Popliteal Sciatic Nerve Block: Comprehensive Surgical Technique
Key Takeaway
The popliteal sciatic nerve block is a highly effective regional anesthesia technique for foot and ankle surgery. Performed in the prone or lateral position, it targets the sciatic nerve proximal to its bifurcation. This guide details the anatomical landmarks, nerve stimulation parameters, and ultrasound-guided techniques required to achieve profound analgesia while minimizing postoperative opioid consumption and mitigating neurological complications.
Introduction to the Popliteal Sciatic Nerve Block
The evolution of perioperative pain management in orthopedic surgery has increasingly favored regional anesthesia, significantly reducing reliance on systemic opioids and facilitating accelerated rehabilitation protocols. The popliteal sciatic nerve block is a cornerstone technique for providing profound anesthesia and postoperative analgesia for surgical procedures involving the distal lower extremity, specifically the foot, ankle, and distal tibia.
By targeting the sciatic nerve within the popliteal fossa—proximal to its bifurcation into the tibial and common peroneal nerves—the orthopedic surgeon or regional anesthesiologist can achieve comprehensive sensory and motor blockade of the lower leg, sparing only the anteromedial cutaneous territory innervated by the saphenous nerve. This masterclass details the precise anatomical landmarks, biomechanical considerations, and step-by-step surgical techniques for both the prone and lateral approaches to the popliteal sciatic nerve block.
Surgical Anatomy and Neurophysiology
A rigorous understanding of the popliteal fossa's tridimensional anatomy is mandatory for the safe and efficacious execution of this block.
Boundaries of the Popliteal Fossa
The popliteal fossa is a diamond-shaped space located at the posterior aspect of the knee.
* Superolateral Border: Biceps femoris muscle and tendon.
* Superomedial Border: Semitendinosus and semimembranosus muscles.
* Inferior Borders: Medial and lateral heads of the gastrocnemius muscle.
* Floor: Popliteal surface of the femur, the posterior capsule of the knee joint, and the popliteus muscle.
* Roof: Popliteal fascia, which is a continuation of the fascia lata.
The Sciatic Nerve and its Bifurcation
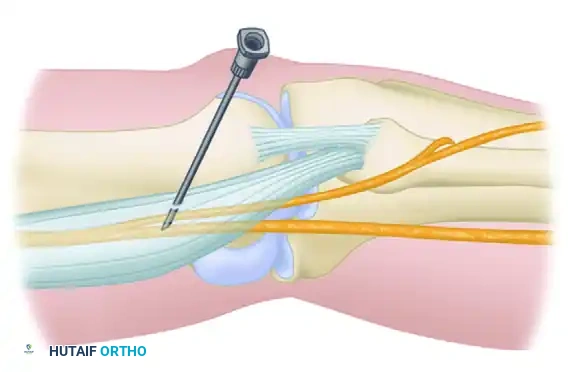
The sciatic nerve (L4-S3) descends through the posterior thigh and typically bifurcates into the tibial nerve (medial) and the common peroneal nerve (lateral) at a variable distance proximal to the popliteal crease. Cadaveric studies indicate that this bifurcation occurs between 5 and 10 cm cephalad to the popliteal crease in the majority of patients.
Both nerves are enveloped within a common epineural sheath (the paraneural sheath or Vloka's sheath) before they physically separate. Injecting local anesthetic within this common sheath—but strictly outside the perineurium of the individual fascicles—results in a rapid, dense, and highly successful block.
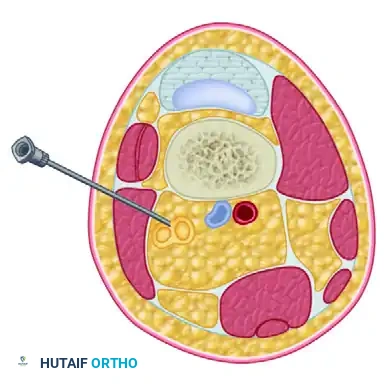
Vascular Relationships
The popliteal artery and vein lie deep (anterior) and medial to the sciatic nerve within the fossa. The nerve is the most superficial and lateral of the major neurovascular structures in this region, making it highly accessible to percutaneous blockade while minimizing the risk of inadvertent vascular puncture, provided the needle trajectory is meticulously controlled.
💡 Clinical Pearl: The Paraneural Sheath
For optimal onset time and block density, the goal is a "sub-paraneural" injection. The local anesthetic should spread circumferentially around both the tibial and common peroneal components within the common sheath, creating a "donut sign" on ultrasound, without breaching the epineurium of the individual nerves.
Indications and Contraindications
Indications
The popliteal sciatic nerve block is indicated for a wide array of orthopedic procedures, including but not limited to:
* Achilles tendon repair and reconstruction.
* Ankle arthrodesis (tibio-talar, subtalar, or triple arthrodesis).
* Open reduction and internal fixation (ORIF) of calcaneal, talar, and complex pilon fractures.
* Forefoot reconstructions (e.g., severe hallux valgus correction, Charcot foot reconstruction).
* Amputations of the foot or toes.
Contraindications
- Absolute: Patient refusal, active infection at the injection site, documented allergy to amide local anesthetics.
- Relative: Pre-existing peripheral neuropathy (e.g., severe diabetic sensorimotor polyneuropathy) where postoperative neurological assessment is critical, severe coagulopathy, or systemic infection.
Preoperative Preparation and Equipment
Standard monitoring (pulse oximetry, electrocardiography, and non-invasive blood pressure) must be applied. Intravenous access is mandatory, and resuscitation equipment, including 20% lipid emulsion therapy for Local Anesthetic Systemic Toxicity (LAST), must be immediately available.
Required Equipment:
* High-frequency linear ultrasound transducer (10–15 MHz).
* Peripheral nerve stimulator.
* Sterile skin preparation (Chlorhexidine gluconate 2%).
* 1% plain lidocaine for local skin infiltration.
* Short-bevel, insulated stimulating block needle (typically 21-gauge, 100 mm).
* 30 to 40 mL of long-acting local anesthetic (e.g., 0.5% Ropivacaine or 0.25%–0.5% Bupivacaine), often mixed with adjuvants like dexamethasone (1-2 mg) to prolong duration.

Surgical Technique: Popliteal Sciatic Nerve Block (Prone)
The prone approach is the classical technique, offering excellent anatomical symmetry and straightforward landmark identification. It is particularly useful when the surgical procedure itself will be performed in the prone position (e.g., Achilles tendon repair).
Step 1: Patient Positioning and Landmark Identification
- Position the patient prone with the legs fully extended. Place a small pillow under the ankles to slightly flex the knees, which relaxes the hamstring tendons and makes the popliteal fossa more palpable.
- Draw a transverse line across the popliteal crease, extending between the prominent tendons of the biceps femoris (lateral) and the semitendinosus/semimembranosus complex (medial).
- Identify and mark the exact midline of this popliteal crease.
- The popliteal fossa triangle is now visually bordered by the semitendinosus-semimembranosus medially, the biceps femoris laterally, and the popliteal crease inferiorly.
Step 2: Needle Insertion Site Mapping
- From the midline of the popliteal crease, measure exactly 7 cm cephalad along the longitudinal midline axis of the posterior thigh.
- From this 7 cm mark, measure 1 cm lateral to the axis. This specific offset accounts for the lateral anatomical bias of the sciatic nerve relative to the midline vessels. Mark this point as the needle insertion site.
Step 3: Preparation and Anesthesia
- Perform a wide sterile preparation of the posterior thigh and knee.
- Raise a superficial skin wheal at the marked insertion site using 1% plain lidocaine and a 25-gauge needle to ensure patient comfort.
Step 4: Nerve Stimulation and Needle Advancement
- Attach the peripheral nerve stimulator according to the manufacturer’s instructions. Place the negative lead (cathode) on the exploring block needle and the positive lead (anode/ground) on the ipsilateral leg (or as directed by specific device polarity to ensure depolarization occurs at the needle tip).
- Direct the 100-mm insulated needle cephalad and parallel to the femur, entering the skin at a 45-degree angle.
- Advance the needle slowly through the subcutaneous tissue and fascia lata, maintaining continuous negative pressure (aspiration) on the syringe to rule out intravascular placement.
- Set the electrical current to 1 mA at a frequency of 1 Hz.
Step 5: Eliciting the Motor Response
- Continue advancement until a brisk motor response is observed.
- Tibial nerve stimulation: Results in plantar flexion and inversion of the foot.
- Common peroneal nerve stimulation: Results in dorsiflexion and eversion of the foot.
- Note: Eliciting a tibial response is generally preferred as it indicates proximity to the larger, more central component of the sciatic nerve, though a combined response is ideal.
- Once a brisk contraction of the gastrocnemius or foot is observed, gradually decrease the current.
- The goal is to maintain a visible, brisk muscle twitch at 0.3 mA to 0.5 mA.
- Crucial Safety Check: If the twitch remains vigorous at < 0.2 mA, the needle tip is likely intraneural. Withdraw the needle 1-2 mm immediately to prevent fascicular injury.
🚨 Surgical Warning: Injection Pressures
Never inject local anesthetic against high resistance. High injection pressure (> 15 psi) is a highly sensitive indicator of intraneural (intrafascicular) needle placement. Injection under high pressure will cause irreversible ischemic and mechanical damage to the nerve fascicles.
Step 6: Injection Protocol
- Once the needle is optimally positioned (twitch present at 0.3 mA, absent at 0.2 mA), inject a test dose of 1 mL of local anesthetic.
- Observe for the immediate disappearance of the muscle twitch (the Raj test). The physical volume of the fluid pushes the nerve away from the needle tip, extinguishing the motor response.
- Confirm verbally with the awake or lightly sedated patient that they do not experience any sharp, radiating pain or paresthesia during the injection.
- Following negative aspiration, administer a total of 35 mL of local anesthetic in 5-mL increments, aspirating gently between each increment to ensure the needle has not migrated into a vessel.
Surgical Technique: Lateral Popliteal Nerve Block
While the prone position is classical, it requires repositioning if the surgery is to be performed supine. Grosser et al. recommended a preoperative lateral popliteal nerve block, which can be seamlessly performed with the patient remaining in the supine position. This is highly advantageous for trauma patients or those with cervical spine instability where prone positioning is contraindicated.
The Lateral Approach
- With the patient supine, the knee is slightly flexed and the leg is internally rotated, or the leg is elevated on a ramp.
- The needle is introduced from the lateral aspect of the thigh, typically 7 to 10 cm proximal to the lateral femoral epicondyle.
- The trajectory passes through the interval between the vastus lateralis (anteriorly) and the biceps femoris (posteriorly).
- The needle is advanced medially and slightly posteriorly toward the posterior aspect of the femur until the sciatic nerve is encountered.
Clinical Outcomes of the Lateral Approach
Grosser et al. demonstrated that performing this block in sedated patients in the operating room provides exceptional postoperative pain control. In their cohort, patients reported virtually no pain immediately postoperatively. The average duration of the block was documented at 14 hours, and they reported zero complications using this specific lateral technique. The lateral approach is now widely considered a standard-of-care alternative to the prone technique.
Modern Integration: Ultrasound-Guided Technique
While landmark and nerve stimulator techniques are foundational, the modern gold standard incorporates real-time ultrasound guidance. Ultrasound allows for direct visualization of the nerve, the needle trajectory, and the spread of the local anesthetic, drastically reducing the required volume of anesthetic and minimizing complication rates.
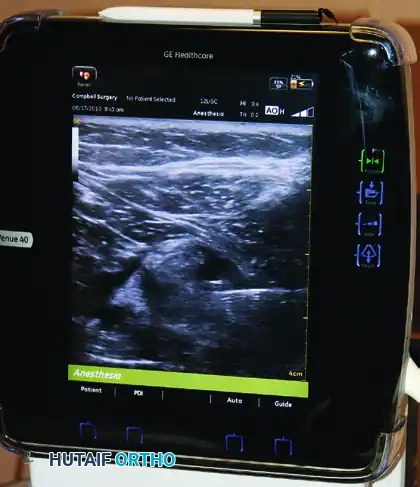
- Place a high-frequency linear transducer transversely across the popliteal crease.
- Identify the pulsatile, hypoechoic popliteal artery. The popliteal vein is usually superficial to the artery and compressible.
- Scan superficially and laterally to identify the tibial nerve (hyperechoic, honeycomb appearance).
- Trace the tibial nerve proximally (cephalad) until the common peroneal nerve joins it to form the unified sciatic nerve. This bifurcation is the optimal target zone.
- Using an in-plane technique (often from lateral to medial), advance the needle until the tip breaches the paraneural sheath.
- Inject 1-2 mL of anesthetic to confirm spread within the sheath. The fluid should separate the sheath from the nerve, creating a hypoechoic halo. Proceed with the remaining volume in aliquots.
Adjunctive Blockade: The Saphenous Nerve
The sciatic nerve supplies the majority of the lower leg, but it does not innervate the anteromedial aspect of the lower leg, the medial malleolus, or the medial aspect of the midfoot. This territory is supplied by the saphenous nerve, a terminal sensory branch of the femoral nerve.
To achieve complete surgical anesthesia or comprehensive postoperative analgesia for procedures involving the medial ankle (e.g., medial malleolus ORIF, total ankle arthroplasty), a supplemental saphenous nerve block is required.
- Technique: With the patient supine, identify the level of the tibial tuberosity.
- Injection: Administer an additional 5 mL of local anesthetic subcutaneously to block the saphenous nerve and its infrapatellar branches as they course superficially along the medial aspect of the proximal tibia.
Postoperative Protocol and Rehabilitation
The profound motor and sensory blockade provided by the popliteal sciatic nerve block necessitates strict postoperative protocols to prevent secondary injury.
- Weight-Bearing Restrictions: Because the block eliminates proprioception and motor control of the foot and ankle, patients must be strictly instructed not to bear weight on the operated limb for 12 to 18 hours postoperatively. Premature weight-bearing can lead to catastrophic falls, ankle sprains, or failure of the surgical fixation.
- Neurological Monitoring: The return of neurological function should be monitored. Patients should be educated that tingling and a gradual return of motor function (ability to wiggle the toes) will occur as the block recedes.
- Rebound Pain Management: As the block's duration averages 14 to 18 hours, patients must be instructed to initiate oral analgesic therapy before the block completely wears off to prevent severe rebound pain.
- Protection of the Insensate Limb: The limb must be properly padded and positioned in the postoperative splint or cast to prevent pressure ulcers, particularly over the heel and fibular head, as the patient will not feel ischemic pain while the block is active.
Conclusion
The popliteal sciatic nerve block, whether performed via the traditional prone landmark technique or the supine lateral approach, is an indispensable tool in the orthopedic surgeon's armamentarium. By mastering the anatomical relationships, adhering to strict nerve stimulation parameters, and integrating modern ultrasound guidance, clinicians can provide superior perioperative care, ensuring optimal surgical conditions and exceptional postoperative pain control for complex foot and ankle reconstructions.
You Might Also Like
