Open Reduction for Old Unreduced Knee Dislocation

Key Takeaway
Old unreduced dislocations of the knee and patella present complex reconstructive challenges due to adaptive soft-tissue contractures and articular degeneration. Successful management requires distinguishing traumatic from congenital etiologies. Treatment ranges from benign neglect in functional patients to complex open reduction, realignment, or salvage procedures like arthrodesis and arthroplasty. This guide details the biomechanics, surgical approaches, and postoperative protocols necessary to optimize outcomes in these rare, high-morbidity orthopedic presentations.
INTRODUCTION TO CHRONIC UNREDUCED DISLOCATIONS OF THE KNEE
Old unreduced dislocations of the knee—encompassing both the tibiofemoral joint and the patellofemoral articulation—are exceedingly rare in modern orthopedic practice due to advancements in acute trauma imaging and management. However, when encountered, they present a formidable reconstructive challenge. The chronicity of the dislocation leads to profound adaptive changes, including severe soft-tissue contractures, capsular scarring, articular cartilage degeneration, and adaptive bony remodeling.
Management of these complex lesions requires a highly individualized approach. The surgeon must carefully weigh the functional demands of the patient against the extensive surgical dissection required for open reduction. In many cases, the native joint cannot be salvaged, necessitating complex reconstructive options such as arthrodesis, constrained arthroplasty, or realignment osteotomies.
PATHOPHYSIOLOGY AND BIOMECHANICS
Distinguishing Traumatic from Congenital Patellar Dislocation
A critical diagnostic step in evaluating an old unreduced dislocation of the patella is distinguishing a missed traumatic event from a congenital dislocation. This distinction fundamentally alters the surgical approach and prognosis.
Congenital dislocation of the patella is often not appreciated during infancy because normal patellar ossification does not occur until approximately 3 years of age. The congenital lesion is characterized by primary anatomical abnormalities:
* Primary Incongruity: The patella and the femoral trochlea are dysplastic from birth.
* Obligatory Contractures: A severe flexion contracture of the knee is a primary component of the original pathological process, driven by the abnormal vector of the extensor mechanism.
In contrast, posttraumatic chronic dislocations exhibit secondary, adaptive changes:
* Adaptive Flattening: The patella undergoes adaptive flattening over time due to abnormal tracking and loss of normal articulation with the trochlear groove.
* Reactive Contractures: The knee flexion contracture is a reactive change secondary to capsular scarring, intra-articular fibrosis, and hamstring shortening, rather than a primary developmental anomaly.
Clinical Pearl: A high percentage of traumatic patellar dislocations (up to 16%) are missed in the acute setting when an associated tibiofemoral knee dislocation is present. Always maintain a high index of suspicion for concomitant patellar dislocation when the medial stabilizing structures (medial patellofemoral ligament, medial collateral ligament) have been severely damaged.
PREOPERATIVE EVALUATION
Clinical Assessment
Patients with chronic unreduced dislocations typically present with profound mechanical symptoms, including an inability to bear weight, severe limitation in range of motion (ROM), and fixed flexion or valgus/varus deformities. However, a subset of patients may present with surprisingly functional, albeit mechanically altered, ambulation.
A meticulous neurovascular examination is mandatory. The popliteal artery and common peroneal nerve are at high risk during the initial traumatic event and remain at risk during any surgical attempt to mobilize and reduce the chronically contracted joint.
Imaging Protocols
Standard orthogonal radiographs (Anteroposterior and Lateral) are the baseline requirement. They will demonstrate the direction of the dislocation (anterior, posterior, medial, or lateral) and the degree of adaptive bony changes, osteopenia, and post-traumatic arthritis.
Advanced imaging, including Computed Tomography (CT) with 3D reconstruction, is invaluable for assessing bone stock, trochlear dysplasia, and the exact spatial relationship of the dislocated segments. Magnetic Resonance Imaging (MRI) is utilized to evaluate the integrity of the extensor mechanism, the degree of meniscal and cruciate ligament obliteration, and the presence of intra-articular fibrosis. CT Angiography (CTA) should be strongly considered if there is any alteration in distal pulses or if extensive posterior dissection is anticipated.
INDICATIONS FOR SURGICAL INTERVENTION
The treatment algorithm for old traumatic dislocations is dictated by the duration of the dislocation, the degree of articular degeneration, and the patient's baseline function.
1. Observation (Benign Neglect)
Function of the knee can sometimes be surprisingly satisfactory despite an old unreduced dislocation of the patella or even a chronic subluxation of the tibiofemoral joint. If the patient is ambulatory with minimal pain and acceptable alignment, observation is the treatment of choice. The risks of extensive surgical dissection often outweigh the benefits in a highly adapted, painless limb.
2. Open Reduction and Realignment
Open reduction is indicated if:
* The dislocation is of relatively short duration (weeks to a few months).
* Degenerative changes of the patella and tibiofemoral joint are minimal or absent.
* The patient has severe functional impairment that can be mechanically corrected.
3. Salvage Procedures (Patellectomy, Arthrodesis, Arthroplasty)
In dislocations of long duration, traumatic arthritis is inevitably present. Joint motion will be severely limited, accompanied by debilitating pain.
* Patellar Degeneration: If patellar degenerative changes are significant, a patellaplasty or complete patellectomy may be indicated. There is currently insufficient evidence to support the use of isolated patellar resurfacing or patellar prostheses for this specific chronic condition.
* Tibiofemoral Degeneration: If open reduction of the knee would require excessive dissection that compromises the neurovascular bundle or soft-tissue envelope, salvage with an arthrodesis or total knee arthroplasty (TKA) is required.
Surgical Warning: The long-term prognosis for useful, pain-free function is guarded regardless of the procedure selected. Extensive preoperative counseling regarding the potential need for future fusion or arthroplasty is mandatory.
SURGICAL TECHNIQUE: OPEN REDUCTION OF THE KNEE
Positioning and Anesthesia
The patient is placed supine on a radiolucent operating table. General or regional anesthesia is administered. A high thigh tourniquet is applied but not inflated unless necessary, to allow for continuous assessment of distal perfusion during the reduction maneuvers. The contralateral limb is prepped and draped if autograft harvesting is anticipated.
Surgical Approach
- Incision: A standard anterior midline incision is preferred, allowing extensile access to both the medial and lateral compartments, as well as the extensor mechanism.
- Arthrotomy: A medial parapatellar arthrotomy is typically utilized. In cases of severe lateral patellar dislocation with lateral retinacular contracture, a lateral release is performed simultaneously to mobilize the extensor mechanism.
- Debridement and Mobilization: The joint space is often obliterated by dense fibrous tissue. Meticulous excision of the scar tissue within the intercondylar notch, the medial and lateral gutters, and the suprapatellar pouch is required.
- Neurovascular Protection: If posterior subluxation is present, the posterior capsule will be heavily scarred to the posterior femoral condyles. Extreme caution must be exercised when elevating the posterior capsule to avoid injury to the popliteal artery, which may be tethered by scar tissue.
Reduction and Temporary Fixation
Once the soft tissues are adequately mobilized, gentle traction and manipulation are applied to reduce the tibiofemoral joint. Forceful leverage must be avoided to prevent iatrogenic fractures of the osteopenic bone.
If the joint is highly unstable following reduction due to the complete incompetence of the collateral and cruciate ligaments, temporary transarticular fixation is required. A smooth, heavy Steinmann pin is driven through the quadriceps mechanism, across the femur, and into the tibia to hold the reduction in approximately 10 to 15 degrees of flexion.
CLINICAL CASE EXAMPLE: CHRONIC DISLOCATION IN NEUROFIBROMATOSIS
The following case illustrates the complexity of managing a chronic, unreduced dislocation. The patient is a 17-year-old girl with a history of neurofibromatosis who presented with a 6-week history of an acute knee dislocation and a complete inability to walk.
Preoperative Imaging
Initial radiographs demonstrated a severe posteromedial dislocation of the tibia relative to the femur, accompanied by a medial dislocation of the patella.
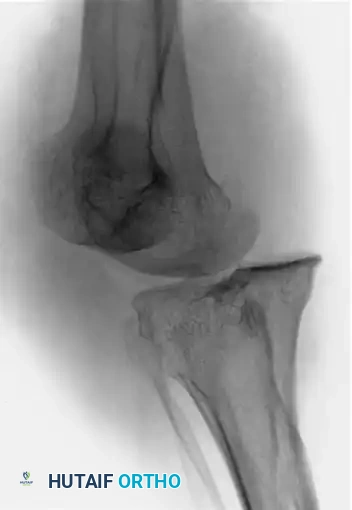
Figures A and B: Anteroposterior and lateral radiographs of the knee showing a posteromedial knee dislocation with medial dislocation of the patella.
Intraoperative Management
Given the 6-week duration, an open reduction was mandated. Extensive soft-tissue releases were performed to mobilize the contracted structures. Following successful reduction of both the tibiofemoral and patellofemoral joints, the inherent instability required temporary internal fixation. A smooth Steinmann pin was passed longitudinally through the quadriceps mechanism, traversing the femur and anchoring into the tibia to maintain alignment.
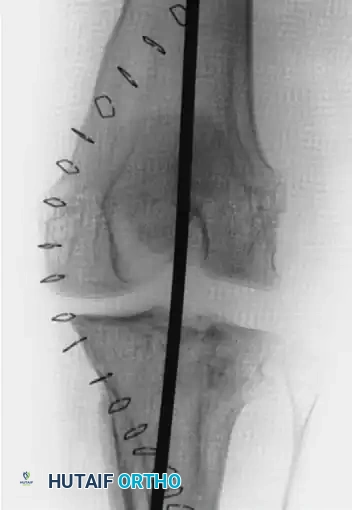

Figures C and D: Anteroposterior and lateral radiographs at the time of open reduction and internal fixation with a smooth Steinmann pin through the quadriceps mechanism of the femur and tibia.
Postoperative Outcomes
Postoperative imaging confirmed the restoration of the mechanical axis. While a mild persistent lateral subluxation of the patella remained, the overall reduction of the knee and patellar dislocations was highly satisfactory, allowing the soft tissues to heal in an anatomically appropriate position.


Figures E and F: Postoperative anteroposterior and lateral radiographs showing mild persistent lateral subluxation but good overall reduction of the knee and patellar dislocations.
SALVAGE PROCEDURES FOR THE UNREDUCIBLE KNEE
When open reduction alone requires excessive dissection that threatens limb viability, or when the articular cartilage is completely destroyed, salvage procedures must be employed.
1. Arthrodesis
Knee arthrodesis remains a highly reliable salvage option for the chronically dislocated, painful, and unstable knee, particularly in young laborers or patients with compromised extensor mechanisms.
* Technique: The remaining articular cartilage and fibrotic tissue are resected to healthy, bleeding cancellous bone. The knee is positioned in 10 to 15 degrees of flexion and 5 to 7 degrees of valgus.
* Fixation: Intramedullary nailing is the biomechanically superior choice, though dual-plate constructs or external fixation may be required if active infection or severe bone loss is present.
2. Total Knee Arthroplasty (TKA)
In older, lower-demand patients, TKA can provide a mobile, painless joint. However, the surgeon must be prepared for severe bone loss and complete ligamentous incompetence.
* Implants: A rotating-hinge or fully constrained prosthesis is almost universally required due to the absence of functional collateral ligaments.
* Soft Tissue Balancing: Extensive releases are required. If the extensor mechanism is contracted, a quadriceps snip, V-Y quadricepsplasty, or tibial tubercle osteotomy may be necessary to gain exposure and allow for subsequent closure.
3. Realignment Osteotomy (The Assighir Technique)
In highly selected cases where the knee is chronically dislocated but remains functional and painless, attempting a direct intra-articular reduction may cause more harm than good. Assighir reported successfully treating a chronic dislocation by performing a realignment distal femoral osteotomy above the dislocated joint.
* Biomechanics: This extra-articular procedure realigns the mechanical axis of the lower extremity, improving gait mechanics and reducing abnormal stress on the adjacent joints, while leaving the adapted, functional pseudarthrosis of the knee undisturbed.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol is entirely dependent on the surgical intervention performed.
Following Open Reduction and Pinning
- Immobilization: The extremity is immobilized in a long-leg cast or a rigid hinged knee brace locked in extension (or slight flexion, depending on the pinning angle).
- Pin Management: If a transarticular Steinmann pin is used, it is typically left in place for 4 to 6 weeks to allow the capsular structures to heal and the contractures to resolve.
- Weight-Bearing: The patient is kept strictly non-weight-bearing on the operative extremity.
- Rehabilitation: Once the pin is removed, aggressive physical therapy is initiated to restore range of motion. The transition to weight-bearing is gradual, protected by a hinged brace. If the joint remains stiff, a manipulation under anesthesia (MUA) or subsequent arthroscopic lysis of adhesions may be required.
Following Arthroplasty or Arthrodesis
- Arthroplasty: Postoperative care mirrors that of a complex revision TKA. Early mobilization is encouraged to prevent arthrofibrosis, though the use of a hinged brace may be necessary to protect the soft-tissue envelope.
- Arthrodesis: The limb is protected until radiographic evidence of bony union is observed, typically requiring 12 to 16 weeks. Progressive weight-bearing is allowed based on the stability of the fixation construct.
COMPLICATIONS
The surgical management of old unreduced knee dislocations is fraught with potential complications:
* Neurovascular Injury: The highest-risk complication. Traction injuries to the peroneal nerve or tethering of the popliteal artery during reduction can lead to catastrophic limb loss.
* Arthrofibrosis: Severe stiffness is common due to the extensive surgical dissection and the preexisting fibrotic state of the joint.
* Recurrent Dislocation/Subluxation: Due to the attenuation of the native ligaments, the joint may slowly subluxate postoperatively, as seen in the clinical case example.
* Post-Traumatic Osteoarthritis: Even with a perfect anatomical reduction, the prolonged period of abnormal joint loading inevitably leads to accelerated chondral wear, often necessitating future arthroplasty.
CONCLUSION
Old unreduced dislocations of the knee and patella are complex pathologies that demand meticulous preoperative planning and a deep understanding of altered joint biomechanics. While observation is appropriate for the highly adapted, functional patient, surgical intervention is often required for those with severe pain and disability. Whether utilizing open reduction with temporary transarticular fixation or employing salvage techniques like arthrodesis and constrained arthroplasty, the orthopedic surgeon must carefully balance the desire for anatomical restoration against the risks of extensive soft-tissue dissection.
You Might Also Like

