Restoring the Axis of the Radius: Fixation for Distal Fractures
Key Takeaway
Discover the latest medical recommendations for Restoring the Axis of the Radius: Fixation for Distal Fractures. Distal radius fractures originate in the radial metaphysis, often extending into the radiocarpal or distal radioulnar joints. These common fractures can be stable or unstable, intraarticular or extraarticular, and are frequently dorsally displaced. Understanding surrounding anatomy, such as the dorsal intercarpal ligament with fibers perpendicular to the long axis of the radius, is key to treatment and stability assessment.
Introduction and Epidemiology
Distal radius fractures represent one of the most frequently encountered osseous injuries in orthopedic trauma, accounting for approximately one-sixth of all fractures evaluated in emergency departments. These fractures typically originate in the radial metaphysis and frequently propagate into the radiocarpal joint and the distal radioulnar joint. The injury patterns range from simple, stable extra-articular fractures to highly comminuted, unstable intra-articular disruptions associated with profound ligamentous and soft tissue trauma.
The epidemiological profile of distal radius fractures demonstrates a classic bimodal distribution. The first peak occurs in the pediatric and young adult population, predominantly males, resulting from high-energy trauma such as motor vehicle collisions, falls from significant heights, or athletic injuries. In this demographic, the mechanism often involves substantial axial loading that exceeds the failure strength of dense cortical and trabecular bone, leading to complex intra-articular shear and impaction injuries. The second peak occurs in the elderly population, predominantly postmenopausal females, where low-energy falls from a standing height result in fractures due to underlying osteopenia or osteoporosis.

Pathogenetically, these fractures typically occur due to a fall on an outstretched hand. The specific fracture morphology is dictated by the magnitude of the applied force, the vector of the axial load, and the precise spatial orientation of the carpus at the moment of impact. Dorsally displaced or angulated fractures (apex volar) occur when the wrist is in a neutral or extended position, driving the carpus dorsally against the distal radius. The goals of surgical intervention are to restore articular congruity, re-establish normal anatomic parameters, and provide rigid mechanical stability to facilitate early functional rehabilitation.
Surgical Anatomy and Biomechanics
A profound understanding of the osseous, ligamentous, and tendinous anatomy of the distal radius is paramount for executing safe surgical approaches and achieving anatomic reduction. The distal radius articulates with the proximal carpal row at the scaphoid fossa and the lunate fossa, and with the distal ulna at the sigmoid notch.
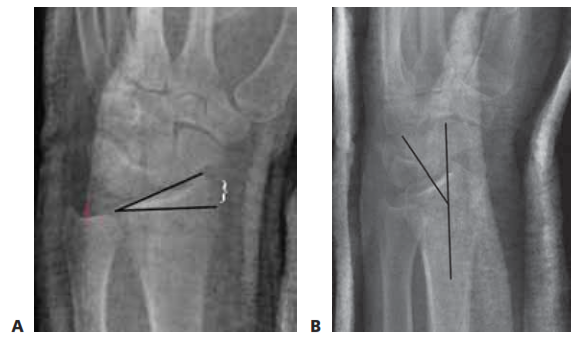
Normal radiographic osseous parameters of the distal radius are critical benchmarks for surgical restoration. The articular surface normally exhibits a volar tilt averaging 10 degrees (range 2 to 20 degrees). Radial height, measured from the tip of the radial styloid to the ulnar articular surface, averages 11 mm. Radial inclination, measured in the coronal plane, averages 22 degrees. Ulnar variance, defining the relative length of the radius to the ulnar head at the sigmoid notch, is highly variable and patient-dependent but must be restored to its pre-injury state to prevent ulnocarpal impaction or distal radioulnar joint incongruity.

The ligamentous architecture stabilizing the radiocarpal and midcarpal joints is complex. Dorsal ligamentous structures include the dorsal intercarpal ligament and the dorsal radiocarpal ligament. The dorsal radiocarpal ligament originates from the dorsal rim of the radius and courses obliquely to attach to the triquetrum and lunate. The dorsal intercarpal ligament functions as a capsular thickening on the dorsum of the carpus, with fiber alignment running perpendicular to the long axis of the radius. Volar ligamentous stabilizers are more robust and include the radioscaphocapitate ligament, the long radiolunate ligament, and the short radiolunate ligament.
The triangular fibrocartilage complex is the primary stabilizer of the distal radioulnar joint. It consists of the central articular disc, the volar and dorsal radioulnar ligaments, the meniscal homologue, the extensor carpi ulnaris subsheath, and the ulnocarpal ligaments. The volar and dorsal radioulnar ligaments originate from the respective edges of the sigmoid notch, become confluent, and insert at the fovea at the base of the ulnar styloid.

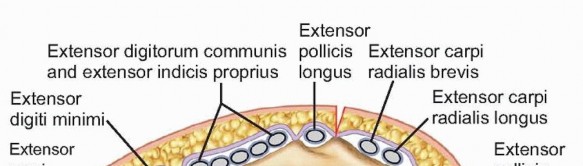
The extensor retinaculum lies superficial to the extensor tendons and deep to the subcutaneous tissues, creating six distinct dorsal compartments through vertical septations. Understanding these compartments is essential for dorsal surgical approaches:
* First Compartment: Contains the abductor pollicis longus and extensor pollicis brevis tendons. It lies over the radial styloid.
* Second Compartment: Contains the extensor carpi radialis longus and extensor carpi radialis brevis tendons.
* Third Compartment: Contains the extensor pollicis longus tendon, which courses around the Lister tubercle.
* Fourth Compartment: Contains the extensor indicis proprius and the extensor digitorum communis tendons, positioned over the dorsal-ulnar aspect of the distal radius.
* Fifth Compartment: Contains the extensor digiti minimi tendon, situated directly over the distal radioulnar joint.
* Sixth Compartment: Contains the extensor carpi ulnaris tendon, lying within a distinct groove on the distal ulna.
Biomechanically, the distal radius transmits approximately 80 percent of the axial load across the wrist joint, with the remaining 20 percent transmitted through the ulnocarpal articulation. Alterations in radial length or volar tilt significantly shift these load-bearing mechanics, predisposing the patient to accelerated post-traumatic arthrosis and functional impairment.
Indications and Contraindications
Treatment algorithms for distal radius fractures are predicated on fracture stability, the degree of comminution, articular segment displacement, and the physiologic age and functional demands of the patient. Stable fractures, which maintain their alignment following closed reduction and immobilization, historically yield excellent outcomes with nonoperative management. However, fractures demonstrating inherent instability require surgical stabilization.
Instability is clinically and radiographically defined by several well-established parameters. The Lafontaine criteria identify primary risk factors for loss of reduction, including initial dorsal angulation greater than 20 degrees, dorsal metaphyseal comminution, intra-articular fracture extension, associated ulnar fracture, and advanced patient age. Additional indicators for operative intervention include radial shortening greater than 5 mm and intra-articular step-off or gap exceeding 2 mm.

While volar locked plating has become highly prevalent, dorsal plating and intramedullary fixation remain critical techniques in the orthopedic armamentarium. Dorsal plating is specifically indicated for fractures with severe dorsal comminution, dorsal shear fractures (Barton fractures), and complex intra-articular patterns where the dorsal articular fragments cannot be adequately reduced or captured from a volar approach. Intramedullary fixation is indicated for extra-articular or simple intra-articular fractures where load-sharing biomechanics and minimal soft tissue disruption are prioritized.
| Indication Category | Operative Management Criteria | Non Operative Management Criteria |
|---|---|---|
| Articular Congruity | Step-off or gap > 2 mm | Step-off or gap < 2 mm |
| Radial Length | Shortening > 5 mm | Shortening < 5 mm |
| Sagittal Alignment | Dorsal tilt > 10 degrees (or volar tilt > 20 degrees) | Neutral to 10 degrees volar tilt |
| Comminution | Severe dorsal or volar metaphyseal comminution | Minimal to no comminution |
| Patient Factors | High functional demand polytrauma open fractures | Low functional demand high surgical risk |
| Associated Injuries | Concomitant carpal fractures or severe soft tissue loss | Isolated stable skeletal injury |
Contraindications to surgical fixation include active local or systemic infection, severe medical comorbidities precluding anesthesia, and non-ambulatory patients with minimal functional demands where the risks of surgery outweigh the functional benefits. Relative contraindications for intramedullary fixation include extremely distal fracture lines lacking adequate metaphyseal bone for distal locking, and narrow medullary canals.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential for successful surgical execution. Standard radiographic evaluation must include posteroanterior, true lateral, and oblique views of the wrist. The true lateral view is critical for assessing volar tilt and dorsal comminution, while the posteroanterior view evaluates radial height, inclination, and ulnar variance.
For complex intra-articular fractures, computed tomography without contrast is strongly recommended. Two-dimensional multiplanar reconstructions and three-dimensional surface rendering provide invaluable information regarding the size, location, and displacement of specific articular fragments (e.g., the radial styloid, dorsal ulnar corner, and volar rim). This dictates the choice of surgical approach and the specific implant required. Digital templating should be performed to anticipate implant size, screw trajectory, and the necessity for supplemental bone grafting or orthobiologics.

Anesthesia may consist of a regional brachial plexus block (supraclavicular or axillary) combined with intravenous sedation, or general anesthesia, depending on patient preference and comorbidities. A regional block provides the added benefit of prolonged postoperative analgesia and potential sympathectomy, which may mitigate the early onset of complex regional pain syndrome.
The patient is positioned supine on the operating table with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The fluoroscopy unit (C-arm) is brought in from the foot of the hand table, parallel to the longitudinal axis of the limb, allowing the surgeon unimpeded access to the surgical field while facilitating orthogonal imaging without moving the fracture site.

The extremity is prepped and draped in a standard sterile fashion. Exsanguination is achieved using an Esmarch bandage, and the tourniquet is inflated to standard pressures (typically 250 mm Hg or 100 mm Hg above systolic blood pressure). Prophylactic intravenous antibiotics are administered prior to tourniquet inflation.
Detailed Surgical Approach and Technique
The surgical management of distal radius fractures via dorsal plating and intramedullary fixation requires meticulous soft tissue handling and precise osseous manipulation. The following sections detail the step-by-step techniques for these specific modalities.
Dorsal Approach to the Wrist
The dorsal approach provides direct visualization of the radiocarpal joint and the dorsal metaphyseal cortex. A longitudinal incision is made centered over the Lister tubercle, extending approximately 5 to 8 cm proximally from the radiocarpal joint. Subcutaneous dissection is carried down to the extensor retinaculum. Care must be taken to identify and protect the terminal branches of the superficial radial nerve radially and the dorsal sensory branch of the ulnar nerve ulnarly.
The third extensor compartment is identified, and the retinaculum is incised longitudinally along the ulnar border of the Lister tubercle. The extensor pollicis longus tendon is mobilized and transposed radially. The Lister tubercle is often excised with a rongeur to create a flat surface for subsequent plate application and to prevent delayed tendon attrition.

Subperiosteal dissection is then utilized to elevate the second compartment (extensor carpi radialis longus and brevis) radially and the fourth compartment (extensor digitorum communis and extensor indicis proprius) ulnarly. This exposes the entire dorsal metaphysis of the distal radius. If visualization of the articular surface is required, a dorsal capsulotomy is performed. A ligament-sparing capsulotomy, such as the Berger approach, is preferred. This involves an incision parallel to the dorsal radiocarpal ligament and the dorsal intercarpal ligament, preserving their structural integrity for later repair.
Fracture Reduction Techniques
Reduction of the distal radius is achieved through a combination of longitudinal traction, ligamentotaxis, and direct manipulation of the fracture fragments. A Freer elevator or a dental pick can be used as a joystick to elevate impacted articular fragments. If a central articular die-punch fragment is present, it must be elevated to restore the articular horizon. The resulting metaphyseal void may be filled with cancellous autograft, allograft, or a synthetic bone substitute to provide subchondral support.
Once provisional reduction is achieved, it is maintained with multiple 0.045-inch or 0.062-inch Kirschner wires. These wires are strategically placed to stabilize the radial styloid, the dorsal ulnar corner, and the volar lunate facet. Fluoroscopic evaluation in both the posteroanterior and true lateral planes confirms the restoration of radial height, inclination, volar tilt, and articular congruity.

Dorsal Plate Fixation Technique
Historically, dorsal plating was associated with a high incidence of extensor tendon tenosynovitis and rupture due to implant prominence. Modern dorsal plates are anatomically contoured, ultra-low-profile, and often utilize fragment-specific designs to minimize soft tissue irritation.
The selected dorsal plate is applied to the reduced radius. Fragment-specific fixation may involve a radial column plate and an intermediate column plate, placed orthogonally or parallel depending on the fracture morphology. The plate is initially provisionally fixed to the diaphysis with a cortical screw in an oblong hole, allowing for proximal-distal adjustment.
Distal locking screws are then inserted into the articular fragments. It is imperative that these screws do not penetrate the radiocarpal or distal radioulnar joints. The dorsal horizon fluoroscopic view (aiming the beam 10 to 15 degrees proximally on the lateral view) is essential to confirm that screws do not protrude past the subchondral bone. Once distal fixation is secure, the proximal diaphyseal screws are placed.

Following definitive fixation, the dorsal capsule is meticulously repaired. The extensor retinaculum is repaired over the second and fourth compartments, leaving the extensor pollicis longus transposed in the subcutaneous tissue to prevent impingement against the hardware.
Intramedullary Fixation Technique
Intramedullary fixation of the distal radius offers the biomechanical advantage of load-sharing and minimizes soft tissue dissection, theoretically reducing the risk of tendon irritation and accelerating recovery. This technique is primarily indicated for extra-articular fractures or simple intra-articular fractures without significant metaphyseal comminution.
A limited 2 to 3 cm incision is made over the first dorsal compartment at the radial styloid. The superficial radial nerve is identified and retracted. The first compartment is opened, and the abductor pollicis longus and extensor pollicis brevis are retracted to expose the radial styloid.
Under fluoroscopic guidance, a starting guidewire is introduced into the tip of the radial styloid, directed proximally and ulnarly down the medullary canal of the radius. The entry point must be precise to avoid violating the radiocarpal joint. A cannulated awl or drill is used to open the cortex.

The fracture is reduced via closed means, and a flexible reamer is passed over the guidewire to prepare the canal. The appropriate sized intramedullary nail is then inserted. The nail is advanced until the distal end is flush with or slightly recessed beneath the cortex of the radial styloid.
Distal locking screws are inserted through a targeting guide. These screws are designed to capture the dorsal and volar cortices of the distal articular block, providing angular stability. Proximal locking screws are subsequently placed through the guide into the radial diaphysis. Final fluoroscopy confirms fracture reduction, hardware placement, and restoration of anatomical parameters. The incisions are irrigated and closed in layers.
Complications and Management
Despite advancements in implant design and surgical technique, surgical fixation of distal radius fractures carries a distinct complication profile. The surgeon must be adept at recognizing and managing these adverse events to optimize patient outcomes.
Extensor tendon complications remain a significant concern, particularly with dorsal plating. Tenosynovitis can progress to spontaneous tendon rupture, with the extensor pollicis longus being the most vulnerable due to its anatomical course and proximity to the hardware. Prophylactic transposition of the extensor pollicis longus and the use of modern low-profile plates mitigate this risk. If rupture occurs, treatment typically involves tendon transfer, most commonly utilizing the extensor indicis proprius.

Intra-articular screw penetration is a severe technical error that leads to rapid chondrolysis and post-traumatic osteoarthritis. This complication is entirely preventable with rigorous intraoperative fluoroscopic evaluation. The surgeon must utilize multiple views, including the 20-degree elevated lateral view and the dorsal horizon view, to ensure screws remain extra-articular. If penetration is identified postoperatively, immediate hardware removal or revision is mandated.
Complex Regional Pain Syndrome (CRPS) is a devastating neuroinflammatory complication characterized by disproportionate pain, hyperalgesia, sudomotor changes, and trophic skin alterations. The incidence is variable but significant. Prevention strategies include meticulous surgical technique, avoidance of excessive traction, and early postoperative mobilization. Some literature supports the perioperative administration of Vitamin C (500 mg daily for 50 days) to reduce the incidence of CRPS, though this remains a topic of academic debate. Management of established CRPS requires a multidisciplinary approach involving aggressive hand therapy, neuropathic pain modulators, and potentially sympathetic nerve blocks.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Strategy / Management |
|---|---|---|---|
| Extensor Tendon Rupture | 1% to 5% | Hardware prominence, direct attrition, devascularization | EIP to EPL tendon transfer, hardware removal |
| Intra-articular Hardware | 2% to 4% | Unrecognized screw protrusion, inadequate fluoroscopy | Immediate surgical revision and screw exchange |
| Complex Regional Pain Syndrome | 5% to 15% | Excessive traction, tight dressings, psychological factors | Multidisciplinary pain management, aggressive hand therapy, sympathetic blocks |
| Loss of Reduction / Malunion | 2% to 10% | Inadequate fixation, severe osteopenia, patient non-compliance | Corrective osteotomy with structural bone grafting and revision fixation |
| Superficial Radial Nerve Neuritis | 3% to 8% | Iatrogenic traction during radial styloid approaches | Observation, gabapentinoids, surgical neurolysis if refractory |
| Infection (Deep) | < 1% | Open fractures, prolonged surgical time, comorbidities | Irrigation and debridement, targeted systemic antibiotics, possible hardware removal |
Loss of reduction and subsequent malunion can occur if the fixation construct is mechanically insufficient to withstand physiological loads, particularly in osteoporotic bone. Malunion typically presents with radial shortening, dorsal angulation, and altered ulnar variance, leading to midcarpal instability and ulnocarpal abutment. Symptomatic malunions require corrective osteotomy. The distal radius is re-osteotomized, realigned to restore volar tilt and length, and stabilized with a robust plate construct, often necessitating an interpositional structural bone graft (autograft or allograft) to fill the resulting metaphyseal defect.
Post Operative Rehabilitation Protocols
The ultimate functional outcome following distal radius fixation is heavily dependent on a structured, progressive rehabilitation protocol. The primary goal of postoperative care is to prevent stiffness in the digits, wrist, and adjacent joints while protecting the surgical fixation.
Phase 1 (0 to 2 weeks postoperatively) focuses on edema control and immediate digital mobilization. The patient is placed in a bulky soft dressing and a volar orthosis. Active range of motion of the metacarpophalangeal and interphalangeal joints is initiated immediately. Patients are instructed to perform full composite fist exercises multiple times a day to facilitate tendon gliding and reduce swelling. Elevation of the extremity above the level of the heart is strictly enforced. Shoulder and elbow range of motion exercises are also mandated to prevent proximal stiffness.
Phase 2 (2 to 6 weeks postoperatively) begins at the first postoperative visit. Sutures are removed, and the patient is transitioned to a custom-molded, removable thermoplastic splint. Depending on the rigidity of the fixation and the bone quality, active and active-assisted range of motion of the radiocarpal and distal radioulnar joints is initiated. Flexion, extension, pronation, and supination are performed within a pain-free arc. The splint is worn between exercise sessions and at night. Passive stretching is generally avoided during this phase to prevent stress on the healing fracture.
Phase 3 (6 to 12 weeks postoperatively) marks the transition to strengthening and functional use. Radiographic evaluation is performed to confirm progressive osseous union. Once clinical and radiographic healing is evident, the splint is discontinued. Progressive resistive exercises are introduced, utilizing putty, hand grippers, and light weights. Proprioceptive training and weight-bearing exercises are gradually incorporated.
Return to heavy manual labor or contact sports is typically permitted between 3 and 6 months postoperatively, contingent upon the restoration of near-normal grip strength, full range of motion, and complete radiographic consolidation. Patients must be counseled that maximal medical improvement may not be reached until 12 to 18 months following the injury, and mild residual deficits in terminal flexion or supination are not uncommon.
Summary of Key Literature and Guidelines
The surgical management of distal radius fractures is supported by a robust body of orthopedic literature and established clinical practice guidelines. The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines provide evidence-based recommendations for the treatment of these injuries. The guidelines strongly support operative fixation for fractures with post-reduction radial shortening greater than 3 mm, dorsal tilt greater than 10 degrees, or intra-articular displacement or step-off greater than 2 mm.
Landmark biomechanical studies have elucidated the critical importance of restoring anatomical parameters. Shortening of the radius by as little as 2 mm has been shown to significantly alter the load distribution at the distal radioulnar joint, leading to increased forces on the triangular fibrocartilage complex and the ulnar head. Similarly, residual dorsal tilt alters the contact mechanics of the radiocarpal joint, concentrating forces on the dorsal aspect of the scaphoid and lunate fossae, accelerating degenerative changes.
The debate regarding the optimal fixation modality—volar plating, dorsal plating, or intramedullary nailing—remains a prominent topic in orthopedic literature. While volar plating has become the most widely utilized technique due to its favorable soft tissue envelope and ability to buttress the volar cortex, dorsal plating remains indispensable for specific fracture patterns. Recent prospective cohort studies evaluating modern, low-profile, fragment-specific dorsal plates have demonstrated functional outcomes and complication rates comparable to volar plating, effectively neutralizing the historical stigma associated with dorsal hardware prominence.
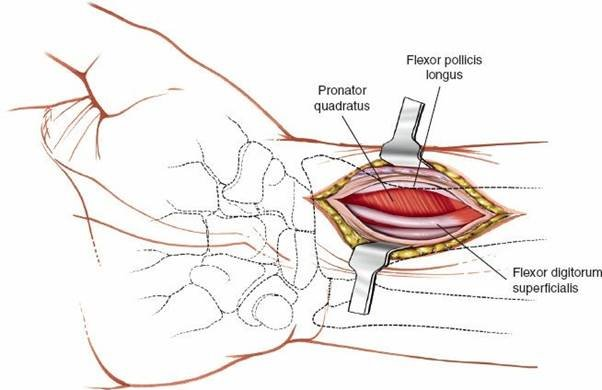
Intramedullary fixation has been extensively studied in the context of extra-articular and simple intra-articular fractures. Randomized controlled trials comparing intramedullary nailing to volar locked plating have shown that intramedullary fixation yields equivalent clinical and radiographic outcomes at one year. However, intramedullary nailing often demonstrates superior early functional scores (at 3 to 6 weeks) and a faster return to work, likely attributable to the minimally invasive approach and preservation of the pronator quadratus and volar soft tissues.
In the elderly demographic, the literature presents a more nuanced perspective. Several high-quality randomized trials, including the prominent study by Arora et al., have demonstrated that while surgical fixation in patients over the age of 65 provides superior radiographic restoration compared to cast immobilization, this does not consistently translate into superior long-term functional outcomes as measured by the Disabilities of the Arm, Shoulder and Hand (DASH) or Patient-Rated Wrist Evaluation (PRWE) scores. Therefore, the decision to operate on an elderly patient must be highly individualized, carefully weighing the patient's functional demands, medical comorbidities, and the inherent risks of surgical intervention against the predictable outcomes of nonoperative management.
Clinical & Radiographic Imaging
You Might Also Like