Achieve Perfect Reduction: Managing Radial Styloid Fractures with Arthroscopy
Key Takeaway
We review everything you need to understand about Achieve Perfect Reduction: Managing Radial Styloid Fractures with Arthroscopy. Radial styloid fractures are isolated breaks of the radial styloid, often ideally managed arthroscopically for precise reduction. This approach is beneficial for detecting associated scapholunate ligament injuries and ensuring anatomical alignment, preventing rotational displacement often missed by fluoroscopy. Arthroscopic fixation typically uses cannulated screws for stable repair, decreasing soft tissue irritation compared to K-wires.
Introduction and Epidemiology
Fractures of the radial styloid, often termed Chauffeur's or Hutchinson fractures, represent a distinct subset within the spectrum of distal radius injuries. Characterized by an oblique fracture line propagating from the radial articular surface proximally, these injuries typically result from an axial load applied to the scaphoid, driving it into the radial styloid. While often considered an isolated injury, radial styloid fractures frequently occur in conjunction with other carpal pathologies, particularly scapholunate interosseous ligament (SLIL) tears, making their accurate assessment and management critical for optimal long-term wrist function.
The epidemiology of radial styloid fractures generally aligns with that of other distal radius fractures, with a bimodal distribution peaking in younger, active individuals involved in high-energy trauma (e.g., motor vehicle accidents, sports injuries) and in older, osteoporotic populations following low-energy falls. The hallmark of an ideal treatment strategy for these injuries is the restoration of articular congruity, radial length, and radial inclination, alongside the identification and management of associated soft tissue injuries, which are paramount in preventing post-traumatic arthritis and carpal instability.
Arthroscopic assistance in the management of radial styloid fractures has emerged as a superior technique, particularly for achieving anatomical reduction and comprehensively addressing concomitant intra-articular pathologies. Its direct visualization capabilities offer an unparalleled advantage over traditional fluoroscopic guidance alone, enabling the surgeon to detect and correct subtle rotational deformities and articular step-offs that might otherwise be missed. Furthermore, for surgeons developing proficiency in arthroscope-assisted fixation of distal radius fractures, an isolated radial styloid fracture often serves as an ideal entry point due to its relatively confined nature and the clear benefits of direct articular visualization.
Surgical Anatomy and Biomechanics
Radial Styloid Anatomy
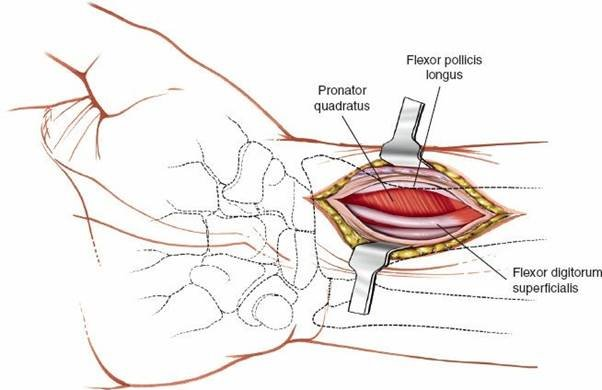
The radial styloid process is the most lateral projection of the distal radius, extending approximately 9-12 mm further distally than the ulnar head. It forms the lateral wall of the radiocarpal joint and serves as the primary articulation point for the scaphoid. The articular surface of the distal radius is primarily composed of two distinct facets: the scaphoid facet, which articulates with the scaphoid, and the lunate facet, which articulates with the lunate. The radial styloid is integral to the scaphoid facet and is bordered by a robust network of ligamentous structures crucial for carpal stability.
Key ligamentous attachments to the radial styloid include the radioscaphocapitate (RSC) ligament, the long radiolunate (LRL) ligament, and the radial collateral ligament. The RSC ligament, originating from the radial styloid and traversing to the scaphoid and capitate, acts as a primary stabilizer against carpal supination and volar displacement. The LRL ligament originates more proximally on the radius and extends to the lunate, contributing to lunate stability. The radial collateral ligament extends from the radial styloid to the scaphoid and trapezium, resisting ulnar deviation. Damage to these structures during a radial styloid fracture can significantly compromise carpal stability and subsequent functional outcomes. The superficial radial nerve courses distally over the radial styloid, requiring careful protection during surgical approaches.
Biomechanical Considerations
The distal radius plays a critical role in load transmission across the wrist. Approximately 80% of axial load is transmitted through the radiocarpal joint, with the remaining 20% passing through the ulnocarpal joint. The radial styloid, specifically its articulation with the scaphoid, is a major contributor to this load-bearing capacity. Anatomical restoration of the radial styloid fragment is essential for maintaining the normal biomechanics of the wrist, which include:
- Radial Height: The difference in length between the radial styloid and the ulnar head (normal 9-12 mm). Loss of radial height can lead to ulnar positive variance, increased load on the ulnar side, and potential ulnocarpal impingement.
- Radial Inclination: The angle formed by a line connecting the radial styloid tip to the ulnar corner of the lunate facet, and a line perpendicular to the long axis of the radius (normal 21-25 degrees). Loss of radial inclination can alter carpal kinematics and restrict wrist range of motion.
- Volar Tilt: The angle between the articular surface of the distal radius and a line perpendicular to the long axis of the radius (normal 11-12 degrees volarly). While radial styloid fractures primarily affect the coronal plane, significant displacement can secondarily impact volar tilt.
Disruption of the articular surface by a radial styloid fracture, especially with articular step-off or gap, directly impacts the smooth gliding motion of the scaphoid, predisposing the joint to post-traumatic osteoarthritis. Furthermore, the strong association with scapholunate ligament injuries highlights the interconnectedness of carpal stability. A compromised SLIL can lead to scapholunate dissociation (SLD), resulting in a dorsal intercalated segmental instability (DISI) pattern and progressive carpal collapse. Therefore, accurate reduction and stable fixation of the radial styloid, coupled with a thorough assessment and potential treatment of associated ligamentous injuries, are paramount to preserving long-term wrist function.
Indications and Contraindications
The decision to pursue operative versus non-operative management for radial styloid fractures is based on a comprehensive assessment of fracture characteristics, patient factors, and the presence of associated injuries. The goal of treatment is always to restore wrist anatomy and function, thereby minimizing the risk of complications such as post-traumatic arthritis or chronic instability.
Operative Indications
Operative intervention is generally indicated for displaced or unstable radial styloid fractures, particularly those with articular incongruity. Arthroscopic assistance significantly enhances the ability to meet these surgical goals.
- Articular Step-off or Gap: An intra-articular step-off or gap of greater than 1-2 mm is a strong indication for surgical fixation, as it correlates with increased risk of post-traumatic arthritis. Arthroscopy allows for precise visualization and reduction of these articular imperfections.
- Displacement of the Radial Styloid Fragment: Displaced fractures where the radial styloid fragment is translated, angulated, or rotated relative to the radial shaft.
- Significant Radial Shortening: Loss of radial height compared to the contralateral wrist or significant shortening (>2 mm).
- Loss of Radial Inclination: Reduction of the normal radial inclination angle (<20 degrees).
- Associated Carpal Instability: This is a critical indication for arthroscopic evaluation. The high incidence of associated scapholunate interosseous ligament tears necessitates direct visualization and, if unstable, potential repair or stabilization. Other carpal ligament injuries (e.g., lunotriquetral, radioscaphocapitate) can also influence the decision for operative management.
- Open Fractures: Require immediate surgical debridement and stabilization.
- Polytrauma Patients: May benefit from early definitive fixation to facilitate mobilization and overall rehabilitation.
- Isolated Radial Styloid Fractures: These are particularly well-suited for arthroscopic management due to the clear visualization of the single major articular fragment, making it an ideal fracture pattern for surgeons gaining experience with arthroscope-assisted fixation.
Non-Operative Indications
Non-operative management typically involves closed reduction and cast immobilization. This approach is reserved for specific fracture patterns.
- Nondisplaced or Minimally Displaced Fractures: Articular step-off or gap less than 1 mm, without significant displacement, shortening, or angular deformity.
- Stable Fracture Pattern: Fractures that remain stable after reduction and do not show signs of re-displacement during follow-up radiographs.
- Absence of Associated Carpal Instability: No evidence of scapholunate dissociation or other significant ligamentous injuries.
- Patient Comorbidities: In patients with significant medical comorbidities that preclude safe surgical intervention, non-operative management may be considered even for displaced fractures, accepting a potentially less ideal anatomical outcome.
- Low Functional Demand: Patients with very low functional demands on the wrist.
Contraindications
Absolute contraindications for arthroscopic management of radial styloid fractures are rare but include:
- Severe Comminution: Extensive comminution of the radial styloid fragment that precludes stable fixation with screws.
- Gross Contamination or Established Infection: Acute infection around the wrist joint.
- Severe Soft Tissue Compromise: Extensive open wounds or severe crush injuries where additional portals might compromise soft tissue viability.
- Uncontrolled Coagulopathy: Risk of significant bleeding during arthroscopy.
- Patient Inability to Tolerate Anesthesia: Severe medical conditions.
| Indication Category | Operative Indications | Non-Operative Indications |
|---|---|---|
| Fracture Displacement | Articular step-off >1-2 mm, significant fragment displacement | Articular step-off <1 mm, nondisplaced |
| Radial Parameters | Radial shortening >2 mm, loss of radial inclination | Normal radial length, inclination, and volar tilt |
| Associated Injuries | Scapholunate ligament injury (unstable), other carpal instability | No significant carpal ligamentous injury |
| Fracture Type | Isolated radial styloid fracture (ideal for arthroscopy) | Stable fracture pattern after closed reduction |
| Open Fractures | All open fractures | N/A |
| Patient Factors | High functional demand, ability to tolerate surgery | Significant comorbidities, low functional demand |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is crucial for successful arthroscopic management of radial styloid fractures, ensuring efficient execution and minimizing potential complications.
Diagnostic Imaging
- Standard Radiographs: Anteroposterior (AP), lateral, and oblique views of the wrist are the initial imaging modalities. These provide basic information on fracture pattern, displacement, and articular involvement. A contralateral wrist series can be helpful for assessing normal radial height and inclination.
- Computed Tomography (CT) Scan: A fine-cut CT scan is essential for detailed assessment of the fracture. It accurately delineates the articular step-off or gap, fragment size, degree of comminution, and the relationship of the radial styloid fragment to the rest of the distal radius. Three-dimensional (3D) reconstructions can further aid in surgical planning by visualizing complex fragment rotation.
- Magnetic Resonance Imaging (MRI): While not routinely required for radial styloid fractures, an MRI may be considered if there is strong clinical suspicion of significant soft tissue injuries beyond the scope of arthroscopic visualization, such as complete extrinsic ligament tears or intrinsic carpal ligament avulsions that may not be fully addressed by standard arthroscopy. However, many associated ligamentous injuries, especially SLIL tears, are readily identified and managed intra-arthroscopically.
Surgical Setup and Anesthesia
The procedure is typically performed under regional anesthesia (e.g., supraclavicular or axillary block) combined with light sedation or general anesthesia, based on patient preference and surgeon judgment. A pneumatic tourniquet is applied to the upper arm to maintain a bloodless field, typically inflated to 250-300 mmHg.
The operating room should be set up to facilitate both arthroscopic and open techniques if conversion becomes necessary. A standard wrist arthroscopy tower with camera, light source, pump, and shaver is required. A C-arm fluoroscopy unit is positioned to allow for AP, lateral, and oblique views without repositioning the patient or the arm. Instrumentation should include small fragment cannulated screw sets (2.4mm to 3.5mm), guidewires, a wire driver, a standard arthroscopy set (2.7mm or 2.9mm 30-degree scope), a blunt trocar, and appropriate hand surgical instruments.
Patient Positioning
The patient is positioned supine on the operating table. The affected arm is prepared and draped in a sterile fashion up to the mid-humerus. A standard hand table is used to support the arm. The wrist is suspended using finger traps attached to a traction tower, applying 10-15 pounds of traction. This distraction of the radiocarpal joint is critical for improving visualization during arthroscopy by creating space within the joint and reducing impaction of fracture fragments. The traction tower should allow for adjustments in forearm rotation (pronation/supination) and wrist position (flexion/extension, radial/ulnar deviation) as needed during the procedure. Typically, the forearm is pronated to facilitate access to dorsal portals and the wrist is in slight flexion.
Portal Placement
Careful planning and creation of arthroscopic portals are essential to prevent iatrogenic neurovascular injury. Standard dorsal portals are utilized for radial styloid fracture management:
- 3/4 Portal: Located between the third and fourth extensor compartments. This is typically the primary viewing portal for initial inspection and for instruments during reduction. The arthroscope is inserted in the dorsal 3/4 portal to clear the joint of debris and hematoma.
- 4/5 Portal: Located between the fourth and fifth extensor compartments. This portal is often used as a working portal for instruments or as an alternative viewing portal to assess reduction and rotation effectively.
- 6R Portal: Located radial to the extensor carpi ulnaris (ECU) tendon, between the sixth and fifth extensor compartments. This portal is particularly useful for viewing the radial styloid fragment from a more ulnar perspective, which is crucial for judging rotation and reduction.
- 1/2 Portal: Located between the first and second extensor compartments, radial to the extensor pollicis longus (EPL) tendon. This portal can be used as an outflow portal, or occasionally for instrumentation for specific radial-sided issues.
- Midcarpal Portals: While not always required for isolated radial styloid fractures, midcarpal portals (e.g., midcarpal radial) may be established if extensive carpal ligament assessment or repair is anticipated.
Portal placement begins with palpation of anatomical landmarks and extensor tendons. Skin incisions are typically 3-5 mm. Blunt dissection is performed down to the joint capsule using a mosquito hemostat to create a safe path, preventing damage to the dorsal sensory branches of the radial and ulnar nerves, which are particularly vulnerable in the vicinity of the portals. The joint capsule is then carefully incised, and a blunt trocar is inserted into the joint to prevent chondral damage.
Detailed Surgical Approach and Technique
The arthroscopic management of radial styloid fractures offers a precise method for achieving anatomical reduction and stable internal fixation, while simultaneously allowing for the evaluation and treatment of associated intra-articular pathologies.
Initial Joint Assessment and Debridement
With the wrist suspended in traction and appropriate portals established, the arthroscope is initially inserted through the dorsal 3/4 portal. The joint is thoroughly irrigated to clear any debris, hematoma, or synovial inflammation, which can impair visualization. A motorized shaver, inserted through a working portal (e.g., 4/5 or 6R), is used for debridement.
The initial inspection focuses on:
1. Articular Surface of the Radial Styloid: Assessing the fracture pattern, the degree of displacement, and the size of the fragment.
2. Scapholunate Interosseous Ligament (SLIL): This is a critical step, as radial styloid fractures have a high incidence of associated SLIL tears. The SLIL is best assessed arthroscopically by direct visualization and probing. Dynamic evaluation with a probe can identify laxity or complete tears. Instability can be further assessed by viewing the scaphoid-lunate interval and attempting to reduce any scaphoid malrotation.
3. Lunotriquetral Interosseous Ligament (LTIL): Though less commonly associated than SLIL tears, the LTIL should also be inspected.
4. Cartilage Status: Evaluation of the radiocarpal articular cartilage for any pre-existing degeneration or acute chondral injuries secondary to the trauma.
5. Extrinsic Ligaments: Inspection of the extrinsic ligaments, such as the radioscaphocapitate, long radiolunate, and radial collateral ligaments, for avulsions or tears.
This comprehensive initial assessment dictates the full scope of the surgical intervention beyond just fracture reduction.
Guidewire Placement for Reduction
Following the initial assessment, attention shifts to the radial styloid fragment. One or two cannulated guidewires are inserted percutaneously into the radial styloid fragment. It is crucial at this stage that these guidewires do not cross the fracture site. The guidewires are advanced into the fragment using a wire driver in oscillation mode. This mode generates less heat compared to continuous drilling, reducing the risk of thermal necrosis to bone and surrounding soft tissues.
Fluoroscopic evaluation is performed to ensure the guidewires are centrally positioned within the radial styloid fragment, providing optimal purchase for manipulation. These wires will serve as "joysticks" for controlled reduction.
Arthroscopic Guided Reduction
For optimal visualization of the reduction, the arthroscope is often transferred to a more ulnar portal, such as the 6R or 4/5 portal. This vantage point allows for a broad view across the radiocarpal joint, facilitating effective judgment of the radial styloid fragment's rotation and reduction relative to the main radial shaft.
Using the previously placed guidewires as joysticks, the radial styloid fragment is meticulously manipulated. The goal is to achieve an anatomical reduction, restoring articular congruity, radial length, and inclination. This manipulation is performed under direct arthroscopic observation, which is the key advantage of this technique. The arthroscopic view allows the surgeon to detect subtle rotational deformities or articular step-offs that may appear perfectly reduced on fluoroscopy but are still incongruent. This discrepancy highlights the critical role of arthroscopy in achieving true anatomical reduction.
In some cases, a blunt trocar can be inserted through another working portal, such as the 3/4 portal, to assist with reduction. The trocar acts as an internal lever or pusher, aiding in the precise alignment and seating of the fragment.

Figure 1A: Arthroscopic view demonstrating the use of a blunt trocar through the 3/4 portal to aid in the reduction of a displaced radial styloid fragment.

Figure 1B: Arthroscopic visualization of the radial styloid fragment being manipulated into anatomical alignment, with concurrent assessment of articular congruity.
Provisional Fixation and Verification
Once the fracture is judged to be absolutely anatomic under direct arthroscopic visualization, the guidewires are then carefully advanced across the fracture site into the radius shaft. This provides provisional fixation, holding the reduction in place.
The provisional fixation and the anatomical reduction are then meticulously evaluated under fluoroscopy. AP, lateral, and oblique views are obtained to confirm the restoration of radial length, inclination, and volar tilt, and to ensure that the guidewires are in optimal position within the radius shaft without impinging on the joint or causing iatrogenic injury.

Figure 1C: Fluoroscopic image showing guidewires advanced across the anatomically reduced radial styloid fracture into the radial shaft, providing provisional fixation.
Definitive Fixation with Cannulated Screws
While guidewires alone can provide stabilization, cannulated screws are the recommended definitive fixation method. Cannulated screws offer superior compressive strength and rotational stability compared to K-wires. Moreover, they significantly decrease the risk of soft tissue irritation and potential pin track infection, which are common complications associated with K-wire fixation, particularly if left protruding through the skin.
Using the provisional guidewires as guides, appropriate length cannulated screws are selected. These can be either fully threaded headless screws (for subchondral compression) or partially threaded headed screws. The screw length is typically measured from the guidewire using a depth gauge. A cannulated drill bit can be used over the guidewire if necessary, followed by cannulated tapping if dictated by bone density or screw system recommendations. The cannulated screws are then carefully inserted over the guidewires, ensuring optimal compression across the fracture site without over-compression that might lead to comminution, and without intra-articular penetration.
Post-fixation, arthroscopic inspection is again performed to confirm that no screw threads or tips are intra-articular and that the articular surface remains perfectly congruent. Fluoroscopy is also repeated to confirm final screw position and fracture reduction.

Figure 1D: Post-fixation arthroscopic view confirming anatomical reduction and intra-articular hardware integrity, showing the inserted cannulated screw.

Figure 1E: Final fluoroscopic image demonstrating stable internal fixation of the radial styloid fracture with cannulated screws, confirming precise reduction and hardware placement.
Ligamentous Repair or Stabilization
If significant scapholunate or other carpal ligamentous injuries were identified during the initial assessment and deemed unstable, appropriate intervention is undertaken at this stage. For an acute, repairable SLIL tear, direct repair, capsulodesis, or K-wire stabilization across the scaphoid and lunate may be performed. The choice of technique depends on the tear pattern, chronicity, and surgeon preference. The arthroscopic environment provides an excellent platform for these concurrent procedures.
Wound Closure
Following definitive fixation and any necessary ligamentous work, the arthroscopy fluid is allowed to drain. The portals are closed with a single skin stitch (e.g., 4-0 nylon) or sterile adhesive strips. A sterile dressing is applied, and a well-padded splint (e.g., sugar tong or volar forearm splint) is used to immobilize the wrist in a position of comfort and stability.
Complications and Management
Despite the precision offered by arthroscopic techniques, radial styloid fracture management can be associated with a range of complications, requiring careful monitoring and appropriate intervention.
General Complications of Distal Radius Fixation
- Malunion/Nonunion: Inadequate reduction or unstable fixation can lead to malunion (healing in a deformed position) or, less commonly, nonunion (failure to heal). Malunion, particularly articular step-off, is a primary cause of post-traumatic arthritis. Salvage: Revision open reduction and internal fixation, corrective osteotomy, or in severe cases, partial or total wrist arthrodesis.
- Post-Traumatic Arthritis: The most common long-term complication, especially with residual articular incongruity or unaddressed associated ligamentous injuries (e.g., SLAC wrist from SLIL tear). Salvage: Activity modification, NSAIDs, corticosteroid injections, eventually wrist fusion or arthroplasty for debilitating symptoms.
- Hardware Irritation/Prominence: Screws can sometimes irritate tendons or overlying soft tissues, particularly if not countersunk adequately or if they protrude. Salvage: Elective hardware removal after fracture healing.
- Tendon Rupture/Attrition: Rare, but can occur with prominent hardware or chronic irritation. Salvage: Tendon repair or reconstruction.
- Pin Tract Infection (if K-wires used): A significant risk with K-wire fixation, necessitating meticulous pin care. Less common with fully internalized cannulated screws. Salvage: Oral antibiotics for superficial infections, K-wire removal and debridement for deep infections.
- Nerve Injury:
- Superficial Radial Nerve Neuroma: Can occur from direct trauma, traction, or iatrogenic injury during exposure.
- Median Nerve (Carpal Tunnel Syndrome): Can be pre-existing, or develop acutely due to hematoma/edema, or chronically due to malunion or inflammation. Salvage: Acute carpal tunnel release for impending ischemia, elective release for chronic symptoms.
- Dorsal Sensory Ulnar Nerve: Vulnerable during medial portal placement. Salvage: Neurolysis, local anesthetic injections.
- Complex Regional Pain Syndrome (CRPS) Type 1: A severe pain syndrome characterized by disproportionate pain, swelling, stiffness, and autonomic dysfunction. Salvage: Multidisciplinary approach involving physical therapy, pain management, stellate ganglion blocks, medications (e.g., gabapentin, bisphosphonates).
- Stiffness: Common after wrist trauma and immobilization. Salvage: Intensive physical therapy, dynamic splinting, manipulation under anesthesia, capsulectomy.
Arthroscopy-Specific Complications
- Iatrogenic Chondral Damage: Injury to articular cartilage from instruments, scope, or excessive traction. Incidence is generally low with careful technique. Salvage: Microfracture, chondroplasty if symptomatic.
- Fluid Extravasation: Accumulation of irrigation fluid in the soft tissues, potentially leading to compartment syndrome. Rare in the wrist but a known risk in arthroscopy. Maintaining appropriate pump pressure and limiting operative time are important. Salvage: Close monitoring, fasciotomy if compartment syndrome develops.
- Portal Site Infection: Low incidence, typically superficial. Salvage: Oral antibiotics, local wound care.
- Neurovascular Injury at Portals: Damage to superficial radial nerve, dorsal sensory ulnar nerve, or radial artery branches during portal creation. Careful blunt dissection and knowledge of anatomy minimize this risk. Salvage: Direct repair of nerve, neurolysis, or observation depending on severity.
| Complication | Incidence (General) | Salvage Strategies |
|---|---|---|
| Malunion/Nonunion | 5-15% | Revision ORIF, corrective osteotomy, partial/total wrist arthrodesis |
| Post-Traumatic Arthritis | 10-30% (depending on articularity) | NSAIDs, injections, activity modification, wrist fusion, arthroplasty |
| Hardware Irritation/Prominence | 5-10% | Elective hardware removal |
| Pin Tract Infection (K-wires) | 5-10% | Oral antibiotics, pin removal, debridement |
| Nerve Injury (SRN, Median, DSUN) | <5% (variable by nerve) | Neurolysis, carpal tunnel release, observation, nerve repair |
| CRPS Type 1 | 2-5% | Multidisciplinary pain management, PT, stellate ganglion blocks, medications |
| Stiffness | 10-20% | Intensive PT, dynamic splinting, manipulation under anesthesia, capsulectomy |
| Iatrogenic Chondral Damage | <1% | Microfracture, chondroplasty |
| Fluid Extravasation | Rare (compartment syndrome) | Close monitoring, fasciotomy |
Post Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is essential to optimize functional recovery, restore range of motion, and prevent stiffness after arthroscopic fixation of radial styloid fractures. The protocol must be tailored to the individual patient, fracture stability, and any associated ligamentous repairs.
Immediate Postoperative Phase (0-2 Weeks)
- Immobilization: The wrist is typically immobilized in a well-padded sugar tong splint or volar forearm splint for 1-2 weeks. This provides protection while allowing for some forearm pronation/supination. If significant carpal ligamentous repair (e.g., SLIL) was performed, a longer period of rigid cast immobilization (e.g., 4-6 weeks) may be indicated.
- Elevation and Ice: Consistent elevation of the hand above heart level and regular application of ice packs are crucial to minimize swelling and pain.
- Pain Management: Prescribe appropriate analgesics, including NSAIDs and opioids as needed, and consider regional nerve blocks.
- Digital Range of Motion: Patients are strongly encouraged to actively move their fingers and thumb throughout the day to prevent stiffness and maintain circulation.
- Shoulder and Elbow Range of Motion: Active range of motion exercises for the shoulder and elbow are initiated immediately to prevent stiffness in these joints.
- Wound Care: Maintain clean and dry dressings. Monitor portal sites for signs of infection. Suture removal typically occurs at 10-14 days.
Early Mobilization Phase (2-6 Weeks)
- Splint/Cast Removal: The splint is typically removed at 2-3 weeks, or as dictated by fracture stability and soft tissue healing. If a cast was used for ligamentous repair, it is removed at 4-6 weeks.
- Gentle Wrist Range of Motion: Under guidance from a hand therapist, initiate gentle active and passive range of motion exercises for the wrist.
- Flexion/Extension: Gravity-assisted exercises, gentle stretches.
- Radial/Ulnar Deviation: Small, controlled movements.
- Forearm Pronation/Supination: Continued emphasis on restoring full rotation.
- Early Strengthening (Isometric): Isometric exercises for wrist and forearm musculature may be introduced cautiously, without resistance.
- Scar Management: Begin scar massage and desensitization around portal sites once incisions are healed.
- Edema Control: Continue with elevation, compression garments, and retrograde massage to manage residual swelling.
Strengthening and Return to Activity Phase (6-12+ Weeks)
- Progressive Strengthening: Gradually advance strengthening exercises using light resistance bands, therapy putty, and light weights. Focus on grip strength, wrist flexion/extension, and forearm rotation.
- Proprioceptive Exercises: Introduce activities to improve wrist stability and proprioception, such as weight-bearing on the hand, balance board exercises.
- Functional Activities: Incorporate exercises that mimic daily living activities and work-specific tasks.
- Return to Activity: Gradual return to light recreational activities and work-related duties. High-impact or heavy resistance activities should be deferred until 3-4 months postoperatively, pending radiographic evidence of healing and robust clinical stability.
- Long-Term Monitoring: Patients should be monitored for signs of persistent pain, stiffness, or early arthritic changes.
The success of rehabilitation relies on close collaboration between the surgeon, hand therapist, and patient. Patient education regarding the importance of adherence to the protocol and activity modifications is crucial. Any signs of complications, such as increased pain, swelling, or neurological symptoms, warrant immediate reassessment.
Summary of Key Literature and Guidelines
The paradigm of managing intra-articular distal radius fractures, including radial styloid fractures, has significantly evolved with the advent and refinement of arthroscopic techniques. A substantial body of literature now supports the advantages of arthroscopically assisted reduction and internal fixation (ARIF) over traditional fluoroscopically guided techniques alone.
Key findings and consensus points from the literature include:
- Superior Articular Reduction: Numerous studies and meta-analyses consistently demonstrate that arthroscopic visualization allows for more precise anatomical reduction of intra-articular fragments, minimizing residual articular step-off and gap. This direct visualization helps identify and correct subtle fragment rotation that is often missed on fluoroscopy, a critical factor in mitigating the risk of post-traumatic arthritis. While fluoroscopy remains essential for overall alignment and hardware placement, arthroscopy provides the ultimate intra-articular truth.
- Comprehensive Ligamentous Assessment: A compelling advantage of wrist arthroscopy in the setting of distal radius fractures is the ability to thoroughly evaluate associated carpal ligamentous injuries. Radial styloid fractures, in particular, have a well-documented high incidence of scapholunate interosseous ligament (SLIL) tears. Arthroscopy allows for direct visualization, probing, and dynamic assessment of these ligaments. Identifying and addressing significant, unstable SLIL injuries concurrently can prevent the long-term sequelae of carpal instability, such as scapholunate advanced collapse (SLAC) wrist.
- Improved Outcomes for Associated Injuries: When concomitant ligamentous injuries are identified and treated appropriately (e.g., K-wire stabilization, direct repair, capsulodesis), arthroscopy is associated with improved long-term functional outcomes compared to cases where these injuries are missed or untreated.
- Learning Curve and Surgeon Experience: While ARIF offers significant benefits, it is acknowledged that there is a learning curve associated with wrist arthroscopy and arthroscopically assisted fracture fixation. Isolated radial styloid fractures are often cited as an ideal starting point for surgeons gaining experience, as they involve a single, relatively large fragment and the goals of reduction are clear. Proficiency in basic wrist arthroscopy and fracture management principles is a prerequisite.
- Fixation Principles: The literature generally advocates for stable internal fixation with cannulated screws for radial styloid fractures, particularly over K-wires alone for definitive fixation. Cannulated screws provide better compression and stability, while minimizing soft tissue irritation and reducing the risk of pin track infection compared to exposed K-wires.
- Acceptable Reduction Parameters: Current guidelines generally consider an articular step-off or gap of greater than 1-2 mm to be an indication for operative intervention due to the increased risk of post-traumatic arthritis. Arthroscopy provides the means to consistently achieve less than 1 mm of residual articular incongruity. Restoration of radial length, radial inclination, and volar tilt are also critical radiological parameters for successful outcomes.
- Evidence for Specific Patient Groups: Studies have shown that ARIF can be particularly beneficial in younger, active patients with displaced intra-articular fractures, where restoration of precise anatomy is paramount for returning to high-demand activities.
In summary, the academic consensus supports arthroscopic assistance for the management of radial styloid fractures as a highly effective method to achieve anatomical reduction and simultaneously manage associated intra-articular soft tissue injuries. For orthopedic surgeons, this technique represents a valuable tool in the armamentarium for optimizing outcomes in this specific fracture pattern, especially given its role in preventing degenerative changes and maintaining long-term wrist function.
You Might Also Like