Minimally Invasive Posterior Approach: Techniques, Benefits & Recovery
Key Takeaway
Learn more about Minimally Invasive Posterior Approach: Techniques, Benefits & Recovery and how to manage it. The minimally invasive posterior approach is a surgical technique for the lumbar spine, primarily used for disc excision or nerve root decompression. It involves a small incision and improved imaging, offering benefits like reduced postoperative pain, shorter hospital stays, and earlier return to work compared to classical methods.
Introduction and Epidemiology
The minimally invasive posterior approach to the lumbar spine represents a significant evolution in surgical management for single-level disc and nerve root pathology. This paradigm shift from classical open techniques to less invasive methods has been driven by a confluence of factors, including advancements in imaging, instrumentation, and surgical philosophy focused on tissue preservation. In many specialized spinal units, this approach has largely superseded its open predecessor for indications such as symptomatic lumbar disc herniation and focal spinal stenosis, where direct decompression or disc excision is warranted.
The theoretical and observed advantages of minimally invasive surgery (MIS) often cited include reduced postoperative pain, diminished intraoperative blood loss, shorter hospital stays, and a more expedited return to functional activities and work. These benefits are primarily attributed to the preservation of paraspinal musculature and their innervation, reduced soft tissue dissection, and minimized bone resection compared to traditional open laminectomy or laminotomy. Despite these compelling advantages, the technique is inherently demanding, requiring a steep learning curve and precise execution. It is also associated with a distinct set of potential complications, notably a reported higher incidence of incidental durotomy in some series, underscoring the technical challenge.
Epidemiologically, low back pain is a pervasive global health issue, with a significant proportion attributable to degenerative spinal conditions. Lumbar radiculopathy secondary to disc herniation affects 1-3% of the population annually, while lumbar spinal stenosis affects millions, particularly in an aging demographic. While conservative management remains the cornerstone for most patients, a substantial subset eventually requires surgical intervention. The refinement of MIS posterior approaches has expanded the accessibility of surgical treatment for these conditions, offering potentially superior recovery profiles without compromising long-term efficacy when applied appropriately.
Surgical Anatomy and Biomechanics
A thorough understanding of the regional surgical anatomy and its biomechanical implications is paramount for the safe and effective execution of the minimally invasive posterior lumbar approach. This approach capitalizes on specific anatomical planes to minimize iatrogenic damage.
Lumbar Vertebral Anatomy
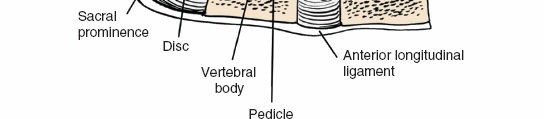
The lumbar spine comprises five vertebrae (L1-L5), characterized by large, kidney-shaped vertebral bodies, robust pedicles, and a triangular vertebral canal. The posterior elements, critical to this approach, include:
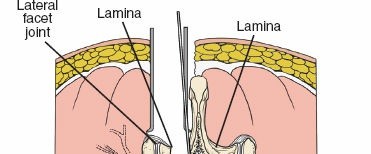
* Laminae: Flat plates extending posteriorly from the pedicles, forming the posterior wall of the vertebral canal.
* Spinous Process: Projects posteriorly and inferiorly from the junction of the laminae.
* Facet Joints (Zygapophyseal Joints): Formed by the superior and inferior articular processes, these synovial joints dictate the pattern of motion and provide posterior stability. The medial aspect of the inferior articular process and the superior articular process are key landmarks for nerve root identification and decompression.
* Transverse Processes: Extend laterally, serving as attachment sites for muscles and ligaments.
* Pars Interarticularis: The segment of bone between the superior and inferior articular processes, a common site for spondylolysis.
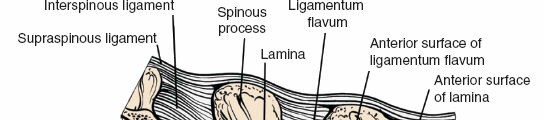
Ligamentous Structures
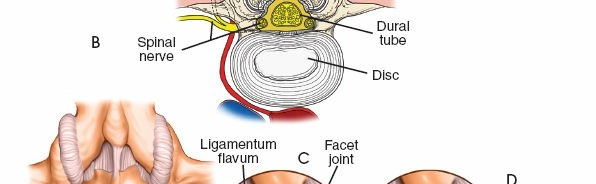
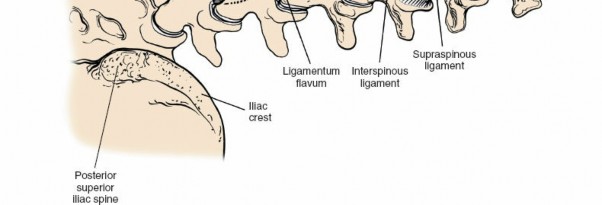
- Ligamentum Flavum: A strong, elastic ligament connecting adjacent laminae. Hypertrophy of this ligament is a common cause of spinal stenosis. Its precise identification and careful resection are central to decompression.
- Posterior Longitudinal Ligament (PLL): Lines the anterior aspect of the vertebral canal, posterior to the vertebral bodies and discs. It resists disc protrusion but is often breached by large central disc herniations.
- Interspinous and Supraspinous Ligaments: Connect the spinous processes and provide posterior stability, often partially disrupted in open approaches but largely preserved in MIS.
Paraspinal Musculature and Internervous Planes
The paraspinal muscles are crucial for spinal stability and motion. The MIS posterior approach specifically aims to preserve these muscles:
* Erector Spinae Group: Composed of iliocostalis (lateral), longissimus (intermediate), and multifidus (medial).
* Multifidus: Deepest and most medial of the erector spinae, originating from sacrum, ilium, transverse processes, and articular processes, inserting onto spinous processes. It is innervated segmentally by the dorsal rami of spinal nerves.
* Longissimus and Iliocostalis: More superficial and lateral, running cranially.
The Wiltse approach or paramedian intermuscular approach, frequently employed in MIS posterior lumbar surgery, exploits the fascial plane between the multifidus (medial) and longissimus (lateral) muscles. This plane is relatively avascular and minimizes denervation and devascularization of the critical multifidus muscle, which is essential for segmental spinal stability. Dissection through this plane allows access to the lamina and facet joint without extensive muscle stripping from the spinous processes and laminae.
Neural Elements
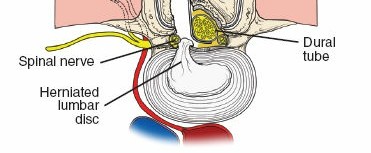
- Dural Sac: The sac containing the spinal cord (conus medullaris typically ends at L1-L2) and the cauda equina (nerve roots below L2).
- Cauda Equina: The bundle of spinal nerve roots below the conus medullaris.
- Spinal Nerve Roots: Exit the spinal canal via the intervertebral foramen. In the lumbar spine, each nerve root exits below its corresponding pedicle (e.g., L5 nerve root exits below the L5 pedicle). Understanding the "shoulder" (axilla) and "axilla" (shoulder) of the nerve root relative to disc herniation is vital.
Biomechanics
The lumbar spine's biomechanics are complex, balancing mobility and stability. The MIS posterior approach aims to restore neurological function by decompressing neural elements while minimizing iatrogenic destabilization. By preserving the posterior ligamentous complex and minimizing facet joint resection, the intrinsic stability of the motion segment is better maintained compared to more aggressive open approaches. This is particularly relevant in preventing or delaying adjacent segment degeneration and postoperative instability. The paramedian approach preserves the central stabilizing multifidus muscles, which are key to segmental control and proprioception.
Indications and Contraindications
Patient selection for the minimally invasive posterior lumbar approach is critical for optimal outcomes and minimizing complications. Improved imaging techniques, particularly high-resolution MRI, have largely eliminated the need for extensive surgical exploration, allowing for precise localization of pathology.
Main Indications
The primary indications revolve around neural element compression, most commonly due to disc herniation or spinal stenosis, recalcitrant to conservative management.
-
Excision of Intervertebral Disc (Microdiscectomy):
- Symptomatic lumbar disc herniation causing radiculopathy (unilateral or bilateral, leg pain predominating over back pain).
- Persistent or progressive neurological deficit despite appropriate conservative therapy (typically 6 weeks or longer).
- Cauda equina syndrome (a surgical emergency).
- Large, contained or extruded disc herniations.
-
Decompression of Spinal Nerve Root (Laminotomy/Partial Facetectomy):
- Unilateral or bilateral lumbar spinal stenosis (central, lateral recess, or foraminal) leading to neurogenic claudication or radiculopathy.
- Symptoms refractory to conservative measures.
- Focal pathology amenable to limited bony and ligamentous resection.
Specific Clinical Scenarios
- Low-Grade Spondylolisthesis (Isthmic or Degenerative): Selected cases of stable, low-grade spondylolisthesis (Meyerding Grade I or II) with symptomatic stenosis may be amenable to MIS decompression without fusion if instability is not the primary driver of symptoms. However, careful consideration is given to the potential for iatrogenic instability.
- Recurrent Disc Herniation: In carefully selected patients, a revision MIS microdiscectomy can be performed, often with increased technical difficulty due to scar tissue.
Contraindications
Contraindications range from absolute to relative, often depending on the extent of pathology, patient comorbidities, and surgeon experience.
-
Absolute Contraindications:
- Active systemic or local spinal infection.
- Significant spinal instability requiring extensive fusion (e.g., high-grade spondylolisthesis, overt degenerative instability).
- Severe multi-level spinal pathology not addressable through a single or limited-level MIS approach.
- Significant neurological deficits mandating rapid, extensive exposure not feasible with MIS (e.g., rapidly progressive myelopathy).
- Severe coagulopathy that cannot be corrected.
- Medical comorbidities precluding general anesthesia.
-
Relative Contraindications:
- Obesity (can increase technical difficulty, fluoroscopy requirements, and incision size).
- Significant prior lumbar surgery with extensive scar tissue (though revision MIS is possible for experienced surgeons).
- Severe spinal deformity.
- Lack of surgeon experience with MIS techniques.
- Diffuse pathology better addressed with a comprehensive open approach.
The decision-making process for operative vs. non-operative management is guided by patient symptomatology, neurological status, imaging findings, and response to conservative therapies.
| Indication Type | Operative Indications | Non-Operative Indications |
|---|---|---|
| Lumbar Disc Herniation | * Persistent radiculopathy despite 6-12 weeks of conservative treatment * Progressive neurological deficit (e.g., worsening motor weakness) * Acute cauda equina syndrome (emergency) * Intractable pain |
* Initial presentation of radiculopathy * Symptoms improving with conservative treatment (NSAIDs, physical therapy, epidural steroid injections) * Mild or stable neurological deficits * Patients unwilling or medically unfit for surgery |
| Lumbar Spinal Stenosis | * Neurogenic claudication severely limiting activity * Persistent radiculopathy refractory to 3-6 months of conservative treatment * Progressive neurological deficit * Failure of epidural steroid injections to provide sustained relief |
* Mild or intermittent neurogenic claudication * Symptoms well-controlled with activity modification or conservative therapies (physical therapy, NSAIDs, epidural steroid injections) * Patients with significant comorbidities making surgery high-risk * Asymptomatic radiographic stenosis |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning and precise patient positioning are foundational to the success and safety of the minimally invasive posterior lumbar approach.
Preoperative Planning
- Imaging Review: A comprehensive review of advanced imaging studies is essential.
- Magnetic Resonance Imaging (MRI): The gold standard for visualizing soft tissue pathology (disc herniation, ligamentum flavum hypertrophy, nerve root compression). T1, T2, and STIR sequences in sagittal, axial, and coronal planes provide detailed anatomical and pathological information. Special attention is paid to the exact level, side, size, and type of disc herniation (e.g., contained, extruded, sequestrated) or the extent and location of stenotic lesions.
- Computed Tomography (CT): Useful for assessing bony anatomy, facet hypertrophy, osteophytes, and prior fusion status, especially when assessing bony impingement or for surgical planning in patients with contraindications to MRI.
- Dynamic Radiographs: Flexion-extension views may be obtained to assess for instability, though typically not the primary indication for MIS decompression.
- Anesthetic Considerations: General anesthesia with endotracheal intubation is standard.
- Neuromonitoring: Somatosensory Evoked Potentials (SSEPs) and Electromyography (EMG) are often employed, particularly for cases involving significant neural element manipulation or complex anatomy, to provide real-time feedback on nerve root integrity.
- Antibiotic Prophylaxis: Administered intravenously 30-60 minutes prior to incision, typically a first or second-generation cephalosporin.
- Deep Vein Thrombosis (DVT) Prophylaxis: Mechanical prophylaxis (sequential compression devices) is routinely used. Pharmacological prophylaxis may be considered based on patient risk factors.
- Equipment Preparation: Ensure availability of appropriate MIS instrumentation, including serial dilators, tubular retractors of various diameters and lengths, specialized microdiscectomy instruments (e.g., pituitary rongeurs, nerve root retractors, Kerrison rongeurs), high-speed burr, and microscopic or endoscopic visualization systems. Fluoroscopy units must be checked and functional.
Patient Positioning
The patient is meticulously positioned to optimize surgical access, minimize complications, and facilitate fluoroscopic imaging.
- Prone Position: The patient is placed in the prone position on a radiolucent operating table.
- Abdomen Free: Critically, the abdomen must be free from compression. This is achieved using specific operating tables (e.g., Jackson table) or by placing chest rolls and iliac bolsters/frame (e.g., Relton frame or Wilson frame). Avoiding abdominal compression prevents engorgement of the epidural venous plexus, thereby minimizing intraoperative bleeding and improving visualization within the spinal canal.

- Maintain Lumbar Lordosis: Proper positioning helps maintain physiological lumbar lordosis, which optimizes the working angle for instruments and avoids flattening of the lumbar spine that can make access to the disc space more challenging.
- Extremities Padded: All pressure points, especially knees, ankles, elbows, and shoulders, are meticulously padded to prevent neuropathies or skin breakdown. The upper extremities are typically placed on armboards or tucked by the patient's side.

- Surgical Site Preparation and Draping: The back from the mid-thoracic region to the sacrum is prepped with an antiseptic solution and sterilely draped, ensuring adequate exposure for fluoroscopy and potential extension of the incision if necessary.
- Fluoroscopy Localization:
- After positioning and draping, a C-arm fluoroscope is brought into the field.
- An initial AP view is taken to confirm the midline and identify relevant spinous processes.
- A lateral view is then obtained to accurately identify and mark the target disc level. A radiopaque marker (e.g., a hypodermic needle or clamp) can be placed on the skin at the projected level of the disc space or the specific lamina/pedicle of interest. This step is critical to avoid wrong-level surgery.
Detailed Surgical Approach and Technique
The minimally invasive posterior approach to the lumbar spine, typically a microdiscectomy or decompression, involves a meticulously executed series of steps to access and decompress the neural elements while minimizing collateral tissue damage.
Incision and Initial Dissection
- Incision: Make a 3-cm longitudinal incision approximately 1 cm lateral to the midline at the level of the disc to be approached. The lateral placement (typically ipsilateral to the pathology) is designed to align with the Wiltse paraspinal intermuscular plane.
- The skin and subcutaneous tissues are incised. Bleeding points are managed with electrocautery.

- The skin and subcutaneous tissues are incised. Bleeding points are managed with electrocautery.
- Deep Fascia and Paraspinal Muscle Dissection:
- The lumbodorsal fascia is incised longitudinally.
- A dissection instrument (e.g., blunt K-wire, Bovie cautery tip, or blunt scissors) is used to identify and enter the Wiltse plane between the multifidus muscle (medially) and the longissimus muscle (laterally). This plane is typically approached obliquely from the skin incision.

- Once the plane is identified, a blunt dilator (e.g., a K-wire or initial probe) is inserted down to the target lamina/facet complex under fluoroscopic guidance to confirm the correct trajectory and depth.

- Serial dilators of increasing diameter are then gently advanced over the initial probe, progressively separating the muscle fibers rather than cutting them. This minimizes muscle trauma and denervation.

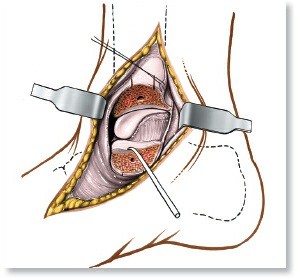
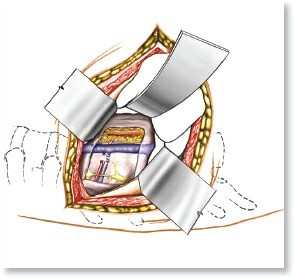
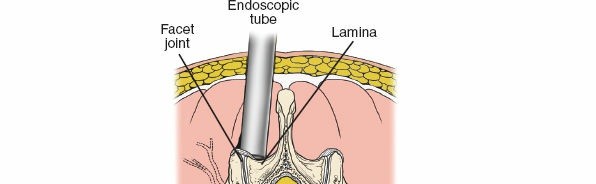
- Tubular Retractor Placement: Once sufficient dilation is achieved (typically to a diameter of 16-22 mm, depending on the pathology and surgeon preference), the tubular retractor is inserted over the final dilator. The dilator is then removed, leaving the tubular retractor docked onto the targeted posterior elements (lamina/facet).
- The retractor is secured to the table or patient, providing a stable working portal.
- The internal aspect of the tube is then cleared of any remaining muscle or soft tissue, and the anatomy within the working channel is confirmed with fluoroscopy.
Exposure and Bone Work
- Anatomical Identification: Within the retractor, the key anatomical landmarks are identified under direct visualization (often with a microscope or endoscope):
- Inferior border of the superior lamina.
- Superior border of the inferior lamina.
- Medial aspect of the facet joint capsule.
- Ligamentum flavum spanning the interlaminar space.

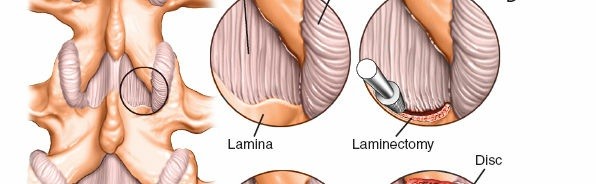
- Laminotomy and Medial Facetectomy:
- For a discectomy, a small laminotomy is typically performed at the inferior edge of the superior lamina to gain access to the interlaminar space. This is done with a high-speed burr or osteotome.
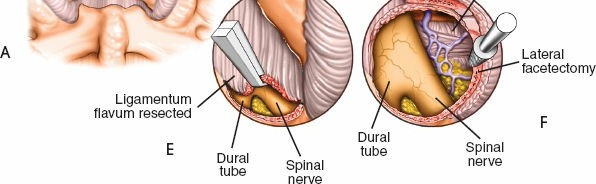
- A portion of the ligamentum flavum is resected to expose the underlying dural sac and nerve root. This "flavotomy" usually begins unilaterally. Kerrison rongeurs are used to meticulously remove the ligamentum flavum.

- In cases of lateral recess stenosis or foraminal compression, a limited medial facetectomy of the superior articular process may be required to adequately decompress the nerve root. Care must be taken to preserve at least 50% of the facet joint to maintain spinal stability.

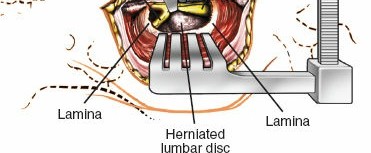
Neural Decompression and Disc Excision
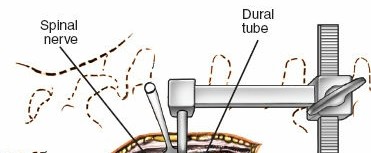
- Dural and Nerve Root Identification: Once the ligamentum flavum is adequately resected, the dural sac and traversing nerve root are carefully visualized. The nerve root's shoulder and axilla are identified relative to the disc space.

- Nerve Root Retraction: A specialized nerve root retractor is gently placed to retract the nerve root medially, exposing the posterolateral aspect of the annulus and any herniated disc material. Careful, minimal retraction is paramount to prevent neural injury.

- Annulotomy and Disc Excision (Microdiscectomy):
- The annulus fibrosus is identified. A small annulotomy is created with a scalpel (No. 11 blade) or rongeur.
- Disc fragments are then carefully removed using various sizes of pituitary rongeurs. Large, extruded fragments are removed first. The disc space is then probed to remove loose fragments.


- The goal is thorough decompression, not necessarily complete disc removal, to avoid destabilization. The disc space is typically not curetted aggressively to reduce the risk of endplate damage and subsequent subsidence or accelerated degeneration.
- Final Assessment: After disc removal or decompression, the nerve root is inspected for free mobility. The dural sac should appear pulsatile and decompressed. Hemostasis is meticulously achieved within the disc space and epidural space.

Closure
- Irrigation and Hemostasis: The surgical site is thoroughly irrigated with saline. Any remaining bleeding points are coagulated. Epidural hemostasis is critical.
- Retractor Removal: The tubular retractor is slowly and carefully removed. As it is withdrawn, suction is applied to the tract to ensure hemostasis and remove any residual blood, preventing hematoma formation.
- Fascial, Subcutaneous, and Skin Closure: The lumbodorsal fascia is typically closed with absorbable sutures to re-approximate the muscle planes. Subcutaneous tissue is closed, followed by meticulous skin closure using sutures, staples, or adhesive strips. A small drain is generally not required for single-level microdiscectomy.
Complications and Management
While the minimally invasive posterior approach offers numerous advantages, it is not without potential complications. Awareness of these, their incidence, and appropriate management strategies is essential for all spine surgeons. The reported complication rates vary depending on the patient population, surgeon experience, and specific technique employed.
Common Complications
| Complication | Incidence (Approximate) | Management and Salvage Strategies |
|---|---|---|
| Dural Tear / Incidental Durotomy | 1-15% (higher in MIS than open in some series) | * Intraoperative: Immediate recognition is key. Direct repair with fine non-absorbable sutures (e.g., 5-0 or 6-0 Prolene) is preferred. Augmentation with dural substitutes (e.g., fascia, fat graft, synthetic dural sealant) may be used. Valsalva maneuver to confirm water-tight closure. * Postoperative: Strict bed rest, avoidance of Valsalva, prophylactic lumbar drain placement for 24-72 hours if repair is tenuous or difficult. Oral acetazolamide to reduce CSF production. Management of pseudomeningocele may require revision surgery. |
| Nerve Root Injury | 0.1-2% | * Intraoperative: Gentle retraction is paramount. Excessive force or direct trauma from instruments. If injury suspected, cessation of procedure, assessment of nerve function (EMG), and repair if transected. * Postoperative: Steroids for inflammation. Neuropathic pain management. Consider nerve conduction studies/EMG. Exploration if severe or progressive deficit, or if persistent compression suspected. |
| Incomplete Decompression | 1-5% | * Intraoperative: Thorough inspection of the neural elements after decompression, confirming free mobility of the nerve root and dural sac. * Postoperative: Persistent radicular pain. Re-evaluation with MRI. May require revision surgery to remove residual disc fragment, osteophyte, or hypertrophied ligamentum flavum. |
| Recurrent Disc Herniation | 5-15% (can be higher for MIS initially) | * Postoperative: New onset or recurrence of radicular pain, often within 3-6 months. * Management: Initial conservative management. MRI to confirm recurrence. If symptoms are severe or persistent, revision microdiscectomy is indicated. Fusion may be considered for multiple recurrences or evidence of instability. |
| Infection (Surgical Site) | 0.1-1% (generally lower for MIS) | * Superficial: Erythema, warmth, purulent discharge. Managed with oral antibiotics, wound care. * Deep: Fever, severe pain, purulent discharge, elevated inflammatory markers. Requires surgical debridement, intravenous antibiotics, and wound culture-directed therapy. |
| Epidural Hematoma | <0.5% | * Postoperative: Acute onset of severe back pain, radicular symptoms, or neurological deficit. * Management: Emergency MRI to confirm. Surgical evacuation of the hematoma is often required to prevent permanent neurological damage. Meticulous hemostasis intraoperatively is key to prevention. |
| Vascular Injury | Extremely rare | * Intraoperative: Catastrophic, often involving major vessels (e.g., iliac vessels) anterior to the disc space, typically due to aggressive anterior penetration with instruments (e.g., pituitary rongeurs). * Management: Immediate recognition, direct pressure, vascular surgery consultation. Potential for exsanguination. |
| Persistent Postoperative Pain | Variable, up to 10-20% | * Can be due to incomplete decompression, nerve root irritation, arachnoiditis, psychosocial factors, or non-spinal generators. * Management: Thorough diagnostic workup (MRI, nerve blocks, psychological evaluation). Multidisciplinary pain management, physical therapy, pharmacological interventions. |
Specific Considerations for MIS
- Learning Curve: The initial learning curve for MIS techniques may be associated with higher complication rates, particularly dural tears, until adequate proficiency is achieved. Supervised training and simulation are crucial.
- Limited Field of View: The tubular retractor provides a narrow, deep field of view, which can obscure adjacent anatomy and increase the risk of missing pathology or causing unintended injury. Meticulous orientation and fluoroscopic checks are essential.
- Radiation Exposure: Increased reliance on fluoroscopy for localization and confirmation translates to increased radiation exposure for both the patient and the surgical team. Strategies to minimize exposure include pulsed fluoroscopy, last-image hold, and appropriate shielding.
Proactive intraoperative risk mitigation strategies, including diligent anatomical identification, meticulous hemostasis, gentle tissue handling, and liberal use of fluoroscopy (within safe limits), are paramount in minimizing the incidence of these complications.
Post Operative Rehabilitation Protocols
A structured and progressive postoperative rehabilitation protocol is integral to achieving optimal functional outcomes following minimally invasive posterior lumbar surgery. The goals are to manage pain, facilitate early mobilization, restore functional strength and flexibility, and enable a safe return to activities of daily living and work. The minimally invasive nature of the procedure typically allows for a more accelerated recovery pathway compared to traditional open surgery.
Immediate Postoperative Period (Days 0-7)
- Pain Management: A multimodal pain management strategy is employed, combining opioid analgesics, NSAIDs (if not contraindicated), and acetaminophen to control postoperative discomfort and facilitate early mobilization. Patient-controlled analgesia (PCA) may be utilized initially.
- Early Mobilization: Patients are encouraged to ambulate within hours of surgery or on postoperative day 1. This minimizes the risks of DVT, pulmonary complications, and muscle deconditioning.
- Activity Restrictions:
- Avoid bending, lifting (typically >5-10 lbs), and twisting (BLT precautions) for the initial 4-6 weeks.
- Limit prolonged sitting (e.g., to 20-30 minutes at a time) to reduce intradiscal pressure.
- No strenuous activities, running, or heavy exercise.
- Activity Restrictions:
- Wound Care: Incision site is monitored for signs of infection (erythema, swelling, discharge). Dressing changes as per institutional protocol.
- Patient Education: Comprehensive instruction on proper body mechanics, posture, and activity limitations is provided to the patient and family.
Early Rehabilitation Phase (Weeks 2-6)
- Initiation of Physical Therapy: Referral to a skilled physical therapist is typically made around 2-4 weeks postoperative, once acute pain has subsided.
- Therapeutic Exercises:
- Core Stabilization: Emphasis on activating deep abdominal muscles (transversus abdominis) and lumbar multifidus to improve trunk stability without stressing the surgical site. Examples include pelvic tilts, gentle abdominal bracing, and bird-dog exercises (modified initially).
- Flexibility: Gentle stretching of hamstrings and hip flexors, avoiding excessive lumbar flexion or rotation.
- Walking Program: Gradual increase in walking duration and intensity.
- Progression of Activities: Light housework and sedentary work may be resumed as tolerated, adhering to BLT precautions. Driving can typically resume when off narcotic pain medication and comfortable turning/twisting.
Intermediate Rehabilitation Phase (Weeks 6-12)
- Progression of Strength and Endurance:
- Advanced Core Strengthening: Progressing to more challenging exercises for the core, back extensors, and gluteal muscles.
- General Conditioning: Incorporating low-impact aerobic activities such as cycling, swimming, or elliptical training.
- Gradual Increase in Resistance: Light resistance training for upper and lower extremities.
- Activity Modification: Gradual loosening of activity restrictions as strength and flexibility improve. Heavy lifting remains restricted.
- Occupational Therapy (if indicated): For patients with physically demanding jobs, an occupational therapist may provide job-specific training and ergonomic assessment.
Advanced Rehabilitation Phase (Beyond 12 Weeks)
- Return to Full Activity: Gradual return to more demanding recreational and occupational activities, including sports, as strength, endurance, and comfort allow. This phase is highly individualized.
- Maintenance Program: Emphasis on a lifelong home exercise program to maintain core strength and flexibility, and to continue practicing good body mechanics.
- Follow-up: Scheduled clinical follow-up visits with the surgeon to monitor progress, address concerns, and guide activity progression. Radiographic evaluation is typically not necessary unless new symptoms or complications arise.
The success of postoperative rehabilitation relies heavily on patient adherence, appropriate guidance from the rehabilitation team, and a realistic expectation of recovery timelines. While MIS often accelerates early recovery, the full healing process and return to peak function can still take several months.
Summary of Key Literature and Guidelines
The evolution of the minimally invasive posterior lumbar approach has been extensively studied, with a growing body of literature supporting its efficacy and defining its role in modern spinal surgery. Key findings and professional guidelines inform current best practices.
Comparative Studies: MIS vs. Open Surgery
Numerous randomized controlled trials and systematic reviews have compared MIS microdiscectomy and decompression to traditional open techniques for lumbar disc herniation and stenosis.
-
Lumbar Microdiscectomy:
- Early studies consistently demonstrated that MIS microdiscectomy results in less intraoperative blood loss, reduced postoperative pain, shorter hospital stays, and a quicker return to work compared to open microdiscectomy.
- Long-term functional outcomes and reoperation rates for recurrent disc herniation are generally considered comparable between MIS and open approaches. However, some literature suggests a slightly higher recurrence rate with MIS in the very early postoperative period, possibly due to less aggressive disc material removal or the learning curve.
- The SPORT (Spine Patient Outcomes Research Trial) study, while not directly comparing MIS to open, established the efficacy of both surgical and non-surgical treatments for disc herniation, providing a benchmark for outcomes against which MIS techniques are measured.
-
Lumbar Decompression for Stenosis:
- For single-level or focal multilevel stenosis, MIS decompression (e.g., unilateral laminotomy for bilateral decompression) has shown similar neurological outcomes and symptom relief to open laminectomy, with the added benefits of reduced tissue trauma, blood loss, and earlier functional recovery.
- Systematic reviews and meta-analyses have largely confirmed these advantages, while acknowledging the technical demand and potential for a higher dural tear rate during the learning curve.
- The long-term stability and incidence of iatrogenic instability following MIS decompression are favorable due to significant preservation of the posterior tension band and facet joints.
Dural Tear Incidence
As highlighted in the initial seed content, dural tears have been reported with a slightly higher incidence in some MIS series compared to open surgery, particularly during the early phase of a surgeon's learning curve. This is attributed to the confined working space, limited peripheral visualization, and potentially different tactile feedback. However, with increasing surgeon experience and refinement of techniques, the incidence has been shown to decrease and approach that of open procedures. When recognized and repaired appropriately, the long-term clinical sequelae are usually minimal.
Cost-Effectiveness
Studies evaluating the cost-effectiveness of MIS approaches have yielded mixed results. While the initial surgical costs (instrumentation, operating room time) might be higher, the potential for reduced hospital stay, decreased need for postoperative analgesia, and faster return to work can offset these costs, leading to overall comparable or even lower societal costs in the long run.
Professional Guidelines and Consensus Statements
Major professional organizations, such as the North American Spine Society (NASS) and AOSpine, issue evidence-based guidelines for the management of lumbar degenerative conditions, including surgical recommendations. These guidelines generally support the use of MIS posterior approaches for carefully selected patients with symptomatic lumbar disc herniation or focal stenosis refractory to conservative management. Key recommendations emphasize:
- Patient Selection: Strict adherence to indications and contraindications.
- Surgeon Expertise: The importance of appropriate training and experience in MIS techniques.
- Imaging: Comprehensive preoperative imaging for accurate diagnosis and surgical planning.
- Risk-Benefit Analysis: Thorough discussion with patients regarding the potential benefits and risks, including technique-specific complications.
Future Directions
The field of MIS lumbar surgery continues to evolve rapidly:
- Enhanced Recovery After Surgery (ERAS) Protocols: Integration of MIS into comprehensive ERAS pathways is further optimizing perioperative care, focusing on preoperative patient optimization, opioid-sparing analgesia, and early mobilization.
- Robotics and Navigation: Robotic guidance systems and advanced navigation platforms are being developed to improve accuracy, reduce radiation exposure, and potentially lower the learning curve for complex MIS procedures.
- Endoscopic Spine Surgery: Fully endoscopic techniques are gaining traction, offering even smaller incisions and potentially further reduced tissue trauma, albeit with a unique and steep learning curve.
- Instrumentation and Technology: Ongoing advancements in retractors, visualization systems (3D exoscopes), and specialized instruments continue to refine the precision and safety of these procedures.
In conclusion, the minimally invasive posterior approach to the lumbar spine represents a validated and often preferred surgical option for targeted decompression and disc excision. Its advantages in terms of reduced morbidity and accelerated recovery are well-established, provided meticulous surgical technique, careful patient selection, and comprehensive postoperative rehabilitation are employed. Continuous research and technological innovation are further solidifying its role in contemporary spinal surgery.
Clinical & Radiographic Imaging

You Might Also Like