Effective K-Wire Fixation for Distal Radius Fractures Without External Fixation
Key Takeaway
This topic focuses on Effective K-Wire Fixation for Distal Radius Fractures Without External Fixation, K-wire fixation without external fixation kwire is suitable for unstable intra-articular or extra-articular distal radius fractures with mild comminution and no osteoporosis. This minimally invasive technique uses percutaneous pins to aid reduction and stabilize fragments. It supports the subchondral area and maintains articular reduction, particularly in cases that do not require additional external support for alignment.
Introduction and Epidemiology
Distal radius fractures represent one of the most frequently encountered osseous injuries in orthopedic practice, accounting for approximately one-fifth of all fractures evaluated in emergency departments. The distribution of these injuries demonstrates a classic bimodal demographic pattern. In the younger demographic, these fractures typically result from high-energy trauma, such as motor vehicle collisions or sports-related injuries, often presenting with significant comminution and articular displacement. Conversely, in the elderly population, particularly postmenopausal women, these fractures are predominantly fragility fractures resulting from low-energy falls from a standing height onto an outstretched hand.
The fundamental mechanism of injury involves an axial load applied to the carpus, which is subsequently transmitted to the distal radius. The position of the wrist at the time of impact dictates the fracture pattern. Wrist extension typically produces a dorsal bending moment, resulting in the classic Colles-type fracture with dorsal angulation and displacement. Wrist flexion generates a volar bending moment, yielding a Smith-type fracture. The energy of the injury, combined with the intrinsic bone mineral density of the patient, determines the degree of metaphyseal comminution and intra-articular extension.
Historically, closed reduction and cast immobilization served as the mainstay of treatment. However, the recognition of functional deficits associated with malunion prompted a shift toward operative intervention. Percutaneous Kirschner wire (K-wire) fixation, utilized without the augmentation of an external fixator, remains a cornerstone in the armamentarium of the orthopedic surgeon. This technique offers a minimally invasive means to stabilize the fracture fragments, acting as a direct internal splint or leveraging the intact cortical hinges. While the advent of volar locking plates has revolutionized the management of complex, comminuted, and osteoporotic fractures, isolated K-wire fixation remains highly effective and economically advantageous for specific fracture patterns, particularly extra-articular fractures with adequate bone stock, simple intra-articular split fractures, and pediatric physeal injuries where growth plate preservation is paramount.
Surgical Anatomy and Biomechanics
A profound understanding of the osseous, ligamentous, and neurovascular anatomy of the distal radius is critical for executing percutaneous pinning safely and effectively. The distal radius is not merely a structural column; it is a complex articular platform that dictates radiocarpal and distal radioulnar joint kinematics.
Osseous Anatomy
The distal radius expands from the diaphyseal shaft into a broad metaphyseal flare, terminating in three distinct articular facets: the scaphoid fossa, the lunate fossa, and the sigmoid notch. The scaphoid and lunate fossae articulate with the proximal carpal row, while the sigmoid notch articulates with the ulnar head to form the distal radioulnar joint.
Normal radiographic parameters of the distal radius are essential benchmarks for reduction. The articular surface exhibits a radial inclination averaging 22 degrees and a volar tilt averaging 11 degrees. Radial height, measured from the tip of the radial styloid to the ulnar articular surface, typically measures 11 to 12 millimeters. Ulnar variance, the relative length of the distal radius to the distal ulna, should ideally be neutral. Biomechanically, the distal radius absorbs approximately 80% of the axial load transmitted across the wrist joint, with the remaining 20% borne by the triangular fibrocartilage complex and the distal ulna. Loss of volar tilt or radial shortening alters this load distribution exponentially, predisposing the patient to radiocarpal arthrosis and ulnocarpal impaction syndrome.

Ligamentous Anatomy and Ligamentotaxis
The concept of ligamentotaxis is foundational to the closed reduction of distal radius fractures. Longitudinal traction applied to the carpus places the extrinsic radiocarpal ligaments under tension, which in turn realigns the attached osseous fracture fragments.
The volar radiocarpal ligaments are stout and provide primary stability to the wrist. These include the radioscaphocapitate, long radiolunate, and short radiolunate ligaments. The dorsal radiocarpal ligaments, including the dorsal intercarpal and radiocarpal ligaments, are comparatively thinner but play a crucial role in preventing dorsal carpal subluxation. When applying traction during closed reduction, the tension generated through these volar and dorsal capsuloligamentous structures aids in restoring radial length and pulling the articular fragments into alignment.

Neuromuscular and Tendinous Anatomy
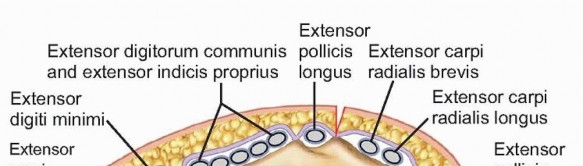
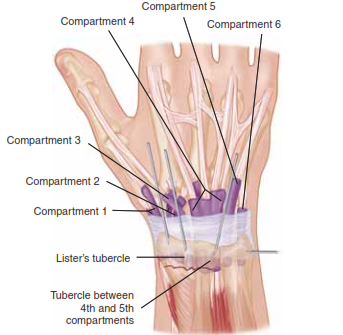
The dorsal aspect of the distal radius is organized into six distinct extensor compartments, defined by the extensor retinaculum.
1. First compartment: Abductor pollicis longus and extensor pollicis brevis.
2. Second compartment: Extensor carpi radialis longus and extensor carpi radialis brevis.
3. Third compartment: Extensor pollicis longus, which routes around Lister’s tubercle.
4. Fourth compartment: Extensor digitorum communis and extensor indicis proprius.
5. Fifth compartment: Extensor digiti minimi.
6. Sixth compartment: Extensor carpi ulnaris.
Between the first and second dorsal compartments lies a critical "bare spot" on the radial styloid, which serves as the optimal entry point for radial styloid K-wires.
The neurovascular anatomy dictates the safe zones for percutaneous pinning. The superficial branch of the radial nerve emerges from beneath the brachioradialis muscle belly in the distal third of the forearm, transitioning from a subfascial to a subcutaneous position. It courses directly over the first dorsal compartment and branches extensively to provide sensation to the dorsal radial aspect of the hand. The terminal branches of the lateral antebrachial cutaneous nerve also lie superficial to the forearm fascia at the radial wrist. These neural structures are highly susceptible to iatrogenic injury during percutaneous pin insertion, necessitating meticulous blunt dissection down to the osseous surface prior to wire advancement.
Indications and Contraindications
The decision to proceed with isolated K-wire fixation without external fixation hinges on fracture morphology, bone quality, and patient-specific factors. Percutaneous pinning relies on the intrinsic stability of the bone once reduced; it does not provide rigid internal fixation. Therefore, it is best suited for fractures where cortical contact can be restored and maintained with simple wire stabilization.
In pediatric populations, smooth K-wires are the gold standard for displaced physeal fractures (Salter-Harris II) that are unstable post-reduction, as they can cross the physis without causing premature growth arrest. In adults, percutaneous pins (typically 0.062-inch or 0.045-inch) are indicated for extra-articular fractures with reducible metaphyseal comminution and simple intra-articular fractures (e.g., radial styloid split) in patients with normal bone mineral density.
Contraindications to isolated K-wire fixation include severe osteoporosis, where the metaphyseal bone is too cavernous to provide purchase for the wires, leading to inevitable loss of reduction. Highly comminuted intra-articular fractures, volar shear fractures (Barton's fractures), and fractures with massive metaphyseal defects lacking cortical contact also contraindicate isolated pinning, as the K-wires cannot resist the deforming forces of the forearm musculature. In these scenarios, volar locking plates or external fixators are mandated.
| Parameter | Operative K-Wire Fixation | Non-Operative or Alternative Fixation |
|---|---|---|
| Fracture Pattern | Extra-articular, simple intra-articular split, reducible | Volar shear (requires plate), severe articular comminution (requires plate/ex-fix) |
| Bone Quality | Normal bone mineral density | Severe osteoporosis (high risk of wire cut-out) |
| Metaphyseal Defect | Minimal to moderate, cortical apposition achievable | Massive defect, lack of volar cortical buttress |
| Pediatric Considerations | Unstable Salter-Harris II physeal fractures | Stable, non-displaced fractures (cast immobilization) |
| Patient Profile | Low to moderate functional demands, adequate soft tissue | High-demand athletes (may prefer rigid plate for early ROM), severe soft tissue compromise |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning begins with high-quality orthogonal radiographs of the wrist, including posteroanterior, lateral, and oblique views. These images allow the surgeon to assess the degree of comminution, the direction of displacement, and the specific fracture lines. For fractures with suspected intra-articular extension, a non-contrast computed tomography scan is highly recommended to delineate the articular step-off, gap formation, and the exact geometry of the fragments, particularly the lunate facet and the sigmoid notch.

Templating is performed to determine the optimal trajectory of the K-wires. The surgeon must select the appropriate wire diameter; 0.062-inch (1.6 mm) wires provide robust stability for adult metaphyseal fixation, while 0.045-inch (1.1 mm) wires are frequently utilized for smaller fragments or in pediatric patients. The necessary equipment, including a wire driver, wire cutter, wire bender, and a mini C-arm fluoroscopy unit, must be confirmed prior to induction.
The procedure can be performed under regional anesthesia (supraclavicular or axillary brachial plexus block) or general anesthesia, depending on patient comorbidities and anesthesiologist preference. The patient is positioned supine on the operating table with the affected extremity extended onto a radiolucent hand table. A pneumatic tourniquet is placed on the proximal arm but is often not inflated for percutaneous procedures unless an open reduction becomes necessary. The mini C-arm is brought in perpendicular to the hand table, allowing for seamless transition between posteroanterior and lateral fluoroscopic views by simply rotating the patient's forearm, thereby minimizing movement of the imaging equipment.
Detailed Surgical Approach and Technique
The execution of percutaneous K-wire fixation requires a meticulous blend of closed reduction maneuvers, precise fluoroscopic interpretation, and rigorous protection of the soft tissue envelope. The objective is to restore anatomic alignment and stabilize the fracture with the minimal necessary hardware.
Closed Reduction Maneuvers
The procedure commences with closed reduction. The surgeon applies sustained longitudinal traction to the digits (frequently utilizing finger traps) with counter-traction applied to the proximal forearm. This traction exploits the principle of ligamentotaxis, pulling the distal fragments out of their impacted, shortened position.
Once length is restored, the surgeon manipulates the distal fragment to correct angulation. For a classic dorsally displaced fracture, the surgeon places their thumbs on the dorsal aspect of the distal fragment and their index fingers on the volar aspect of the proximal radial shaft. A volar-directed force is applied to the distal fragment while simultaneously flexing and ulnarly deviating the wrist. The reduction is immediately verified under orthogonal fluoroscopy. Restoration of volar tilt, radial inclination, and radial height must be confirmed before proceeding to fixation.

Percutaneous Pinning Techniques
Several pinning configurations exist, and the choice depends on the fracture morphology. The most common techniques include radial styloid pinning, crossed pinning, and Kapandji intrafocal pinning.
Radial Styloid Pinning
This technique stabilizes the radial column. To avoid injury to the superficial branch of the radial nerve, a true percutaneous approach (driving the wire directly through the skin) is strongly discouraged. Instead, a 1- to 2-centimeter longitudinal incision is made over the "bare spot" between the first and second dorsal compartments at the radial styloid. Blunt dissection is performed using a mosquito hemostat down to the periosteum, spreading parallel to the nerve fibers.
A tissue protector or drill sleeve is inserted to the bone to shield the soft tissues. A 0.062-inch K-wire is introduced at the tip of the radial styloid and driven proximally, ulnarly, and dorsally across the fracture site to engage the intact opposite cortex of the radial diaphysis. The trajectory must be verified on both PA and lateral fluoroscopic views to ensure it does not penetrate the radiocarpal or distal radioulnar joints.

Crossed Pinning Configuration
To enhance rotational stability and resist dorsal displacement, a second wire is often placed from the dorsoulnar aspect of the distal radius. The entry point is typically between the fourth and fifth dorsal compartments. Similar blunt dissection is performed to protect the extensor tendons. The wire is driven proximally and radially, crossing the first wire proximal to the fracture site. The divergence of the wires within the proximal fragment maximizes the biomechanical stability of the construct. Care must be taken to ensure the dorsoulnar wire does not tether the extensor digitorum communis or extensor digiti minimi tendons.
Kapandji Intrafocal Pinning
The Kapandji technique utilizes K-wires not as transfixion pins, but as intrafocal levers and buttresses. This is particularly useful for dorsally displaced extra-articular fractures.
Following closed reduction, a K-wire is introduced directly into the fracture hematoma from the dorsal aspect. The wire is driven volar-ward until it contacts the intact volar cortex of the proximal fragment. The wire is then levered distally, physically pushing the dorsal cortex of the distal fragment into a reduced position and restoring volar tilt. Once the reduction is achieved, the wire is driven through the volar cortex to lock it in place. A second wire is often placed from the radial aspect into the fracture site and levered to restore radial inclination. This technique relies heavily on the integrity of the volar cortex; if the volar cortex is comminuted, the Kapandji technique is contraindicated as the wires will displace the fragments volarly.

Upon completion of the pinning, the wrist is taken through a gentle range of motion under fluoroscopy to ensure stability of the construct and to confirm that no wires are violating the articular surfaces. The K-wires are bent outside the skin, cut short, and capped to prevent inward migration and to protect the patient from sharp edges. The incisions are closed with simple non-absorbable sutures, and a sterile dressing is applied.
Complications and Management
While percutaneous pinning is minimally invasive, it is not without significant risks. The complications associated with this technique are well-documented, and the surgeon must be prepared to manage them effectively.
Pin tract infection is the most common complication, given the percutaneous nature of the hardware. These are typically superficial and respond well to oral antibiotics and local pin care. Deep infections requiring premature pin removal and surgical debridement are rare but can compromise fracture union.
Neurologic injury, specifically to the superficial branch of the radial nerve, represents a highly morbid complication. Neuroma formation or complex regional pain syndrome (CRPS) can result from direct wire penetration or thermal necrosis during drilling. Meticulous blunt dissection and the use of drill sleeves are the primary preventative measures.
Loss of reduction can occur, particularly if the bone quality was overestimated or if the fracture was highly comminuted. If significant settling occurs, resulting in unacceptable radiographic parameters, revision surgery with internal or external fixation may be required.
Tendon irritation or rupture, particularly of the extensor pollicis longus, can occur if a wire is placed too close to the third dorsal compartment or if it is left protruding excessively on the dorsal cortex.

| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Superficial Pin Tract Infection | 10% - 20% | Prevention: Meticulous sterile technique, regular pin care. Salvage: Oral antibiotics, increased frequency of local care. |
| Superficial Radial Nerve Injury | 2% - 5% | Prevention: Mini-open incision, blunt dissection to bone, use of drill sleeves. Salvage: Gabapentinoids, nerve blocks, surgical exploration for neuroma if refractory. |
| Loss of Reduction / Malunion | 5% - 15% | Prevention: Strict patient selection (avoid in osteoporosis/severe comminution), adequate wire spread. Salvage: Revision ORIF with volar locking plate, corrective osteotomy for established malunion. |
| Tendon Irritation / Rupture | 1% - 3% | Prevention: Avoid multiple passes, protect tendons during insertion, avoid prominent dorsal pins. Salvage: Premature pin removal, tendon transfer (e.g., EIP to EPL) for rupture. |
| Complex Regional Pain Syndrome | 1% - 5% | Prevention: Avoid over-distraction, early finger mobilization, adequate pain control. Salvage: Aggressive hand therapy, sympathetic nerve blocks, multidisciplinary pain management. |
Post Operative Rehabilitation Protocols
The postoperative management following K-wire fixation of the distal radius is designed to protect the fracture during the initial phases of primary bone healing while mitigating the deleterious effects of immobilization on the surrounding joints.
Immediately postoperatively, the patient is placed in a well-padded short arm splint or cast. The wrist is typically immobilized in a neutral position; extreme positions of flexion (the historical Cotton-Loder position) are strictly avoided due to the high risk of median nerve compression and complex regional pain syndrome.
During the immobilization phase, patients are instructed to perform aggressive, active range of motion exercises of the metacarpophalangeal and interphalangeal joints, as well as the elbow and shoulder. Edema control through elevation and compressive dressings is critical. The patient is evaluated in the clinic at one week for radiographic assessment to ensure maintenance of reduction.
Pin care protocols vary by institution, but generally involve daily cleansing of the pin sites with a mixture of normal saline and hydrogen peroxide, followed by the application of sterile gauze.
The K-wires and the cast are typically removed in the outpatient clinic between 4 and 6 weeks postoperatively, contingent upon radiographic evidence of bridging callus and clinical stability. Following pin removal, the patient is transitioned to a removable wrist splint, to be worn during heavy activities and at night.
Formal physical therapy or occupational therapy is initiated immediately upon pin removal. The initial phase focuses on restoring active and active-assisted range of motion of the radiocarpal and distal radioulnar joints. Passive stretching and joint mobilization techniques are introduced gradually. Strengthening exercises, including grip strengthening and progressive resistance exercises for the forearm musculature, are typically delayed until 8 to 10 weeks post-injury, once solid clinical union is achieved. Maximum functional recovery may take up to a year, and patients should be counseled accordingly regarding expectations for terminal range of motion and grip strength.
Summary of Key Literature and Guidelines
The debate regarding the optimal surgical management of distal radius fractures—specifically comparing percutaneous K-wire fixation to open reduction and internal fixation (ORIF) with volar locking plates—has been the subject of extensive orthopedic literature.
The pivotal DRAFFT (Distal Radius Acute Fracture Fixation Trial) study, published by Costa et al. in the BMJ, was a multicenter randomized controlled trial comparing K-wire fixation with volar locking plates for dorsally displaced distal radius fractures in adults. The study concluded that there was no clinically significant difference in patient-rated wrist evaluation (PRWE) scores at 12 months between the two groups. Furthermore, the K-wire cohort demonstrated a significantly lower cost profile and a shorter operative duration. This study robustly supports the continued use of K-wires for reducible fractures where the joint surface can be restored closed.
However, subsequent meta-analyses have nuanced these findings. While functional outcomes at one year may be equivalent, volar locking plates consistently demonstrate superior early functional recovery (within the first 3 months) and a lower incidence of loss of reduction in osteoporotic bone. Therefore, the choice of fixation must be tailored to the individual patient's functional demands and bone quality.
The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines on the Management of Distal Radius Fractures note that rigid internal fixation is recommended for fractures with significant post-reduction instability, articular step-off greater than 2 millimeters, or severe metaphyseal comminution. For fractures that do not meet these criteria of instability, percutaneous pinning remains a highly recommended, evidence-based intervention. The guidelines emphasize that regardless of the fixation method chosen, the primary determinant of long-term functional success is the accurate restoration of anatomic parameters, particularly radial length and volar tilt.
In summary, percutaneous K-wire fixation without external fixation remains a highly effective, biologically friendly, and economically viable surgical strategy. When applied to the appropriate indications with meticulous surgical technique and rigorous postoperative care, it yields excellent clinical outcomes that rival more invasive fixation methods.
Clinical & Radiographic Imaging
You Might Also Like