrodesis.
CONCLUSION
Fractures of the lateral process of the talus are significant intra-articular injuries that demand a high index of suspicion, particularly in the snowboarding demographic. Accurate diagnosis relies on identifying the V-sign on lateral radiographs and utilizing CT imaging for surgical planning. Anatomical reduction and rigid internal fixation via a sinus tarsi approach, utilizing countersunk or headless compression screws, provide the most reliable pathway to restoring subtalar joint congruity and preventing long-term post-traumatic arthritis.
You Might Also Like
