Acute Knee Injury Case Study: Collegiate Athlete with ACL Rupture & Multiligamentous Damage
Key Takeaway
Diagnosing a complex ACL rupture, as seen in collegiate athletes, involves detailed clinical examination including Lachman and Pivot Shift tests, often revealing associated MCL sprains and meniscal tears. Imaging, particularly MRI, confirms complete ACL disruption, bone contusions, and specific findings like a Segond fracture or bucket-handle meniscal tears, guiding comprehensive treatment.
A 22-year-old male soccer player presents with acute knee pain and hemarthrosis following a non-contact pivot injury. You suspect an ACL tear. Describe the clinical examination sequence you would perform to confirm this diagnosis and rule out common associated injuries, and mention the specific radiographic finding that would increase your index of suspicion for a rotatory component.
Candidate: I would examine the knee for an effusion, which is likely a hemarthrosis. I would perform the Lachman test, which is the most sensitive, followed by the Pivot Shift to test for rotatory instability. I would check the collateral ligaments (valgus/varus) to rule out an unhappy triad, and the PCL. Radiographically, I would specifically look for a Segond fracture, which is an avulsion of the anterolateral capsule.
Failing to mention the "order" of examination. Candidates often forget to mention performing tests in a way that minimizes pain (e.g., checking the PCL first to confirm the tibia isn't sagged, which gives a false negative Lachman). Also, failing to quantify findings (e.g., "Grade I vs Grade III laxity") or missing the clinical importance of the Segond fracture as a marker for the anterolateral ligament (ALL) complex injury.
A structured response: 1. Inspection/Palpation: Note the hemarthrosis (positive predictive value 70-90% for intra-articular injury). 2. Stability Testing: PCL first (Posterior Drawer/Sag) to ensure the tibia is not starting from a posterior position. Then the Lachman (most sensitive, 20-30 deg flexion). Followed by the Pivot Shift (best for rotatory instability/functional outcome). 3. Collateral/Meniscal: Valgus/Varus testing at 0 and 30 degrees, McMurray/joint line tenderness. 4. Imaging: A Segond fracture (lateral capsular sign) is the avulsion of the ALL at the tibia, indicating significant rotational instability. Mentioning the need to "pre-hab" to restore terminal extension before definitive surgery is a critical high-level addition.
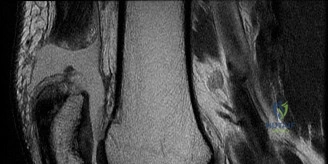
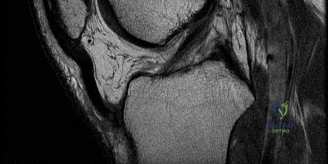
The MRI confirms a complete mid-substance ACL tear with an associated longitudinal vertical tear of the posterior horn of the medial meniscus. The patient is a professional soccer player. Explain your rationale for surgical decision-making and how the imaging findings influence your graft choice.
Candidate: Given his high activity level (Division I soccer), non-operative management carries a high risk of secondary meniscus or chondral damage. I would reconstruct the ACL because the meniscal repair requires a stable knee for the graft to heal. I would use a Bone-Patellar Tendon-Bone (BTB) autograft because it provides bone-to-bone healing, which is faster and more robust for elite athletes than allograft or hamstring autografts.
Suggesting allograft to "save" the harvest site or failing to mention the relationship between the meniscus and the ACL. A failing candidate might also ignore the timing, suggesting surgery "now" while the knee is still swollen, which significantly increases the risk of postoperative arthrofibrosis.
Structure the answer around: 1. Synergy: The posterior horn of the medial meniscus is a secondary restraint; repairing it requires a stable knee (ACL reconstruction), and the reconstruction is protected by the repair. 2. Graft Selection: BTB autograft is the gold standard for high-demand athletes due to the rigid bone-to-bone fixation, allowing faster incorporation. Specifically address why allograft is contraindicated (higher failure rates in <25s due to structural changes from sterilization). 3. Pre-habilitation: Emphasize the necessity of achieving full extension and settling the effusion (typically 4-6 weeks) to prevent arthrofibrosis, a common mistake in early-career surgeons.
During the arthroscopic procedure, you observe the intercondylar notch and perform the meniscal repair. How do you ensure correct tunnel placement to avoid graft impingement and optimize biomechanical outcomes?
Candidate: I would debride the notch to find the anatomical footprint, specifically the lateral bifurcate ridge and the lateral intercondylar ridge, also known as the resident's ridge. I would use an accessory anteromedial portal to drill the femoral tunnel to ensure it is anatomic rather than high in the notch. For the tibia, I would place the guide in the center of the footprint, posterior to the anterior horn of the lateral meniscus.
Mentioning "isometric placement" as the goal—this is an older, outdated concept. Modern FRCS examiners look for "Anatomic Footprint Reconstruction." Failing to identify the "resident's ridge" (the critical bony landmark) shows a lack of anatomical mastery required at the Senior Registrar level.
Focus on Anatomical Reconstruction: 1. Landmarks: Identify the lateral bifurcate ridge (separates AM and PL bundles) and the lateral intercondylar ridge (resident's ridge, the superior boundary of the footprint). 2. Technique: Use an accessory AM portal for independent femoral tunnel placement, which avoids the "vertical" tunnel placement often seen with a transtibial approach. 3. Meniscal Repair: Note the transition from "inside-out" to modern "all-inside" suture devices, and the importance of rasping the tear to stimulate a biological healing response.
