Forequarter Amputation: Surgical Techniques & Protocols
Key Takeaway
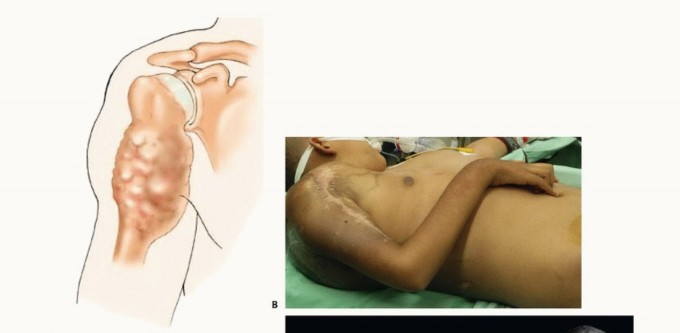
Forequarter amputation, or interscapulothoracic amputation, is a radical salvage procedure involving the en bloc resection of the entire upper extremity, including the scapula and clavicle. Primarily indicated for advanced malignant tumors precluding limb-sparing surgery, this procedure demands meticulous neurovascular control. The surgical execution relies on either the classic anterior approach of Berger or the highly efficient posterior approach of Littlewood, requiring profound anatomical mastery to ensure oncologic clearance and patient survival.
Introduction and Epidemiology
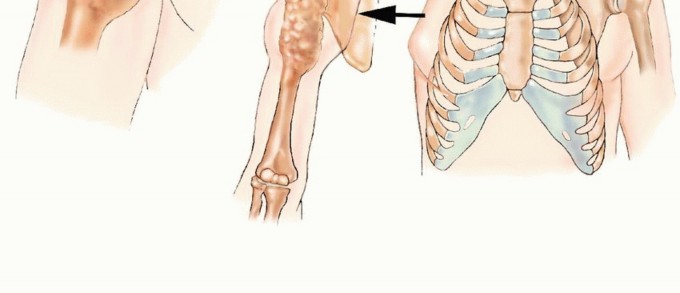
Forequarter amputation, formally known as interscapulothoracic amputation, represents one of the most radical and anatomically complex ablative procedures performed in orthopedic oncology. The procedure entails the en bloc removal of the entire upper extremity, the scapula, and the lateral aspect of the clavicle. Historically described by Paul Berger in 1887, this mutilating amputation was traditionally the standard of care for high-grade primary bone and soft tissue sarcomas arising around the proximal humerus, scapula, and axilla.
In contemporary orthopedic oncology, the epidemiological landscape and treatment paradigms for shoulder girdle sarcomas have evolved significantly. Advances in multimodal therapies, including targeted neoadjuvant chemotherapy, refined radiation therapy protocols, and the development of sophisticated modular endoprosthetic reconstructions, have relegated the forequarter amputation to a rare procedure. Currently, limb-sparing resections are considered safe and oncologically equivalent alternatives in 90% to 95% of cases involving the proximal humerus and periscapular region.

Despite the success of limb salvage, forequarter amputation remains an indispensable surgical option in the modern armamentarium. It is primarily reserved for massive, neglected, or recurrent sarcomas that exhibit extensive neurovascular encasement or chest wall invasion, where limb salvage would result in a functionally useless appendage or compromise oncologic margins. Furthermore, it serves a critical palliative role in cases of intractable pain, fungating tumor masses, or severe radiation-induced brachial plexopathy complicated by chronic infection or ulceration.

The incidence of forequarter amputation is directly proportional to the presentation of advanced local disease. Primary tumors necessitating this approach most frequently include high-grade osteosarcoma, chondrosarcoma, Ewing sarcoma, and aggressive soft tissue sarcomas such as undifferentiated pleomorphic sarcoma and synovial sarcoma. Metastatic lesions to the shoulder girdle rarely require such radical ablation unless complicated by massive soft tissue extension and intractable pain refractory to standard palliative measures.

Surgical Anatomy and Biomechanics
A profound understanding of the complex three-dimensional anatomy of the shoulder girdle, cervicothoracic junction, and axilla is paramount for the safe execution of a forequarter amputation. The upper extremity and scapula are suspended from the axial skeleton and upper torso by a complex network of soft tissue elements and a single bony articulation at the sternoclavicular joint.

Osteology and Articular Anatomy
The bony framework involved in the resection includes the humerus, the scapula, and the lateral portion of the clavicle. The clavicle acts as the sole osseous strut connecting the appendicular skeleton to the axial skeleton. During a standard forequarter amputation, a clavicular osteotomy is performed, typically at the junction of the medial and middle thirds, to gain access to the underlying neurovascular structures. The scapula glides over the posterior thoracic wall, separated by the serratus anterior and subscapularis muscles, forming the scapulothoracic articulation.
Muscular Anatomy and Myofascial Planes
The muscular attachments that must be systematically identified and transected are divided into anterior, posterior, and medial groups.
* Anteriorly: The pectoralis major and minor muscles anchor the humerus and coracoid process to the anterior chest wall. The subclavius muscle lies deep to the clavicle, protecting the underlying neurovascular bundle.
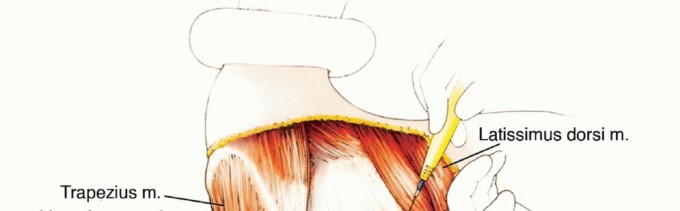
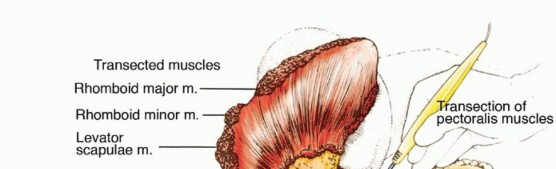
* Posteriorly: The trapezius, latissimus dorsi, rhomboid major and minor, and levator scapulae tether the scapula and humerus to the spinous processes and posterior cervical structures.
* Medially: The serratus anterior anchors the medial border of the scapula to the lateral ribs.
Large tumors of the periscapular area can easily violate these fascial compartments, extending into the posterior triangle of the neck, the adjacent paraspinal musculature, or directly invading the underlying ribs and intercostal spaces. Tumor extension into these anatomic sites must be meticulously evaluated, as en bloc resection of a chest wall segment may be required to achieve negative margins.
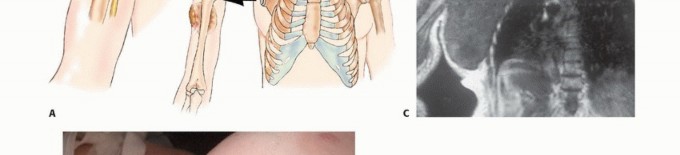
Neurovascular Structures
The critical step in forequarter amputation is the safe isolation and ligation of the subclavian/axillary vessels and the brachial plexus. The subclavian artery and vein transition to the axillary vessels at the lateral border of the first rib. These structures, along with the infraclavicular portion of the brachial plexus, pass immediately inferior to the clavicle and the coracoid process, lying deep to the deltopectoral fascia and pectoralis minor.
The brachial plexus must be transected sharply under tension to allow the proximal nerve stumps to retract deep into the neck musculature, minimizing the risk of symptomatic neuroma formation. The anatomical relationship of the tumor to the thoracic outlet dictates the level of neurovascular transection; massive tumors may require an intra-thoracic or highly proximal extra-thoracic ligation.
Indications and Contraindications
The decision to proceed with a forequarter amputation is complex and requires rigorous multidisciplinary evaluation. The primary goal is achieving an R0 (microscopically negative) oncologic margin while balancing the severe functional and psychological impact of the procedure.
Primary Surgical Indications
- Massive Soft Tissue Sarcomas: Large soft tissue tumors around the proximal arm or axilla demonstrating extensive neurovascular encasement, compromise of the brachial plexus, and extension across the glenohumeral joint, precluding functional limb salvage.
- Advanced Primary Bone Tumors: High-grade primary bone sarcomas (e.g., osteosarcoma, chondrosarcoma) of the proximal humerus or scapula with an extensive extraosseous soft tissue component invading the shoulder joint, axilla, and surrounding muscular compartments.
- Locoregional Recurrence: Extensive locoregional tumor recurrence around the shoulder girdle following previous limb-sparing surgery and radiation therapy, where further salvage attempts are oncologically or technically unfeasible.
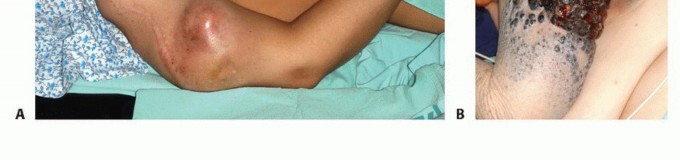
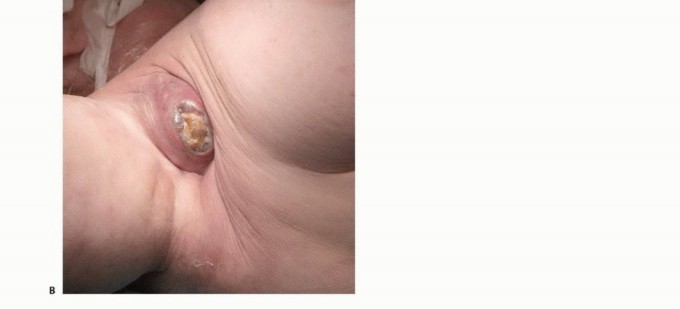
- Palliative Ablation: Palliation of intractable pain, severe infection, or tumor fungation associated with a rapidly enlarging, necrotic lesion that has failed to respond to systemic chemotherapy and radiation therapy.
- Radiation-Induced Complications: Severe radiation-induced brachial plexopathy resulting in a flail, insensate, and painful limb, often complicated by chronic ulceration or secondary radiation-induced sarcomas.
Contraindications and Special Considerations
Forequarter amputation is generally contraindicated when the tumor exhibits massive extension into the mediastinum, extensive involvement of the posterior triangle of the neck, or widespread paraspinal muscle invasion that precludes achieving negative margins even with extended resections.
However, special considerations exist for highly selected patients without distant metastases. In cases of localized chest wall invasion, a concomitant en bloc chest wall resection (including ribs and pleura) can be performed. Similarly, limited extension into the neck may be managed with a concurrent radical neck dissection. These extended procedures demand a patient capable of withstanding the severe physiologic insult of combined major surgeries.
Operative vs Non Operative Management
| Clinical Scenario | Recommended Management Strategy | Rationale and Considerations |
|---|---|---|
| Proximal Humerus Sarcoma (No NV encasement) | Limb-Sparing Resection + Endoprosthesis | Standard of care; achieves R0 margins with preserved hand/elbow function. |
| Axillary Sarcoma with Brachial Plexus Encasement | Forequarter Amputation | Resection of plexus yields a flail limb; amputation provides definitive local control. |
| Fungating, Bleeding Tumor (Metastatic Disease) | Palliative Forequarter Amputation | Improves quality of life, controls hemorrhage, eliminates source of sepsis. |
| Massive Tumor invading Mediastinum/Spine | Non-Operative / Systemic Therapy | R0 margin impossible; surgery carries prohibitive morbidity without survival benefit. |
| Recurrent Sarcoma post-Radiation (Flail Limb) | Forequarter Amputation | Salvage procedure for definitive local control and pain relief. |

Pre Operative Planning and Patient Positioning
Thorough preoperative planning is critical to the success and safety of a forequarter amputation. The surgical team must have a precise understanding of the tumor's margins and its relationship to the critical neurovascular structures of the thoracic outlet.
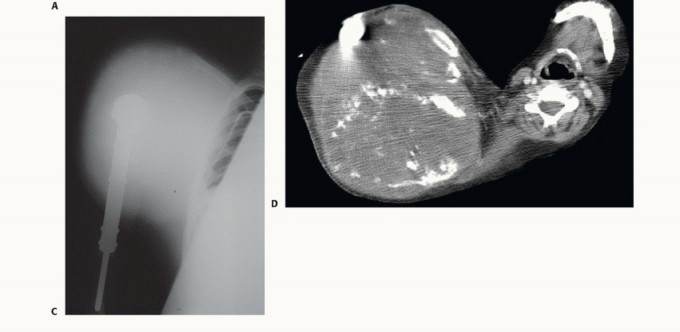
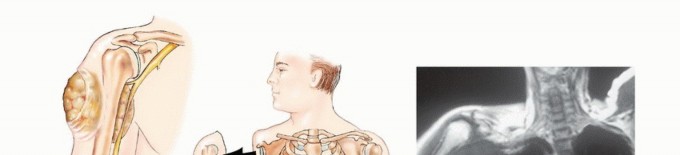
Advanced Imaging Modalities
Magnetic Resonance Imaging (MRI) of the entire shoulder girdle, including the brachial plexus and cervicothoracic junction, is mandatory. MRI provides superior soft tissue contrast to delineate tumor extension into the paraspinal muscles, chest wall, and axillary sheath. Computed Tomography (CT) of the chest is required for pulmonary staging and to assess for bony destruction of the ribs or spine.
A CT Angiogram or standard angiography is highly recommended for massive tumors to map the vascular displacement and identify feeding vessels. In highly vascular tumors (e.g., metastatic renal cell carcinoma or thyroid carcinoma), preoperative transcatheter arterial embolization performed 24 to 48 hours prior to surgery can significantly reduce intraoperative blood loss.
Anesthesia and Hemodynamic Monitoring
Given the potential for massive, rapid blood loss, invasive hemodynamic monitoring is required. This includes an arterial line and a central venous catheter. Two large-bore peripheral intravenous lines and the availability of a rapid infuser are standard. The anesthesia team must have cross-matched blood readily available in the operating room. A multidisciplinary approach involving thoracic or vascular surgery should be coordinated if chest wall resection or proximal vascular control at the sternum is anticipated.
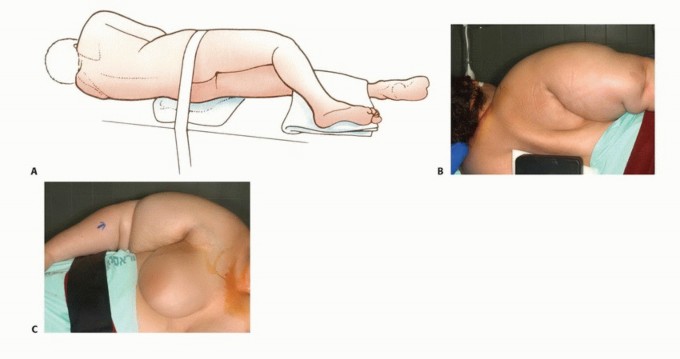
Patient Positioning and Draping
The patient is typically positioned in a full lateral decubitus position or a "floppy lateral" position, utilizing a vacuum bean bag for stability. This position allows simultaneous access to the anterior chest, the axilla, and the posterior scapular region.
The entire upper extremity, shoulder girdle, hemithorax (from the sternal notch to the spine), and the ipsilateral neck (up to the mandible) are prepped and draped free. The arm is wrapped in a sterile stockinette to allow for free manipulation during the procedure, which aids in exposing various fascial planes.
Detailed Surgical Approach and Technique
The classic anterior approach (Berger technique) is the most widely utilized method for forequarter amputation. The procedure is systematically divided into anterior neurovascular control, posterior muscular release, and inferior/medial detachment.
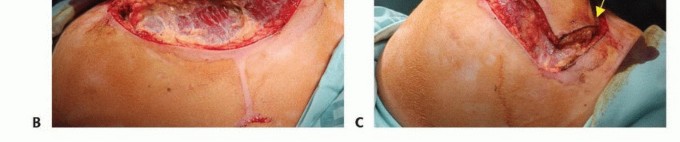
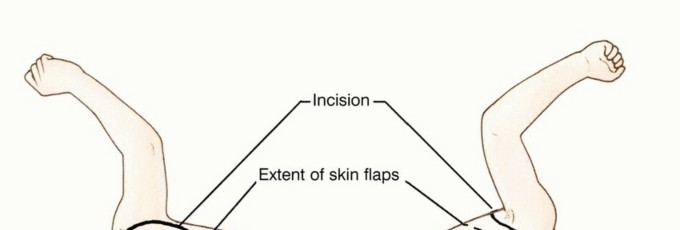
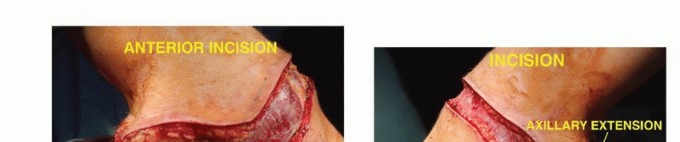
Incision and Flap Design
A racquet-shaped incision is utilized. The anterior limb begins at the medial third of the clavicle, extending laterally and inferiorly along the deltopectoral groove, crossing the axilla. The posterior limb originates at the lateral aspect of the clavicular incision, extending posteriorly over the acromion and continuing inferiorly along the vertebral border of the scapula to meet the anterior incision at the inferior angle of the scapula. The exact design must be modified based on the tumor location to ensure adequate oncologic margins, often requiring the sacrifice of overlying skin and the creation of custom myocutaneous flaps.
Anterior Dissection and Clavicular Osteotomy
The initial step involves deepening the anterior incision through the subcutaneous tissue and platysma. The supraclavicular nerves are identified and transected. The periosteum of the clavicle is incised at the junction of the medial and middle thirds. A malleable retractor is carefully passed deep to the clavicle to protect the underlying subclavian vein. A Gigli saw or an oscillating saw is used to perform the clavicular osteotomy. The lateral segment of the clavicle is elevated and retracted laterally, exposing the subclavius muscle, which is subsequently divided.

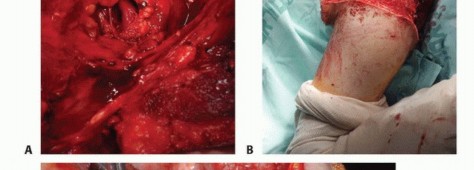
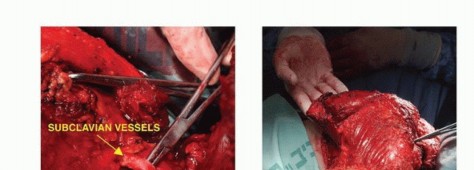
Neurovascular Isolation and Ligation
Elevation of the clavicle provides direct access to the neurovascular bundle. The deep cervical fascia is incised. The subclavian artery and vein are meticulously skeletonized.
Standard oncologic principles dictate that the artery should be ligated first to allow venous drainage of the extremity, thereby reducing blood loss and returning blood volume to the systemic circulation. However, if the tumor is highly friable or if there is a high risk of tumor embolization, the vein may be ligated first. Both vessels are doubly ligated with heavy non-absorbable sutures and transfixed.
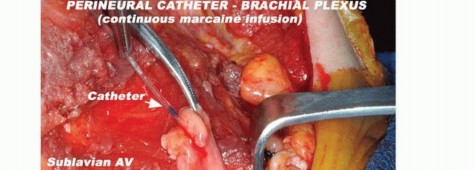
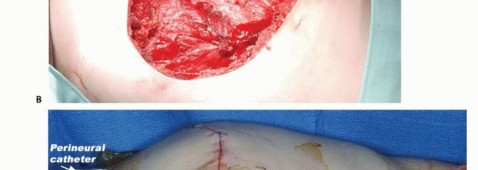
Following vascular control, the trunks or cords of the brachial plexus are identified. To prevent the formation of painful postoperative neuromas, each nerve is placed under gentle distal traction, injected with a long-acting local anesthetic (e.g., bupivacaine), and sharply transected with a scalpel. The proximal stumps are allowed to retract deep into the cervical musculature.

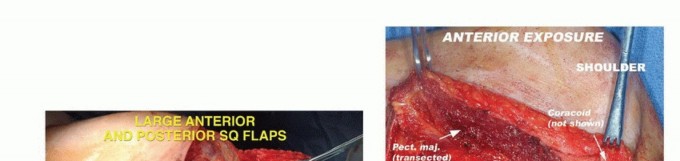
Anterior Muscular Transection
With the neurovascular bundle divided, the anterior muscular attachments are released. The pectoralis major is transected near its clavicular and sternal origins, or closer to its humeral insertion depending on the required tumor margin. The pectoralis minor is divided near the coracoid process. The latissimus dorsi is identified in the axilla and transected.
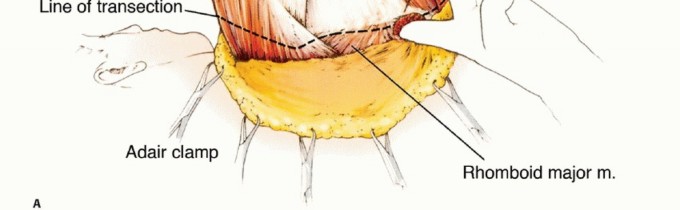
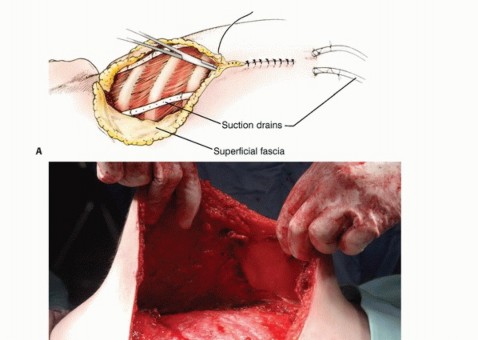
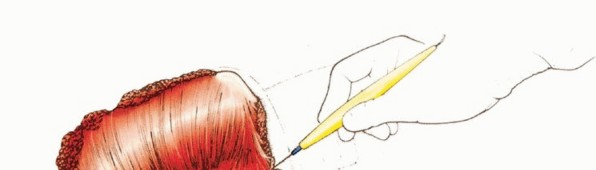
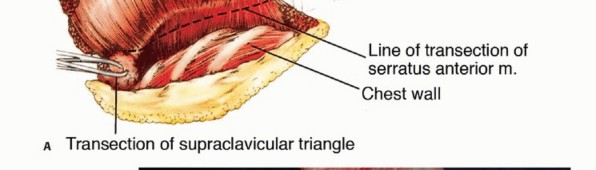
Posterior and Medial Dissection
The patient is rolled slightly forward, and the arm is brought across the chest to place the posterior musculature under tension. The posterior skin incision is deepened. The trapezius muscle is divided along its attachment to the spine of the scapula and acromion.
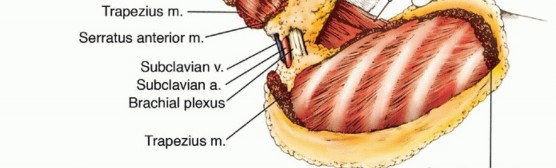
Deep to the trape
Clinical & Radiographic Imaging


You Might Also Like


