Derotational High Tibial Osteotomy for Patellofemoral Instability: A Comprehensive Surgical Guide
Key Takeaway
Derotational high tibial osteotomy is a powerful joint-preserving procedure indicated for skeletally mature patients presenting with patellofemoral instability and severe rotational deformity. By addressing excessive external tibial torsion—typically defined by a thigh-foot angle exceeding 30 degrees—this technique normalizes patellofemoral kinematics. This guide details the biomechanical rationale, precise surgical steps of the Paulos technique, and postoperative rehabilitation protocols essential for optimizing functional outcomes and minimizing complications.
Introduction to Derotational High Tibial Osteotomy
Patellofemoral instability is a complex, multifactorial pathology that demands a comprehensive understanding of lower extremity alignment, both in the coronal and axial planes. While soft tissue reconstructions (such as medial patellofemoral ligament reconstruction) are sufficient for many patients, those with severe underlying osseous malalignment require bony correction to achieve durable stability. For skeletally mature patients with instability associated with severe rotational deformity—often a component of "miserable malalignment syndrome"—a derotational high tibial osteotomy (HTO) combined with tibial tubercle transfer has been found to produce vastly superior functional results and more normal gait patterns than isolated proximal or distal soft-tissue realignment procedures.
The primary goal of this procedure is to normalize the extensor mechanism vector by correcting excessive external tibial torsion, thereby centralizing the patella within the trochlear groove and reducing lateral patellofemoral contact pressures.
Biomechanics and Pathoanatomy
To appreciate the necessity of a derotational osteotomy, the surgeon must understand the biomechanical interplay of the lower limb's rotational profile. Excessive external tibial torsion laterally displaces the tibial tubercle relative to the femoral trochlea. This lateralization dramatically increases the Q-angle, creating a pathologic laterally directed force vector on the patella during quadriceps contraction.
When the tibia is externally rotated, the patella is forced to track against the lateral trochlear facet. Over time, this leads to lateral retinacular tightness, medial soft tissue attenuation, and eventual patellofemoral chondrosis or recurrent dislocation.
Clinical Pearl: Soft tissue procedures alone in the presence of severe external tibial torsion are doomed to fail. The reconstructed medial patellofemoral ligament (MPFL) will inevitably stretch out if the underlying bony vector is not corrected.
By performing a derotational osteotomy and transferring the tibial tubercle, the surgeon effectively medializes the extensor mechanism. Furthermore, by anteriorizing the tubercle during the transfer, joint reaction forces across the patellofemoral joint are significantly decompressed, protecting the articular cartilage.
Clinical Evaluation and Indications
Thorough preoperative clinical and radiographic evaluation is paramount. The rotational profile of the lower extremity must be assessed meticulously.
Physical Examination
- Thigh-Foot Angle (TFA): Measured with the patient prone and the knees flexed to 90 degrees. A TFA of more than 30 degrees of external rotation is highly suggestive of pathologic tibial torsion.
- Tubercle-Sulcus Angle (TSA): Measured with the knee flexed 90 degrees and hanging off the examination table. A TSA of more than 10 degrees indicates significant lateralization of the tibial tubercle.
- Patellar Glide and Tilt: Assess for lateral retinacular tightness (negative passive patellar tilt) and medial soft tissue laxity.
Imaging Studies
- Plain Radiographs: Weight-bearing anteroposterior (AP), lateral, and axial (Merchant or Skyline) views to assess baseline osteoarthritis, patellar height (Caton-Deschamps index), and trochlear dysplasia.
- Computed Tomography (CT): A CT rotational profile (hip, knee, and ankle) is the gold standard for quantifying femoral anteversion and tibial torsion.
- Magnetic Resonance Imaging (MRI): Essential for evaluating the integrity of the articular cartilage, menisci, and ligamentous structures.
Strict Surgical Indications
Suggested indications for a derotational high tibial osteotomy include:
* Skeletal maturity (closed physes).
* Recurrent patellofemoral instability refractory to conservative management.
* Thigh-foot angle (TFA) > 30 degrees.
* Tubercle-sulcus angle (TSA) > 10 degrees (measured at 90 degrees of knee flexion).
* Absence of advanced, diffuse patellofemoral or tibiofemoral osteoarthritis (though isolated lateral or distal patellar chondrosis may benefit from the anteriorization component).
Surgical Technique: The Paulos et al. Approach
The following technique, adapted from Paulos et al., describes a comprehensive approach to derotational high tibial osteotomy focusing on tibial tubercle transfer, lateral release, and medial plication.
1. Patient Positioning and Anesthesia
The patient is placed supine on the operating table. A well-padded high thigh tourniquet is applied. The operative leg is prepped and draped free to allow full range of motion (ROM) from 0 to 120 degrees of flexion. A lateral post or leg holder may be used, but the ability to freely assess patellar tracking throughout the procedure is critical.
2. Diagnostic Arthroscopy
Before proceeding with the open osteotomy, a complete anterior and posterior diagnostic arthroscopy is mandatory.
* Systematically evaluate the suprapatellar pouch, patellofemoral joint, medial and lateral gutters, and both tibiofemoral compartments.
* Assess the severity and location of any chondral defects.
* Treat any identified intraarticular pathological processes (e.g., loose body removal, meniscal debridement, or chondroplasty) as required.
3. Lateral Retinacular Release
If a negative passive patellar tilt was present during the preoperative examination (indicating a tight lateral retinaculum), a lateral release is performed.
* Incision: This can be done arthroscopically or through the planned open incision.
* Execution: Incise the lateral retinaculum and synovium starting from the tibial tubercle and extending proximally.
* Critical Boundary: The release must extend up to, but not include, the vastus lateralis muscle. Preserving the vastus lateralis tendon is crucial to maintain dynamic superior-lateral stability and prevent iatrogenic medial patellar subluxation.
Surgical Warning: Over-release of the lateral structures, particularly violating the vastus lateralis obliquus, is a primary cause of iatrogenic medial patellar instability. Ensure the release is strictly limited to the retinaculum.
4. The Osteotomy and Tubercle Transfer
The core of the procedure involves the osteotomy and subsequent realignment of the tibial tubercle.
* Exposure: Make a longitudinal incision just lateral to the anterior tibial crest, extending from the distal pole of the patella to approximately 10 cm distal to the tibial tubercle. Elevate full-thickness flaps.
* Osteotomy Cut: Using an oscillating saw, perform a flat or slightly oblique osteotomy of the tibial tubercle. The length of the shingle should be at least 6 to 8 cm to allow for adequate bone-to-bone healing and to prevent a stress riser.
* Derotation and Anteriorization: The goal is to correct the tubercle-sulcus angle to between 10 and 15 degrees. Biomechanically, this usually requires moving the tuberosity anteriorly 8 to 10 mm, alongside the medializing/derotational shift.
* Bone Grafting (If necessary): Depending on the angle of the cut (e.g., a Fulkerson-style anteromedialization), a local autograft wedge from the proximal tibia may be used to support the anteriorized tubercle.
5. Provisional Fixation and Tracking Assessment
Safety and precision during fixation are paramount.
* Positioning for Drilling: Flex the knee to exactly 90 degrees.
* Provisional Pinning: Secure the transferred tuberosity by placing a drill bit or Kirschner wire proximally through the tuberosity and into the posterior tibial cortex.
Surgical Warning: Drilling must be performed with the knee in 90 degrees of flexion. In this position, the popliteal artery and tibial nerve fall posteriorly, significantly decreasing the risk of catastrophic neurovascular injury from over-penetration of the drill bit or screws.
- Dynamic Assessment: Release the tourniquet (optional, to assess bleeding) and move the knee through a full range of motion. Carefully evaluate patellar tracking. The patella should engage the trochlea smoothly without lateral subluxation or excessive medial pressure. If tracking is not optimal, remove the provisional wire, adjust the tubercle position, and reassess.
6. Definitive Fixation
Once satisfactory tracking is confirmed, proceed with definitive fixation.
* Secure the tuberosity with two countersunk, low-profile, cancellous screws (typically 4.5 mm or 3.5 mm, depending on patient size).
* Utilize a lag technique to ensure robust compression across the osteotomy site.
* Countersinking is critical; prominent hardware over the anterior tibia is a leading cause of postoperative pain and subsequent reoperation for hardware removal.
7. Medial Retinacular Plication and Closure
To reinforce the medial restraints and balance the soft tissue envelope:
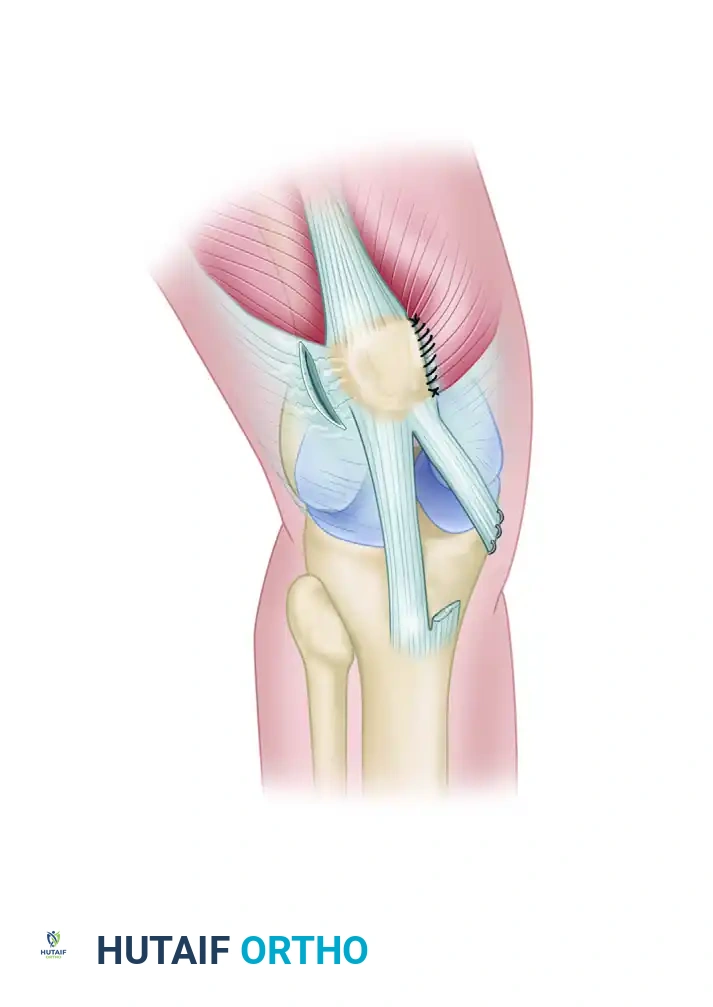
* Medial Plication: Close the medial retinaculum in a "pants-over-vest" fashion. This plicates the medial side, effectively advancing the vastus medialis obliquus (VMO) and tightening the attenuated medial structures.
* Lateral Management: Do not close the lateral retinaculum. Leave it open to prevent recurrence of lateral tethering.
* Skin Closure: Close the subcutaneous tissues and skin in a standard layered fashion. A closed suction drain may be placed deep to the subcutaneous tissue if significant oozing is anticipated.
Postoperative Care and Rehabilitation Protocol
The postoperative protocol must balance the need for early motion to prevent arthrofibrosis with the necessity of protecting the osteotomy site until bony union occurs.
Phase 1: Immediate Postoperative (Weeks 0 to 4)
- Weight Bearing: Weight bearing is allowed as tolerated (WBAT) immediately after surgery, provided the knee is locked in full extension in a hinged knee brace. Axial loading in extension compresses the osteotomy site and promotes healing.
- Immobilization: The knee is immobilized in full extension for ambulation.
- Range of Motion: Passive and active-assisted ROM exercises (0 to 90 degrees) are initiated early, typically within the first week, but only when non-weight bearing.
Phase 2: Intermediate Rehabilitation (Weeks 4 to 8)
- Immobilization: Immobilization is generally continued for 4 to 6 weeks. At the 6-week mark, clinical and radiographic evaluation is performed to assess early callus formation.
- Progression: If radiographs demonstrate satisfactory healing, the brace is gradually weaned.
- Strengthening: Range-of-motion and progressive strengthening exercises are formally instituted. Focus is placed on closed-kinetic-chain exercises, VMO recruitment, and core/gluteal strengthening to control femoral internal rotation.
Phase 3: Advanced Rehabilitation and Return to Play (Months 3 to 9)
- Advanced Strengthening: Isotonic and isokinetic strengthening continues. Proprioceptive and agility training are introduced.
- Return to Sports: Return to high-impact or pivoting sports is usually allowed at 6 to 9 months after surgery, contingent upon radiographic evidence of complete bony union, full painless ROM, and quadriceps strength reaching at least 85-90% of the contralateral limb.
Complications and Pitfalls
While highly effective, derotational high tibial osteotomy and tubercle transfer carry specific risks that the surgeon must anticipate and mitigate.
- Neurovascular Injury: As emphasized, the popliteal vessels are at risk during drilling and screw placement. Strict adherence to drilling at 90 degrees of flexion is mandatory.
- Late Tibial Fracture: There is a recognized long-term risk for proximal tibial fracture after this procedure. The osteotomy creates a stress riser in the anterior tibial cortex. Patients must be counseled regarding this risk, and the surgeon must ensure the distal end of the osteotomy is tapered smoothly to minimize stress concentration.
- Nonunion or Delayed Union: Smoking, poor bone quality, or inadequate fixation can lead to nonunion. Rigid lag screw fixation and early axial loading in extension help mitigate this.
- Symptomatic Hardware: Due to the lack of soft tissue coverage over the anterior tibia, screw heads frequently cause irritation. Meticulous countersinking reduces, but does not eliminate, the potential need for future hardware removal.
- Overcorrection/Undercorrection: Undercorrection leads to recurrent instability, while overcorrection (excessive medialization) can cause iatrogenic medial instability and severe medial compartment arthrosis. Precise preoperative templating and intraoperative dynamic assessment are the best defenses against malalignment.
Conclusion
Derotational high tibial osteotomy with tibial tubercle transfer is a highly demanding but exceptionally rewarding procedure for the treatment of patellofemoral instability in the setting of severe rotational deformity. By addressing the root pathoanatomy—excessive external tibial torsion and lateralization of the extensor mechanism—surgeons can restore normal joint kinematics. Strict adherence to indications, meticulous surgical technique as outlined by Paulos et al., and a structured postoperative rehabilitation program are essential to achieving optimal, long-lasting functional outcomes while minimizing the risk of complications.
You Might Also Like