What to Expect: Ankle Surgery Postoperative Care & Instructions
Key Takeaway
This topic focuses on What to Expect: Ankle Surgery Postoperative Care & Instructions, Postoperative care and instructions following ankle arthrodesis emphasize patient education regarding altered gait. Patients should expect walking will not return to normal, experiencing reduced speed and increased energy expenditure. Achieving optimal fusion position—0° dorsiflexion, 0°-5° valgus, 5°-10° external rotation—is crucial for recovery, guiding rehabilitation strategies and managing long-term functional expectations.
A 45-year-old active patient presents with end-stage post-traumatic ankle arthritis. They have failed all non-operative measures. You are discussing the choice between ankle arthrodesis and total ankle arthroplasty (TAA). What are the critical biomechanical principles and patient factors you must assess to determine the optimal surgical path?
Candidate: I would evaluate the patient's age and activity level. If they are young and active, arthrodesis is usually safer. I'd look at the x-rays to see the degree of arthritis and deformity. I'd also check their vascular status and make sure they don't have diabetes or smoke, as these affect healing.
Failing to mention coronal plane deformity is a major error. Candidates often provide a generic list of factors without prioritizing the anatomical constraints of TAA (e.g., <15 degrees of deformity) versus the salvage nature of arthrodesis. Missing the distinction between "patient demands" and "biological prerequisites" is a common reason for a failing grade.
I would approach this by assessing three domains: 1. Patient Factors: Age, activity demands, and metabolic profile (HbA1c, smoking status). Arthrodesis is favored for high-impact labor, while TAA is considered for low-demand, older cohorts. 2. Deformity/Alignment: TAA requires a neutral coronal axis; deformity >15° typically mandates arthrodesis or staged correction. 3. Joint Integrity: Assessment of bone stock (CT scan for cysts/AVN) and ligamentous stability. If there is significant AVN of the talus or instability, arthrodesis is the gold standard. I would also note that arthrodesis is the definitive salvage for failed TAA.
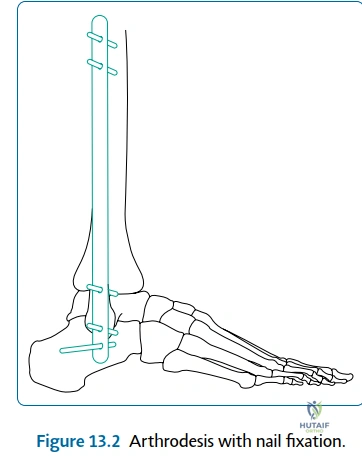
You have decided to perform an ankle arthrodesis. Describe the "Golden Position" for the fusion and explain the consequences of failing to achieve this orientation.
Candidate: The ankle should be fused at 0 degrees, which is neutral. This makes the foot flat on the ground. If you fuse it in too much plantarflexion, the patient will walk on their toes and get knee pain.
Providing an incomplete "Golden Position." Candidates often forget to mention external rotation (5°-10°) to match tibial torsion, which is essential to avoid gait abnormalities. Simply saying "neutral" is insufficient at this level.
The optimal position for ankle arthrodesis is 0° of dorsiflexion/plantarflexion (neutral), 0°-5° of valgus, and 5°-10° of external rotation to match the contralateral limb. Consequences of malposition: - Plantarflexion: Causes a recurvatum thrust at the knee and creates a "vaulting" gait. - Varus: Locks the subtalar and transverse tarsal joints, resulting in a rigid, painful midfoot and accelerated adjacent segment degeneration.
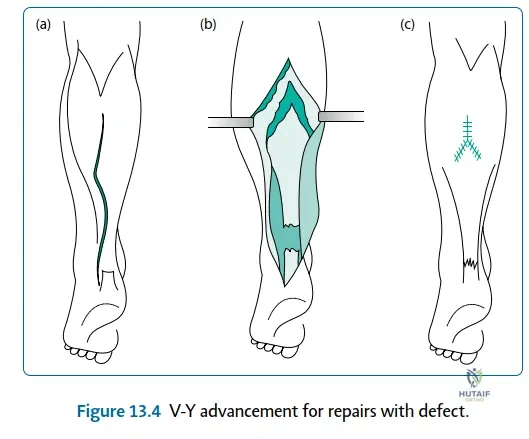
During the postoperative phase of an Achilles tendon repair, what are the specific risks, and how does your rehabilitation protocol mitigate them?
Candidate: The main risk is a wound infection because the skin is thin. I would keep the patient in a cast for 6 weeks and then start moving the ankle. I would also worry about DVT since they are non-weight bearing.
Suggesting strict immobilization for 6 weeks is outdated. Modern evidence-based practice favors early, controlled functional rehabilitation. Failing to address the "sural nerve" risk during surgical approach and the importance of avoiding passive dorsiflexion stretching shows a lack of clinical nuance.
The primary risks are wound dehiscence, sural nerve injury, and tendon elongation due to premature loading. My protocol: 1. Phase 1: Immobilization in 15°-20° of plantarflexion to reduce tension. 2. Phase 2: Transition to a CAM boot with graduated weight-bearing at 2 weeks. 3. Key Principle: Avoid passive dorsiflexion stretching to prevent elongation. Use early functional rehab to encourage controlled stress, which improves collagen alignment while maintaining DVT prophylaxis for the duration of limited mobility.
